
Abstract
Contrast-induced acute kidney injury (CI-AKI) is a serious complication of percutaneous coronary intervention (PCI) in patients with acute ST-segment elevation myocardial infarction (STEMI). Early identification of high-risk patients has an essential role in preventing CI-AKI. This study was designed to evaluate the predictive value of
Keywords
Introduction
Acute ST-segment elevation myocardial infarction (STEMI) is one of the leading causes of death globally. Early restoration of coronary antegrade flow by percutaneous coronary intervention (PCI) plays a critical role in improving the prognosis of patients with STEMI. Contrast-induced acute kidney injury (CI-AKI) is defined as acute renal damage that develops secondary to contrast media exposure and is the third leading cause of in-hospital acute kidney injury.
1
Contrast-induced acute kidney injury occurs frequently in patients with STEMI undergoing PCI due to hemodynamic instability and inadequate prophylaxis
2,3
and is related to long-term morbidity and mortality.
4
–6
Vascular endothelial dysfunction, vasoconstriction, inflammation, free radical damage, tubular cell toxicity, reactive oxygen species, and oxidative stress have been proposed as pathophysiological mechanisms of CI-AKI.
7
At present, there are no operative prophylactic–therapeutic measures for CI-AKI.
8
Therefore, early identification of high-risk groups and active intervention are essential to prevent CI-AKI.
Methods
Study Population
This is a retrospective observational cohort study. From December 2013 to January 2017, consecutive patients with STEMI admitted to Zhongda Hospital and treated with PCI were enrolled. The inclusion criteria were as follows: (1) age between 18 and 80 years old and (2) patients with STEMI who were diagnosed based on the Guidelines for the Diagnosis and Treatment of Acute ST-segment Elevation Myocardial Infarction in 2015 17 and underwent PCI. The exclusion criteria were as follows: (1) allergy to iodine or iodine contrast medium, (2) end-stage renal failure requiring peritoneal dialysis, hemodialysis, and kidney transplantation, (3) severe cardiac insufficiency and valvular heart disease with unstable hemodynamics, (4) definite bacterial and fungal infections, acute and chronic inflammatory diseases, autoimmune diseases, or tumors, (5) antibiotics use before admission, (6) contrast medium administration within 2 weeks before admission, and (7) nephrotoxic drug application during hospitalization. The study was approved by the medical ethics committee of Zhongda Hospital, and all methods were performed in accordance with the relevant guidelines and regulations. All patients included volunteered to participate in this clinical study and signed an informed consent form.
Grouping
The patients were divided into 4 groups according to
Laboratory Investigations
Serum creatinine (SCr) concentration was measured before and 2 to 3 days after contrast media exposure. Renal function was measured using the estimated glomerular filtration rate (eGFR) with the modified MDRD formula (eGFR = 175 × creatinine−1.234 × age−0.179 × [0.79 (female)]) according to data from Chinese patients with CKD. Plasma
Coronary Angiography
All patients were given aspirin (300 mg), ticagrelor (180 mg), or clopidogrel (300 mg) before the operation. Selective coronary arteriography was performed by cardiologists specializing in interventional treatments. The corresponding diseased vessels were treated according to the specific results of the coronary angiography. Nonionic and low-osmotic contrast agents (Iopromide injection, Bayer Vital GmbH) were used during the operation, and the amounts were recorded.
Percutaneous Coronary Intervention
Percutaneous coronary intervention included balloon dilation and/or stent implantation for infarct-related vessels and was performed by experienced operators according to standard techniques. Hydration therapy was given to patients with an eGFR <60 mL/min/1.73 m2 and consisted of intravenous administration of isotonic saline (1.0-1.5 mL/kg/h) at 3 to 12 hours before the operation and 6 to 24 hours after the operation. Isotonic saline solution was intravenously given at 0.5 mL/kg/h if left ventricular ejection fraction (LVEF) <35% or NYHA >2. Aspirin (100 mg, one daily), ticagrelor (90 mg, twice daily), or clopidogrel (75 mg, once daily) were administered after surgery. Statins, β-blockers, nitrates, and angiotensin-converting enzyme inhibitors were commonly used in all patients without contraindications.
Study Protocol: End Points and Follow-Up
The primary end point was CI-AKI. Contrast-induced acute kidney injury was defined as a rise in SCr of 44.2 μmol/L or a 25% increase from the baseline value within 2 to 3 days after contrast media exposure. 18 The secondary end points were the main adverse cardiovascular and cerebrovascular events (MACCEs) and hospitalization for kidney failure during the follow-up period (30 days, 6 months, 1 year after PCI). The MACCEs included all-cause death, target vessel revascularization, myocardial infarction during follow-up, unstable angina pectoris requiring hospitalization, heart failure, stroke, or transient cerebral ischemia. Each patient’s baseline clinical data (including demographic data, previous medical history, and vital signs on admission), biochemical and angiographic variables, and echocardiography results were recorded. The patients made a follow-up visit 30 days, 6 months, and 1 year after the operation. Follow-up data were obtained from hospital records or via interviews (in person or by telephone) with patients and their families conducted by at least 2 cardiologists.
Statistical Analysis
Analyses were performed using SPSS software, version 16.0 (SPSS, Inc). Continuous variables are expressed as the means ± SDs or medians (interquartile ranges). Categorical variables are expressed as frequencies with percentages. Univariable and multivariable logistic regression analyses were used to determine CI-AKI predictors. Variables with univariable P values <.10 were selected for multivariable analysis and expressed as odds ratios (ORs) with 95% CIs. Survival was graphically represented using Kaplan-Meier curves. Differences in survival rates were compared using the log-rank test. The area under the receiver operating characteristic (ROC) curves (AUCs) were used to indicate the predictive value of
Results
Patient Characteristics
This study included 400 patients with STEMI who underwent PCI, and CI-AKI occurred in 66 (16.5%) patients. All patients were subdivided into 4 groups according to
Baseline Clinical Data and Therapy at Admission of the 4 Groups.a

Abbreviations: ACEI, angiotensin-converting enzyme inhibitor; AMI, acute myocardial infarction; ARB, angiotensin receptor blocker; CI-AKI, contrast induced acute kidney injury; SBP, systolic blood pressure.
a Data are presented as the mean ± SD or n (%).
Biochemical and Angiographic Variables of the 4 Groups.a

Abbreviations: eGFR, estimated glomerular filtration rate; HDL-C, high-density lipoprotein cholesterol; IQR, interquartile range; LDL-C, low-density lipoprotein cholesterol; LVEF, left ventricular ejection fraction; NT-proBNP, NT-proB-type natriuretic peptide; SCr, serum creatinine concentration; TC, total cholesterol.
a Data are presented as the IQR, mean ± SD, or n (%).
Risk Factors for CI-AKI
Baseline clinical data and therapy at admission of the CI-AKI and non-CI-AKI groups are given in Table 3. The biochemical and angiographic variables and echocardiography results of the CI-AKI and non-CI-AKI groups are shown in Table 4. The proportions of females (31.8% vs 18.9%, P, .018), diabetes mellitus (47.0% vs 21.0%, P < .001), and anemia (31.8% vs 9.0%, P < .001) in the CI-AKI group were higher than those in the non-CI-AKI group. There were statistically significant differences (P < .05) between the CI-AKI and non-CI-AKI groups in terms of
Baseline Clinical Data and Therapy at Admission of the CI-AKI and Non-CI-AKI Groups.a
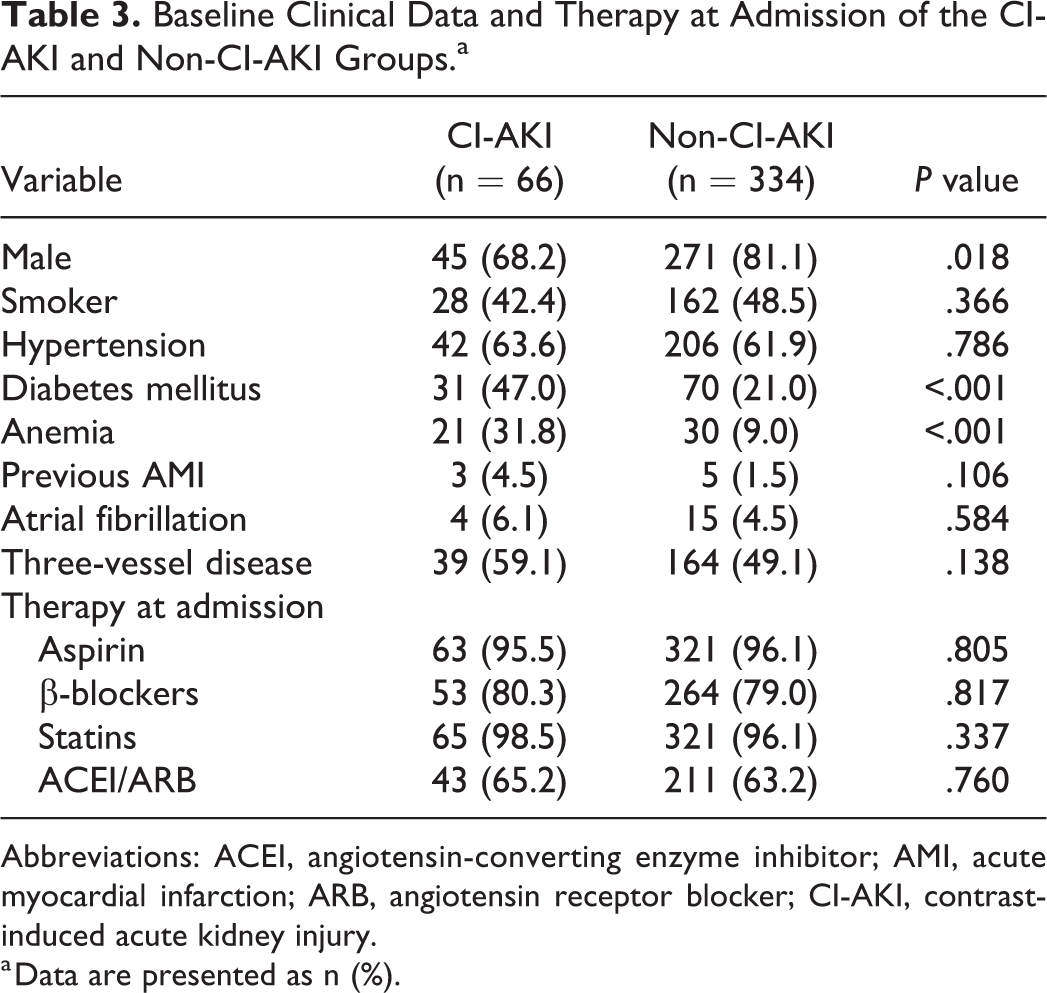
Abbreviations: ACEI, angiotensin-converting enzyme inhibitor; AMI, acute myocardial infarction; ARB, angiotensin receptor blocker; CI-AKI, contrast-induced acute kidney injury.
a Data are presented as n (%).
Biochemical and Angiographic Variables of the CI-AKI and Non-CI-AKI Groups.a

Abbreviations: CI-AKI, contrast-induced acute kidney injury; eGFR, estimated glomerular filtration rate; HDL-C, high-density lipoprotein cholesterol; IQR, interquartile range; LDL-C, low-density lipoprotein cholesterol; LVEF, left ventricular ejection fraction; NT-proBNP, NT-proB-type natriuretic peptide; SBP, systolic blood pressure; SCr, serum creatinine concentration; TC, total cholesterol.
a Data are presented as the IQR or mean ± SD.
Univariable and multivariable analyses and predictors for CI-AKI are presented in Table 5. Univariable logistic regression showed that
Univariable and Multivariable Analysis and Predictors for CI-AKI.
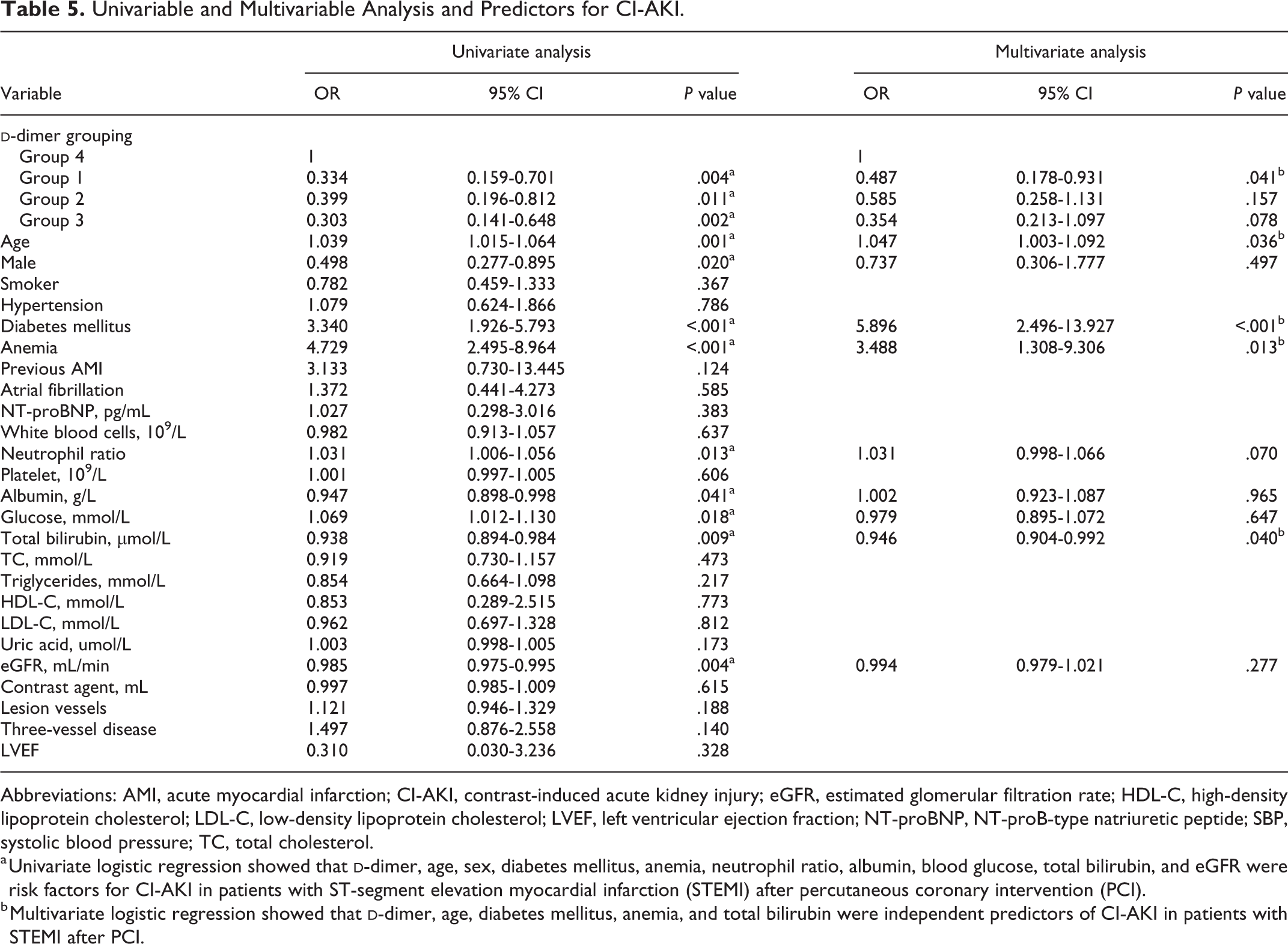
Abbreviations: AMI, acute myocardial infarction; CI-AKI, contrast-induced acute kidney injury; eGFR, estimated glomerular filtration rate; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; LVEF, left ventricular ejection fraction; NT-proBNP, NT-proB-type natriuretic peptide; SBP, systolic blood pressure; TC, total cholesterol.
a Univariate logistic regression showed that
b Multivariate logistic regression showed that
The ROC curves for

Receiver operating characteristic (ROC) curves for
The occurrence of MACCE in each
MACCE Occurrence in Each

Abbreviations: MACCEs, main adverse cardiac and cerebrovascular events; PCI, percutaneous coronary intervention.
a Data are presented as n (%).
b The incidence of MACCE within 30 days, 6 months, and 1 year after PCI in group 4 were higher than that in the other 3 groups.
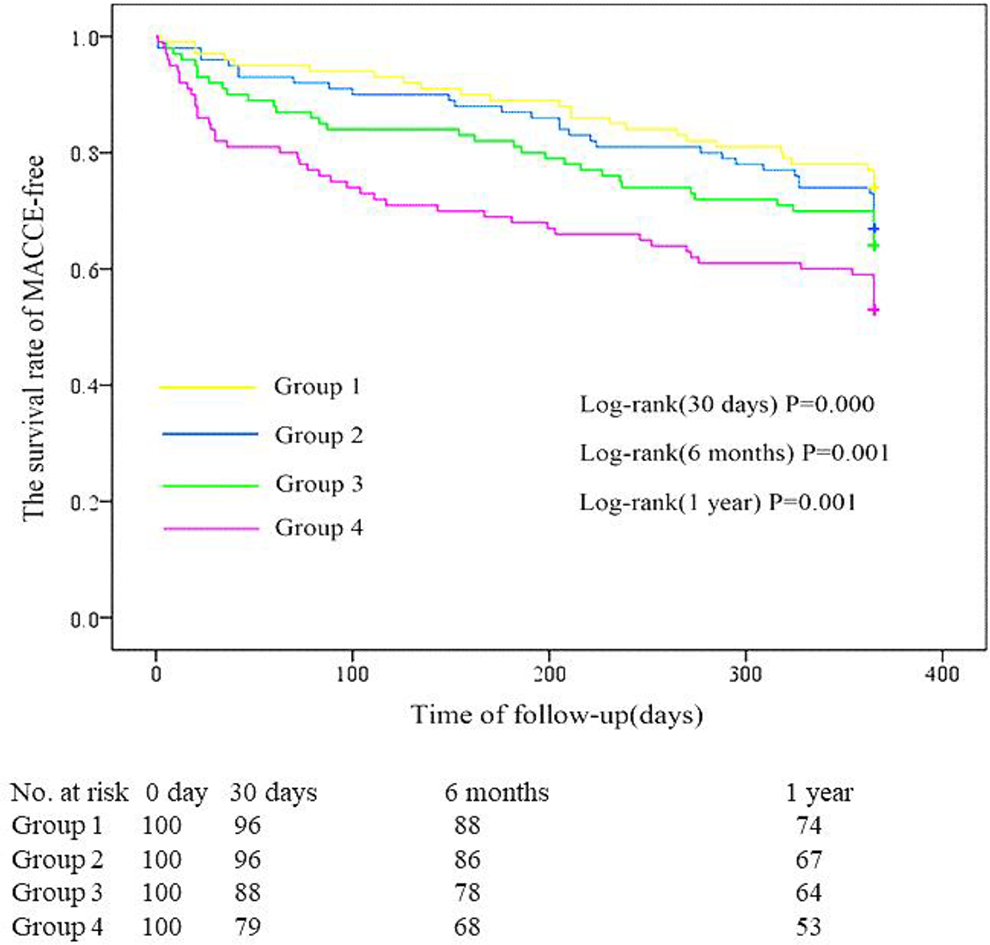
Survival curves for follow-up without an main adverse cardiovascular and cerebrovascular event (MACCE-free) for the 4 groups. The incidence of MACCEs within 30 days, 6 months, and 1 year after percutaneous coronary intervention (PCI) in group 4 were higher than that in the other 3 groups (P < .01).

Cumulative probability of the overall survival for the 4 groups at the 1-year follow-up. The incidence of all-cause mortality within 30 days, 6 months, and 1 year after percutaneous coronary intervention (PCI) in group 4 were higher than that in the other 3 groups (P < 0.01).
Hospitalization for Kidney Failure in Each

Abbreviation: PCI, percutaneous coronary intervention.
a Data are presented as n (%).
b The incidence of hospitalization for kidney failure within 6 months and 1 year after PCI in group 4 were higher than that in the other 3 groups (P < .05).
Discussion
Contrast-induced acute kidney injury is characterized by acute impairment of renal function following exposure to contrast agents, 19 is an independent predictor of worse outcomes, and is significantly associated with long-term mortality. 20 Previous studies have shown that congestive heart failure, chronic renal insufficiency, diabetes mellitus, intravascular volume depletion, and the use of a large amount of contrast agent were considered important predisposing factors. 21 The diagnosis of CI-AKI has traditionally relied on SCr, which is a delayed indicator of CI-AKI. 22 Early identification of high-risk groups and active intervention are indispensable to prevent CI-AKI.
Several risk scores and risk factors have been established for the prediction of CI-AKI, but none is recommended for use in daily practice due to a lack of sufficient verification in the literature. 7,23 Advances in biomarkers for predicting CI-AKI have been made recently. Neutrophil gelatinase-associated lipocalin has been strongly correlated with SCr levels and have been considered in the diagnosis of CI-AKI. 24 Cystatin C levels have been shown to be a more accurate early marker of GFR reduction and were less influenced by nonrenal variables than SCr levels. 25,26 Procalcitonin, a novel marker of systemic inflammatory conditions, has been recently demonstrated to predict CI-AKI in patients with ACS. 27 Unfortunately, although such biomarkers are promising, no standard cutoffs for the diagnosis of CI-AKI have been established, and existing data on clinical outcomes are inadequate.
This study showed that
The prognostic value of
Study Limitations
The following limitations of the present study should be addressed. First, this study was not a standard randomized controlled trial. There was a selection bias, and whether these defects will affect the results also requires a prospective study with larger samples. Second, it was more reasonable to measure
Conclusion
In conclusion, the current study demonstrated that higher
Footnotes
Authors’ Note
Erfei Luo and Dong Wang contributed equally to this work and should be considered co-first authors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by grants to Chengchun Tang and Dong Wang from the National Natural Science Foundation of China (Research Grant #81670237 and 81800244).