
Abstract
A new scoring system Outcomes Registry for Better Informed Treatment (ORBIT) score is used to assess the bleeding risk in anticoagulated patients with atrial fibrillation (AF). Our aim is to investigate the possible correlations of the ORBIT score with 30-day mortality in patients with ST-segment elevation myocardial infarction (STEMI). A total of 639 patients with STEMI were enrolled in this study. The ORBIT, HAS-BLED, and TIMI scores were recorded during admission. After 30 days’ follow-up, 639 patients were divided into 2 groups: the survival group and the nonsurvival group. Different clinical parameters were compared. The predictive values of the ORBIT, HAS-BLED, and TIMI scores for 30-day mortality were assessed from receiver operating characteristic (ROC) analyses. The univariate and multivariate Cox proportional hazards analyses were applied to evaluate the relationships between variables and 30-day mortality. Sixty-seven deaths occurred after a 30-day follow-up. The ORBIT, HAS-BLED, and TIMI scores in the death group were higher than those in the survival group (P < .05). The areas under the ROC curve for the ORBIT, HAS-BLED, and TIMI scores to predict the occurrence of 30-day mortality were 0.811 (95% CI: 0.779-0.841, P < .0001), 0.717 (95% CI: 0.680-0.752, P < .0001), and 0.844 (95% CI: 0.813-0.871, P < .0001), respectively. In multivariate Cox proportional hazards modeling, the high ORBIT score was positively associated with 30-day mortality (hazard ratio: 1.309, 95% CI: 1.101-1.556, P = .013) after adjustment. A graded relation is found in the elevated ORBIT score and 30-day mortality in patients with STEMI. Thus, the ORBIT score can be an independent predictor of 30-day mortality in patients with STEMI.
Introduction
The mortality of patients with ST-segment elevation myocardial infarction (STEMI) is high during hospitalization. Currently, the TIMI score is recommended by the guideline to be a superior scoring system for the early risk stratification of STEMI. The TIMI score shows a good predictive value for the short-term and long-term prognosis for STEMI. 1,2 The Outcomes Registry for Better Informed Treatment (ORBIT) score, similar to the HAS-BLED scoring system, is used to assess the risk of bleeding in anticoagulant therapy for atrial fibrillation (AF). 3 The scoring elements include older age, hemoglobin decline, low hematocrit value or previous anemia, and renal insufficiency. No study is available about the ORBIT score and short-term prognosis for patients with STEMI. Therefore, our study aimed to explore the predictive value of the ORBIT score in the 30-day mortality among patients with STEMI.
Materials and Methods
Study Population
This is a retrospective study. A total of 639 patients with STEMI admitted to the Second Affiliated Hospital of Nantong University from January 2017 to June 2017 were enrolled in this study, including 507 males and 132 females. The average age is 66.51 ± 12.91 years old. The diagnosis of STEMI was based on the presence of characteristic symptoms of myocardial ischemia, appropriate electrocardiographic changes, and elevation in biomarkers of myocardial necrosis. 4 Age, sex, blood pressure, heart rate, past concomitant diseases (eg, hypertension, hyperlipidemia, diabetes, stroke, renal insufficiency, past myocardial infarction, bleeding history), current smokers, in-hospital medications, Killip class, timely percutaneous coronary intervention (PCI), and the ORBIT, HAS-BED, and TIMI scores of all patients were recorded after admission. Troponin I, serum creatinine, and blood routine were immediately detected at admission. Moreover, fasting venous blood samples were collected in the next morning after admission, and the levels of total cholesterol, triglyceride, high-density lipoprotein cholesterol, low-density lipoprotein cholesterol, and N-terminal pro-brain natriuretic peptide (NT-proBNP) were measured. The exclusion criteria were as follows: blood diseases, active bleeding, malignancies, acute infectious disease, chronic rheumatic immunological diseases, and a recent history of infection, surgery, or blood transfusion.
The ORBIT Score
The ORBIT score 3 was developed from the ORBIT registry and calculated as follows: 1 point each for age ≥75 years, insufficient kidney function (glomerular filtration rate <60 mL/min/1.73 m2), and treatment with any antiplatelet; 2 points were assigned to bleeding history and reduced hemoglobin/anemia (<13 mg/dL for males and<12 mg/dL for females or hematocrit <40% for males and <36% for females).
Study End Points
The primary end point was all-cause mortality within 30 days.
Statistical Analysis
The measurement data were presented as means ± SD, while those conforming to skewed distribution were expressed as M (P25-P75). The enumeration data were presented as percentage or frequency. The independent-samples t test, Mann-Whitney U test, and the χ2 test were applied in comparing the measurement and enumeration data of the 2 groups, respectively. The predictive values of the ORBIT, HAS-BLED, and TIMI scores on the 30-day mortality were completed via receiver operating characteristic (ROC) analyses. Univariate and multivariate Cox proportional hazards analyses were used to evaluate the relationship between variables and 30-day mortality. Variables that had a P value <.1 in the univariate analysis were used in a multivariable Cox proportional hazards model to determine the independent prognostic factors for 30-day mortality. Data were analyzed using MedCalc (version 11.2.1; MedCalc) and SPSS 17.0 (SPSS Inc). P < .05 was deemed as statistically significant.
Results
Comparison of Baseline Data of 2 Groups
Age, female, Killip class ≥II, heart rate, serum creatinine, NT-proBNP, and the ORBIT, HAS-BLED, and TIMI scores in the nonsurvivor group were higher than those in the survivor group (P < .05). The systolic blood pressure, timely PCI, angiotensin-converting enzyme inhibitor (ACEI)/angiotensin receptor blocker (ARB), and β-blockers use in the nonsurvivor group were lower than those in the survivor group (Table 1).
Comparison of the General Clinical Information Between the 2 Groups.
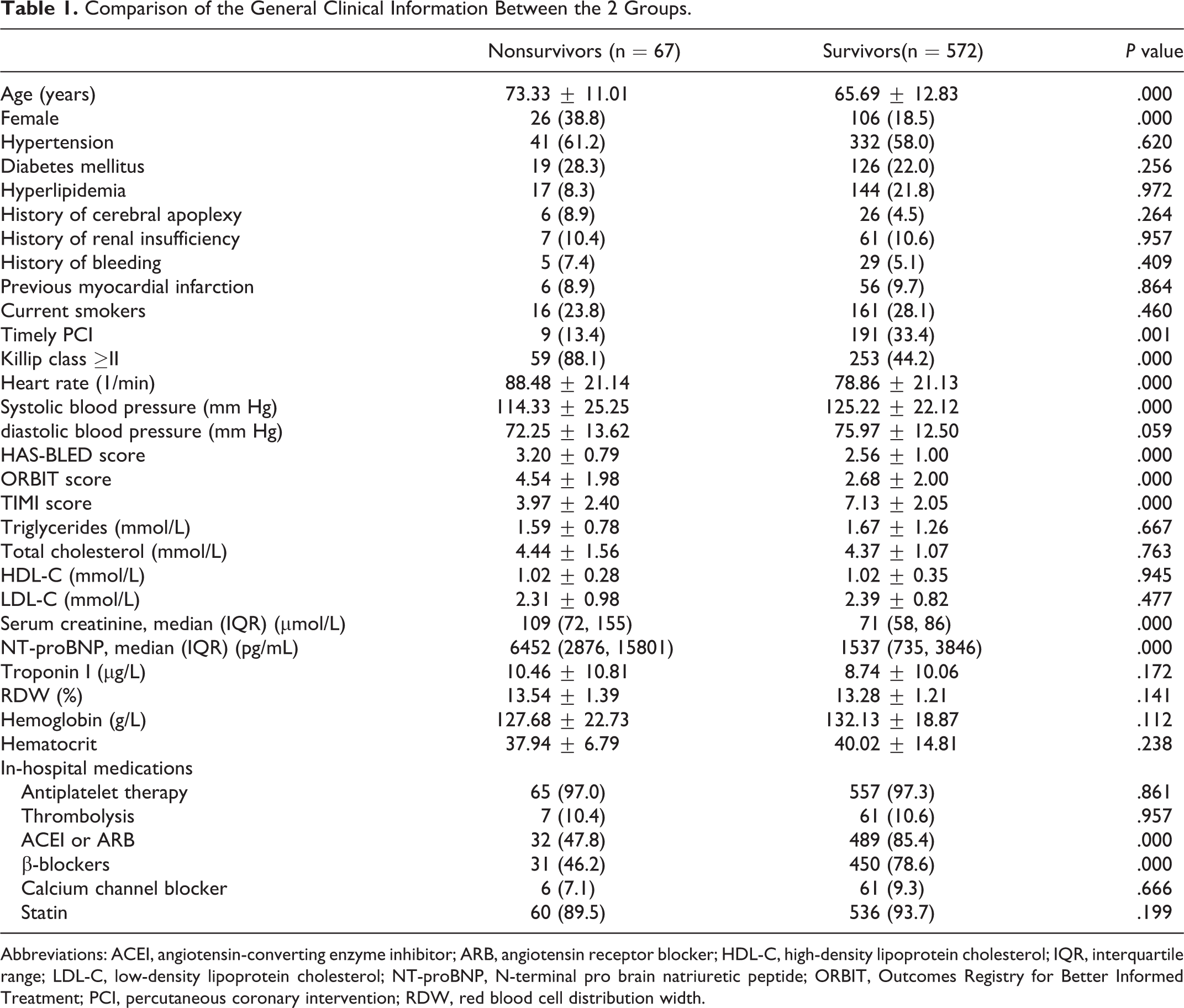
Abbreviations: ACEI, angiotensin-converting enzyme inhibitor; ARB, angiotensin receptor blocker; HDL-C, high-density lipoprotein cholesterol; IQR, interquartile range; LDL-C, low-density lipoprotein cholesterol; NT-proBNP, N-terminal pro brain natriuretic peptide; ORBIT, Outcomes Registry for Better Informed Treatment; PCI, percutaneous coronary intervention; RDW, red blood cell distribution width.
The area under the ROC curve of the ORBIT score to predict 30-day Mortality was 0.811, with a cutoff level of 3 (95% CI: 0.779-0.841) and 74.6% sensitivity and 69.3% specificity (P < .0001). The area under the ROC curve of the HAS-BLED score to predict 30-day mortality was 0.717, with a cutoff level of 2 (95% CI: 0.680-0.752) and 85.1% sensitivity and 51.5% specificity (P < .0001). The area under the ROC curve of TIMI score to predict 30-day mortality was 0.844, with a cutoff level of 4 (95% CI: 0.813-0.871) and 91.0% sensitivity and 61.6% specificity (P < .0001; Figure 1).
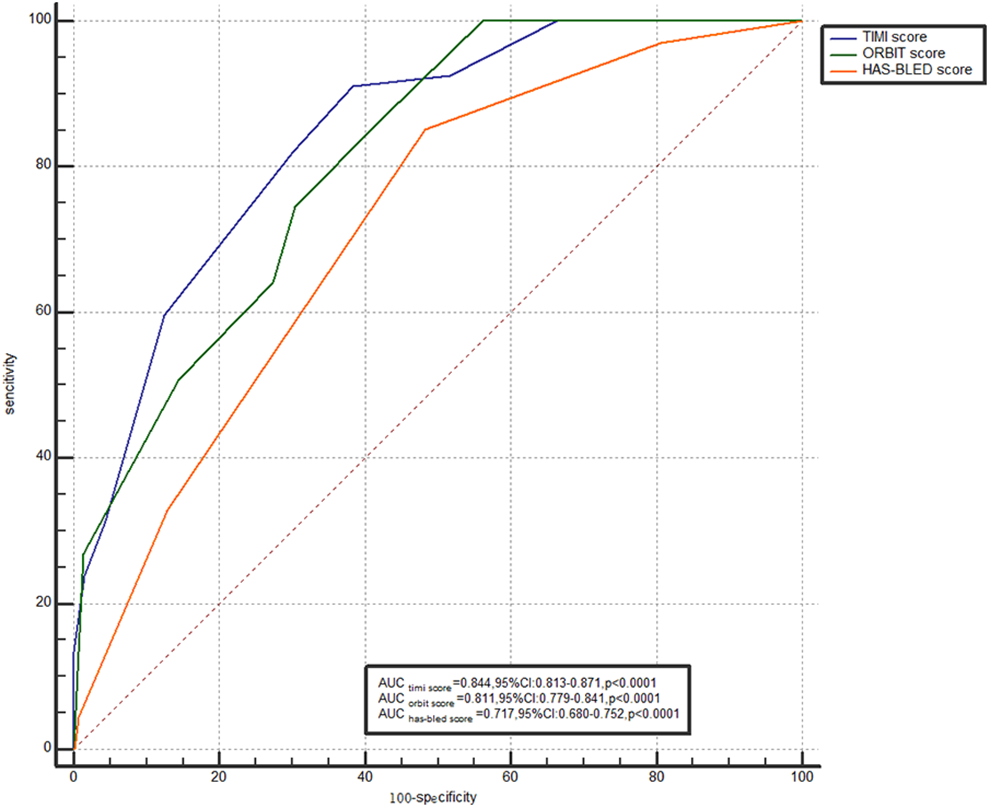
The area under the receiver operating characteristic (ROC) curve.
Variables that had a P value <.1 in the univariate analyses were used in a multivariable Cox proportional hazards model. After forward stepwise multivariate analyses variables for inclusion in the multivariate analyses were age, female, Killip class ≥II, heart rate, systolic pressure, diastolic pressure, timely PCI, the ORBIT, HAS-BLED, and TIMI scores, serum creatinine, NT-proBNP, ACEI/ARB, and β-blockers usage. In multivariate Cox proportional hazards modeling, the high ORBIT score was significantly associated with an increased incidence of 30-day mortality (hazard ratio [HR]: 1.309, 95% CI: 1.101-1.556, P = .013) after adjustment. Other predictors of 30-day mortality were the TIMI score (HR: 1.352, 95% CI: 1.068-1.712, P = .002), heart rate (HR: 1.027, 95% CI: 1.011-1.042, P = .000), and ACEI/ARB usage (HR: 0.316, 95% CI: 0.165-0.605, P = .000; Table 2).
Results of Multivariate Analyses for 30-Day Mortality.
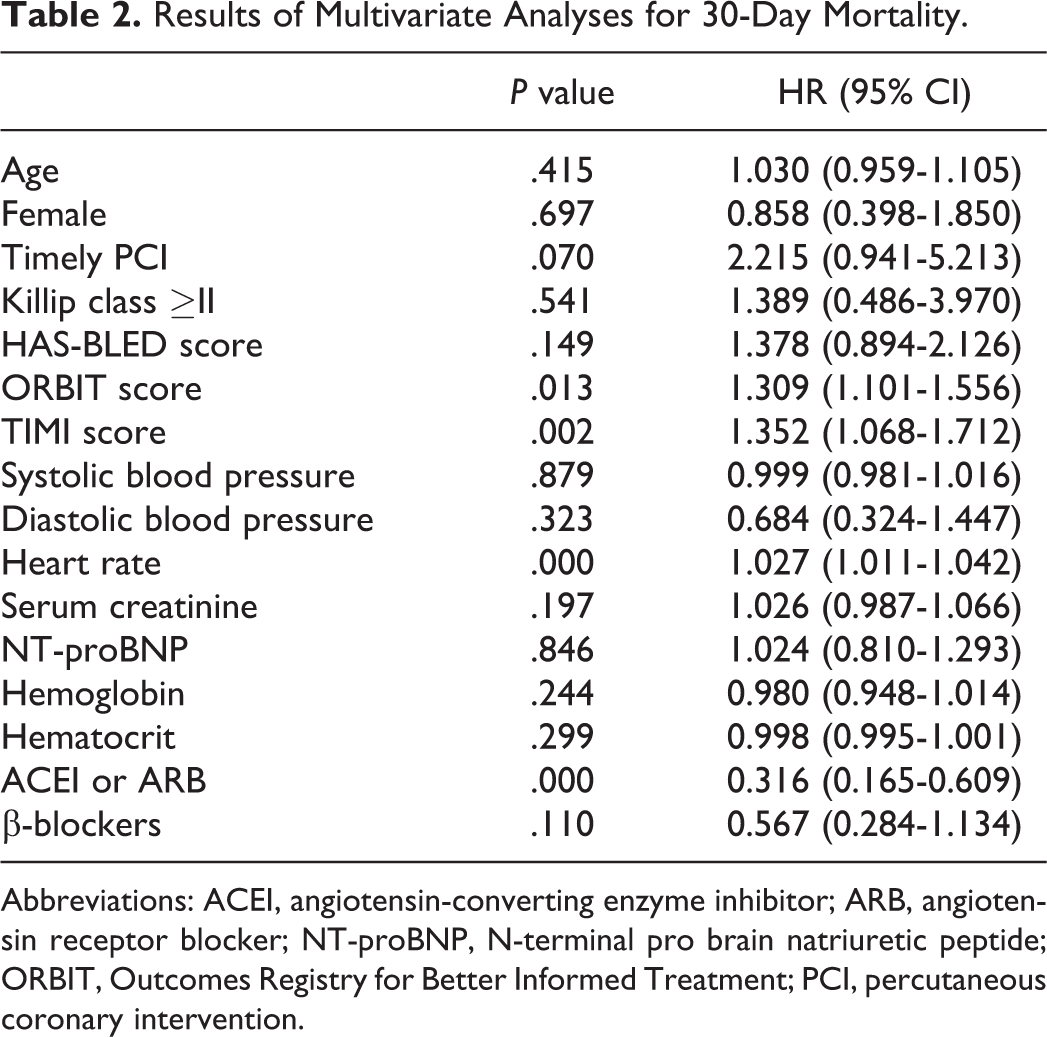
Abbreviations: ACEI, angiotensin-converting enzyme inhibitor; ARB, angiotensin receptor blocker; NT-proBNP, N-terminal pro brain natriuretic peptide; ORBIT, Outcomes Registry for Better Informed Treatment; PCI, percutaneous coronary intervention.
Discussion
The main findings of our study were as follows. (1) The ORBIT score in the death group was higher than those in the nondeath group. (2) Patients with STEMI had an increased risk of death for 30 days when the ORBIT score was above 3 points. (3) The high ORBIT score is an independent predictor of 30-day mortality in patients with STEMI.
The TIMI score has been recommended by guideline to be used for the early risk stratification for patients with STEMI, which displays favorable predictive value for the 30-day prognosis for patients with acute myocardial infarction (AMI). The AF treatment guideline from the European Society of Cardiology in 2010 has first proposed the AF anticoagulation bleeding risk assessment system, the HAS-BLED scoring system, which is the most extensively applied scoring system in clinic. 5 Researches have shown that the HAS-BLED score can be used to evaluate the bleeding risk in patients with acute coronary syndrome (ACS) combined with AF when receiving oral anticoagulants treatment. 6,7 Hsieh et al 8 and Capodanno et al 9 discovered that the HAS-BLED score can also be employed to predict the prognosis of non-AF patients receiving PCI treatment. O’Brien et al had studied 7411 patients with AF receiving oral anticoagulants from 176 centers from 2010 to 2012 and obtained a novel scoring system, namely, the ORBIT scoring system. Similarly, such novel scoring system is also used to assess the bleeding risk in anticoagulant therapy for AF. However, no study is available on the ORBIT scoring system with the prognosis of patients with STEMI. Our study observed that the TIMI, ORBIT, and HAS-BLED scores in the death group are higher than those in the nondeath group. Meanwhile, the TIMI and ORBIT scores are markedly superior to HAS-BLED score in predicting the death event within 30 days for patients with STEMI. No obvious difference is seen in the predictive value between the TIMI and ORBIT scores on death event, but the TIMI score is more sensitive. In addition, multivariate analysis suggests that the ORBIT score can serve as an independent predictor of 30-day mortality in patients with STEMI. Specifically, the risk of 30-day mortality will increase by 1.309-fold with the increase of 1 point in the ORBIT score. Consistent with previous research conclusion, the TIMI score is also the independent predictor of 30-day mortality (HR: 1.352, 95% CI: 1.068-1.712, P = .002). In addition, this study also demonstrated that the increased heart rate is an independent predictor of 30-day mortality (HR: 1.027, 95% CI: 1.011-1.042, P = .000), and ACEI/ARB usage is a protective factor (HR: 0.316, 95% CI: 0.165-0.609, P = .000).
The ORBIT scoring system is comprised of 5 elements, including older age, hemoglobin decline, low hematocrit value or previous anemia, and renal insufficiency. Multiple clinical studies indicate that renal function is closely correlated with the prognosis of AMI. The poorer renal function is associated with a higher incidence of cardiovascular events and more dismal prognosis. Al Suwaidi et al 10 suggested that patients with ACS frequently develop abnormal renal function. Besides, abnormal renal function is the predictor of dismal prognosis, which is related to the increased mortality. A study observed that acute renal injury (AKI) strongly correlated with short-term and long-term all-cause mortality in patients with AMI regardless of baseline renal function. 11 Moriyama et al 12 discovered that early AKI is an independent predictor of in-hospital mortality in patients with AMI. Notably, patients with early AKI were associated with high mortality even when their renal functions had recovered to baseline level. Similarly, age is also related to the dismal prognosis of AMI. Goldberg et al suggested that age is related to the short-term and long-term prognosis of AMI. 13 Champney et al discovered that age is correlated with short-term mortality induced by different sexes, either for STEMI or non-STEMI patients. 14 Gao et al suggested that age strongly influenced the association between sex and specific cardiovascular causes of mortality. 15 In the meantime, hemoglobin decline and reduced hematocrit value are the manifestations of anemia, which has high incidence in patients with AMI. 16 In the CADILLAC trial, which evaluated 2082 patients with AMI, approximately 13% of the patients had anemia. 17 A study of 78 974 elderly patients admitted with AMI has shown that baseline anemia is present in up to 40%. 18 A research has shown that baseline anemia and the occurrence of acute bleeding event will increase the mortality of patients with ACS and STEMI receiving PCI treatment. 19 Anemia is a predictor of increased 1-year cardiovascular mortality in patients with STEMI. If the patients have comorbidities such as chronic kidney disease or hypertension, the effect of anemia is very significant. 20 Therefore, we suggest that patients with STEMI with the high ORBIT scores may possess the following features, such as poorer renal function, greater age, and higher incidence of anemia. Thus, it can be seen that patients with STEMI with the higher ORBIT scores have poorer prognosis.
Conclusion
The ORBIT score was associated with 30-day mortality in patients with STEMI. The ORBIT score can be an independent predictor of short-term prognosis in patients with STEMI.
Footnotes
Authors’ Note
Jun-Hua Shen and Hui-Min Wang contributed equally to this work. All authors had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. The need for informed consent from the patients for publication of this information was waived by the institutional review board of the hospital for this study. This study was approved by the Ethics Committee of The Second Affiliated Hospital of Nantong University (IRB Number: 2019KS062).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study received grant support from the Science Foundation of Nantong City (grant numbers MSZ19105, MSZ19037, MSZ19242).