
Abstract
Acute myocardial infarction (AMI) is a leading cause of death and not a few of these patients are combined with acidemia. This study aimed to detect the association of acidemia with short-term mortality of AMI patients. A total of 972 AMI patients were selected from the Medical Information Mart for Intensive Care (MIMIC) III database for analysis. Propensity-score matching (PSM) was used to reduce the imbalance. Kaplan-Meier survival analysis was used to compare the mortality, and Cox-proportional hazards model was used to detect related factors associated with mortality. After PSM, a total of 345 non-acidemia patients and 345 matched acidemia patients were included. The non-acidemia patients had a significantly lower 30-day mortality (20.0% vs. 28.7%) and lower 90-day mortality (24.9% vs. 31.9%) than the acidemia patients (P < 0.001 for all). The severe-acidemia patients (PH < 7.25) had the highest 30-day mortality (52.6%) and 90-day mortality (53.9%) than non-acidemia patients and mild-acidemia (7.25 ≤ PH < 7.35) patients (P < 0.001). In Cox-proportional hazards model, acidemia was associated with improved 30-day mortality (HR = 1.518; 95%CI = 1.110-2.076, P = 0.009) and 90-day mortality (HR = 1.378; 95%CI = 1.034 -1.837, P = 0.029). These results suggest that severe acidemia is associated with improved 30-day mortality and 90-day mortality of AMI patients.
Introduction
Acute myocardial infarction (AMI) remains a leading cause of death in cardiovascular heart disease patients worldwide. Although there are many heart center, evolution of percutaneous coronary intervention (PCI) and intensive care by cardiac care unit (CCU) for AMI patients, the mortality of AMI still remains high. According to the previous researches, the 30-day mortality of AMI is 4.9-7.1%, and 90-day mortality is 12.2%. 1 –4 A previous study showed that there were 128,088 of 1.8 million AMI patients died during admission. 5 In a multicentre research, the cost of AMI is $19,842 during the first year and $845 per year for the next 5 years. 6 In addition, not a few of the survival would go into the different stages of heart failure, which to affects the quality of patients’ life and costs a lot. Thus, intervention in AMI remains a heat focus worldwide.
In recent years, more and more risk factors of the mortality of AMI, such as gender, hyponatremia, MR-proANP, HbA1c, serum low-density lipoprotein cholesterol (LDL-c) level have been identified. 7 –11 Acidemia is a common pathophysiological condition, which has been demonstrated to increase the mortality of several diseases like cirrhosis, sepsis, chronic kidney disease (CKD) and so on. 12 –14 Cardiologists mainly focus on the evaluation of electrocardiogram and the stenosis of coronary artery, but blood gas could also provide extra help on the comprehensive assessment of the patients. Several researches showed us that 4.2%-22.0% AMI patients complicated with acidemia. 15,16 Data from early study demonstrated that metabolic acidosis and lactic acidosis are important factors in causing the high mortality from acute myocardial infarction. 17 However, little data is available on the association of acidemia with short-term mortality of AMI patients. Here, we retrospectively selected 972 AMI patients admitted in intensive care unit (ICU) based on the Medical Information Mart for Intensive Care (MIMIC) III, aiming to detect the association of acidemia with the 30-day mortality and 90-day mortality of AMI patients.
Methods
Data Source
The primary data of this study was acquired from a large and single-center database, MIMIC-III, containing data associated with over 50,000 distinct hospital patients admitted to critical care units between 2001 and 2012. All the information of the patients such as the demographic characteristics, diagnosis, admission time, dead time, laboratory tests, and treatment outcomes was integrated in 38 tables. 18 As this was a retrospective cohort study, informed consent was unnecessary. One of the authors (G.Y.-Z., certification number: 9016236) gained access to documented the database after online training at the National Institutes of Health (NIH). Institutional Review Boards (IRB) of the Massachusetts Institute of Technology (MIT, Cam-bridge, MA, America) and Beth Israel Deaconess Medical Center approved the database construction. Data was extracted by structured query language with pgAdmin4 PostgreSQL 9.6 (https://www.postgresql.org/).
Patients Selected and Stratification Method
Patients firstly admitted in critical care unit and diagnosed as AMI according to the ICD-9 were collected continuously. Those who were younger than 18 years old were excluded from this analysis. Patients’ baseline characteristics were collected and Sequential Organ Failure Assessment (SOFA) scores were calculated according to the description in previous study. 19 The first measurement of blood gas, blood glucose, hemoglobin, and serum creatinine (Scr) of the patients admitted in ICU were selected. Patients used vasoactive drugs (containing dopamine, epinephrine and norepinephrine), mechanical ventilation, and intro-aortic balloon pump (IABP) within 24 h after ICU admissions were also recorded. Estimated glomerular filtration rate (eGFR) was calculated as: 175×(Scr^-1.154)×(age^-0.203)×1.212(if black)×0.741(if female). 20 Patients with blood gas PH < 7.35 were separated in acidemia group and patients with 7.35≤PH≤7.45 were separated in non-acidemia group. 21 Patients with blood gas PH > 7.45 were excluded from this study. The anion gap (AG) was calculated as: AG = [(Na+)+(K+)]-[(HCO3-)+(Cl-)]. 22 Elevated AG was defined as AG > 16 mmol/L. Anemia was defined as hemoglobin (Hb) < 120.0×103 g/ml for male and Hb < 110.0×103 g/ml for female. Missing value was replaced with means (normal distribution) or modes (skewed distribution), or dropped if its ratio > 30%. The primary endpoint was 30-day mortality and the secondary endpoint was 90-day mortality.
Statistical Analysis
Continuous variables were presented as medians with interquartile range (IQR) or Mean ± SD (if it was normal distribution), and categorical variables were presented by number and percentage. Continuous data were compared by the Mann-Whitney test or t-test as appropriate, and the categorical data were compared by Chi-square test. Propensity score matching (PSM) was used to reduce the imbalance between each group with a 1:1 nearest neighbor matching and a caliper width of 0.05. All the imbalanced categaorial variables were included in PSM. Kaplan-Meier survival analysis was performed to determine whether combined with acidemia affected 30-day mortality and 90-day mortality of AMI patients and compared by Log-rank test, then Kaplan-Meier curves were depicted. Cox-proportional hazards model was used to screen the related factors that associated with the mortality of AMI patients and Hazard ratio (HR) with 95% confidence interval (CI) was used to express the effect. All the above analyses were performed using the software Stata V.14.0 and the significant difference was set as 2-side P < 0.05.
Results
Patient Characteristics
A total of 972 patients were included in this study. The non-acidemia group contains 604 patients (406 males vs. 198 females, age 68.20 ± 13.23 years old), and the acidemia group contains 368 patients (224 males vs. 144 females, age 67.45 ± 13.58 years old). After propensity-score matching, a total of 345 acidemia patients were matched with 345 non-acidemia patients. All the baseline variables were compared between the 2 groups in Table 1. Patients were mainly admitted in cardiac care unit (CCU). Before PSM, the SOFA score, and the rate of cardiogenic shock, use of vasoactive drugs, use of mechanical ventilation were higher in acidemia group than in non-acidemia group (P < 0.001 for all). The PCO2, chloride, and potassium of blood gas were higher in acidemia patients than in non-acidemia patients, and the biocarbonate was higher in non-acidemia group patients than in acidemia group patients (P < 0.001 for all). After PSM, the differences of blood glucose level, the rate of gender, ICU admission, cardiogenic shock, diabetes mellitus, use of vasoactive drugs, use of mechanical ventilation, and SOFA score between acidemia patients and non-acidemia patients were balanced.
Basic Characteristic of the Patients Before and After Propensity-Score Matching (PSM).

ICU, intensive care unit; CCU, cardiac care unit; CSRU, Cardiovascular surgery rehabilitation unit; MICU, Medical intensive care unit; SICU, Surgical intensive care unit; TSICU, Translant surgery care unit; COPD, chronic obstructive pulmonary disease; AG, anion gap; SOFA, Sequential Organ Failure Assessment; IABP, intro-aortic balloon pump.
Outcome
As described in Table 2, the 30-day mortality and 90-day mortality of AMI patients with acidemia, mild-acidemia, and severe-acidemia were all higher than the mortality of non-acidemia AMI patients before PSM (P < 0.05-P < 0.001). But after PSM, there was no significant difference in neither 30-day mortality nor 90-day mortality between mild-acidemia patients and non-acidemia patients (Table 3, P > 0.05 for all). The non-acidemia patients had lower 30-day mortality (20.0% vs. 28.7%) and lower 90-day mortality (24.9% vs. 31.9%) than the acidemia patients (P < 0.001 for all). In subgroup analysis, the severe-acidemia patients with PH < 7.25 had the highest 30-day mortality (52.6%) and 90-day mortality (53.9%) than non-acidemia patients (P < 0.001).
Comparison of Mortality Between Non-Acidemia Patients and Acidemia Patients Before PSM.
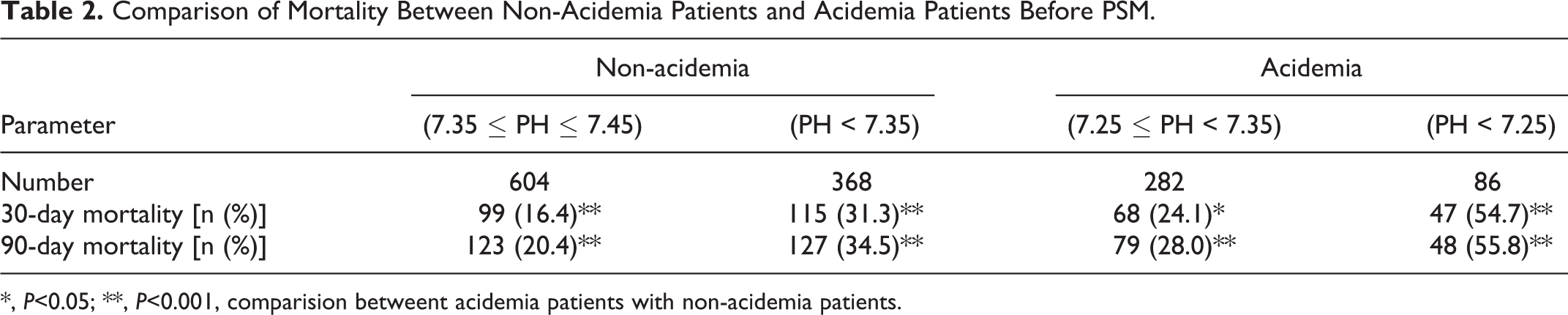
*, P<0.05; **, P<0.001, comparision betweent acidemia patients with non-acidemia patients.
Comparison of Mortality Between non-Acidemia Patients and Acidemia Patients after PSM.
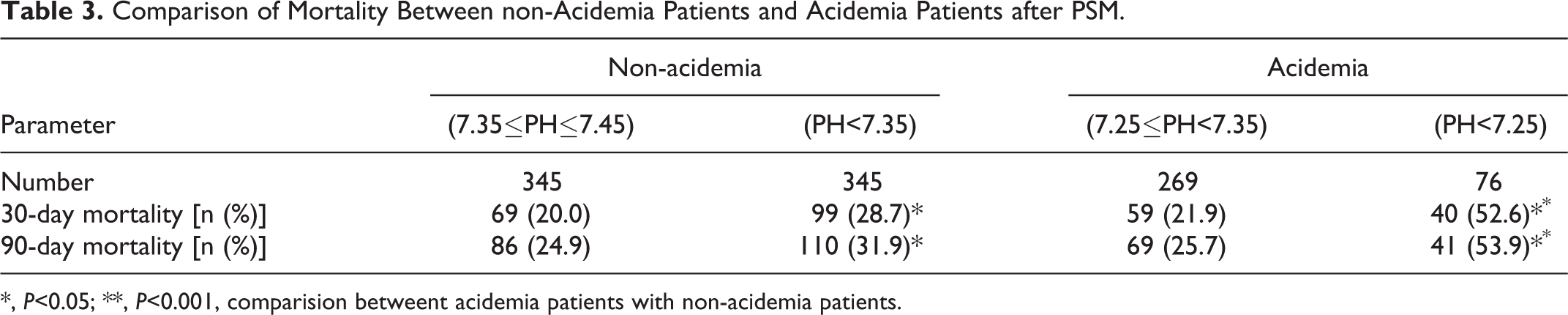
*, P<0.05; **, P<0.001, comparision betweent acidemia patients with non-acidemia patients.
Association of Acidemia With Mortality
Aiming to detect whether acidemia was associated with the prognosis of AMI patients, Kaplan-Meier survival analysis was performed. As shown in Figure 1A and B, acidemia was associated with the increasing of both the 30-day mortality and 90-day mortality of AMI patients. In addition, severe acidemia (PH < 7.25) was notably associated with the improved mortality than non-acidemia patients (Figure 1E and F [P < 0.001]), but the 30-day mortality and 90-day mortality showed no significant difference between mild-acidemia patients and non-acidemia patients (Figure 1C and D [P > 0.05]).

Kaplan-Meier curves of different groups. a, c, e. Kaplan-Meier curves of 30-day after ICU admission of non-acidemia AMI patients vs. acidemia AMI patients, non-acidemia AMI patients vs. mildacidemia AMI patients, and non-acidemia AMI patients vs. severe-acidemia AMI patients. b, d, f. Kaplan- Meier curves of 90-day after ICU admission of non-acidemia AMI patients vs. acidemia AMI patients, nonacidemia AMI patients vs. mild-acidemia AMI patients, and non-acidemia AMI patients vs. severe-acidemia AMI patients. Non-acidemia, 7.35≤PH≤7.45; Mild-acidemia, 7.25 ≤ PH < 7.35; Severe-acidemia, PH < 7.25.
Risk Factors of Mortality
It is described in Figure 2A that several risk factors of 30-day mortality of all AMI patients have been identified, using cox proportional hazards model adjusted for gender, age, combinations (Hypertension, Hyperlipidemia, Arrhythmia, Cardiogenic shock, Heart failure, Diabetes mellitus, Pneumonia, COPD, Liver disease, Chronic kidney diseases and Malignancy), SpO2, anemia, AG, usage of vasoactive drugs, mechanical ventilation, and IABP. Among them, risk factors of 30-day mortality of AMI patients were as following: cardiac shock (HR = 1.991, 95%CI = 1.416-2.799), usage of mechanical ventilation (HR = 2.056, 95%CI = 1.427-2.962), acidemia (HR = 1.518, 95%CI = 1.110-2.076), age > 60 years (HR = 1.931, 95%CI = 1.267-2.946), SpO2 < 95% (HR = 1.629, 95%CI = 1.182-2.244), diabetes mellitus (HR = 1.661, 95%CI = 1.179-2.341), COPD (HR = 2.777, 95%CI = 1.242-6.205), and elevated AG (HR = 1.391, 95%CI = 1.005 -1.927). The results were similar in 90-day mortality cox proportional hazards model analysis (Figure 2B). When the moderate acidemia patients were excluded, cardiac shock, acidemia, age >60 years, SpO2 < 95%, and COPD were also still the risk factors of both 30-day mortality and 90-day mortality (Figure 2C and D).

Hazard ratio of related factors associated with short-term mortality of AMI patients in ICU admission. a. HR of related factors associated with 30-day mortality of all the AMI patients. b. HR of related factors associated with 90-day mortality of all the AMI patients. c. HR of related factors associated with 30- day mortality of non-acidemia AMI patients and severe-acidemia (PH < 7.25) AMI patients. d. HR of related factors associated with 90-day mortality of non-acidemia AMI patients and severe-acidemia (PH < 7.25) AMI patients. HR, Hazard ratio; CI, Confidence interval; COPD, Chronic obstructive pulmonary disease; AG: Anion gap.
Discussion
Acute myocardial infarction is one of the severe acute cardiovascular diseases with highly fatal mortality. To date, mortality of AMI decreases continually with the help of timely PCI and comprehensive intervention containing the use of ACEI, β-blocker and statin. 23,24 In addition, professional care provided by ICU/CCU helps the AMI patients go through difficult times, as part of the AMI patients combined with cardiac shock, malignant arrhythmia, or severe acid-base imbalance. As the clinical manifestations are kaleidoscopic, not a few of AMI patients may not manifest notable respiratory symptoms, which sometimes leads to the neglection of blood gas analysis. In the current study, we analyzed the association of acidemia with short-term mortality of AMI patients, aiming to provide some foundation for the intervention on acidemia of AMI patients.
Acidemia is mainly diagnosed according to the blood gas with PH < 7.35 and it can be classified as metabolic acidosis, respiratory acidosis, lactic acidosis, increased AG acidosis, and non-increased AG acidosis. 25 It is mainly due to the increase of the acidic substance and/or decrease of the alkaline substance. AMI leads to different ischemia, injury, and necrosis of cardiac myocytes, which may results in oxygen deficit, concentration alteration of several intro-cellular ions and extra-cellular ions, and apoptosis of cardiac myocytes. The above variation could aggravate acidemia, and acidemia could in turn aggravate ischemia, oxygen deficit injury, and apoptosis of cardiac myocytes.
Till now, there is a big account of researches focus on the effects of hypoxia and acidemia on cardiac myocyte injury and/or death. Data from Lori A. Kubasiak et al. demonstrated that cardiac myocyte death can be activated by hypoxia combined with acidemia through the Bcl-2 family protein BNIP3. BNIP3 can promote calcium and calpain-dependent cell death. 26,27 John W. Thompson and his team reported that acidemia and hypoxia could activate the DNase, and of apoptosis-inducing factor and DNace II were co-localized with the mitochondria and lysosomes, respectively, and they would translate to nucleus when PH decrease to lower than 6.1-6.7. 28 In addition, a recent study suggested that acidemia can promote cell apoptosis through the G protein-coupled receptor 4/CCAAT/enhancer-binding protein homologous protein pathway. 29 A previous research demonstrated that the expression of miR-133b, which is involved in the regulation of proliferation, cell death and migration can be regulated by acidemia. 30 In the present study, the 30-day mortality and 90-day mortality of AMI patients with acidemia were higher than the AMI patients without acidemia. It is notable to find that when PH < 7.25, the mortality went up to a higher level than the PH varied from 7.25 to 7.35. These results might be associated with above mechanisms. Interestingly, mild-acidemia showed no significant effect on the 30-day and 90-day mortality. Data from previous study suggests that acidemia could promot the myocardial apoptosis. 31 As we known, cardiomyocytes is on of the non-regenerative cells. In our opinion, mild-acidemia can be corrected easier than severe-acidemia, and severe-acidemia may lead to deeper or a larger scale of cardiomyocyte apoptosis, which finally affects the heart function. Thus, severe acidemia in acute perior might result in the permanent myocardiomyocyte damage and then increase the 30-day and 90-day mortality of AMI patients.
Calcium ions play an essential role not only in myocardial contraction but also in the occurrence of arrhythmia. 32,33 Acidemia increases extracellular H+ level and then promotes the exchange between the extracellular H+ and intracellular Ca2+, decreasing the intracellular Ca2+ levels and reduces the contractility of the heart muscle, finally leads to hypoinfusion of vital organs. Besides, H+-Ca2+ exchange promotes Ca2+ translates into cell, shortening the second stages and the whole action potential, finally increases the risk of arrhythmia. Acidemia can also affect the activity of Na+-K+-ATP pump then also affect the action potential. Several earlier studies suggested that the risk of ventricular arrhythmias would increase due to acidemia-induced cellular electrophysiological alteration. 34 –37 In animal research, cellular Ca2+ transient alternans and repolarization alternans susceptibility increase notably when the heart is in acidemia and ischemic, and acidemia can influence Ca2+ waves via inhibitory Hi + and stimulatory Nai + signals. 38,39 Thus, the effect of acidemia on the changes of ions is complicated, but it is of great significance to correct acidemia after AMI in time as it may help increase myocardial contraction and reduce the occurrence of arrhythmia.
We also found several other factors related to the mortality of AMI patients. In this study, AMI patients with cardiac shock carry 1.991 times risk of 30-day mortality than the ones without cardiac shock. A large-size retrospective study showed that proportion of ICU admissions with cardiac shock in 2012 was twice as it was in 1997. Although the mortality had decreased from 50% to 45%, the age of patients had decreased by 2.7 years. 40 Results from another study suggested that patients with cardiac arrest and/or cardiac shock represent 10% of ST segment elevation myocardial infarction (STEMI) patients and account for 80% of deaths, and the mortality was significant higher than the patients without cardiac shock. 2 Cardiac shock leads to low perfusion of several important organs, resulting in hypoxia of organ, accumulation of lactic acid and nitric oxide, and even dysfunction of organs like acute kidney injury. Other factors like mechanical ventilation and COPD are also identified as mortality risks of AMI patients in our study. Thomas Metkus et al. suggested that mechanical respiratory support in NSTEMI is independently associated with mortality, and the mortality of invasive mechanical ventilation is significantly (HR = 0.86; 95%CI = 1.74 -1.98) higher than non-invasive ventilation (HR = 3.03; 95%CI = 2.88-3.19). 41 Previous large-scale study found that AMI patients combined with COPD had worse outcome than those without COPD, and it is similar to find that 90-day mortality and overall mortality of AMI with COPD are higher than those without COPD in another study from Taiwan. 42,43 Besides, age >60 years and SpO2 were also the risk factor of shorr-term mortality of AMI patients. These remind us that the interference on the prognosis of AMI patients is comprehensive and should include multi-variables.
There are several limitations in this study. Firstly, we just selected the AMI patients according to the ICD-9 diagnosis, but there are a part of patients diagnosed as acute coronary syndrome containing STEMI and NSTEMI may be dismissed. Secondly, though we have included several related factors in this study, other potential factors like cTnI, BNP, serum lipids, and drugs which may affect the mortality have not been included as their high rate of missing data or variety of drugs. Finally, we just detect the 30-day mortality and 90-day mortality, but long-term follow-up has not been performed in the current study.
Conclusion
In this study, we used Mimic-III database to detect the association of acidemia with short-term mortality of AMI patients admitted in ICU. It is noteble to find that severe acidemia may increase the 30-day mortality and 90-day mortality of AMI patients after admission in ICU. Cardiac shock, mechanical ventilation, age >60 years, SpO2 < 95%, diabetes mellitus, and COPD may be potential risk factors of short-term mortality of AMI patients.
Footnotes
Abbreviations
Author Contributions
T. Z. and Y.-Z. G. conceived the study, participated in the design, performed the statistical analysis, and drafted the manuscript. H. L. conceived the study, participated in the design and helped to draft the manuscript. All authors read and approved the final manuscript.
Availability of Data and Materials
Ethics approval
Laboratory for Computational Physiology at the Massachusetts Institute of Technology.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Patient consent
Informed consent for patient information to be published in this article was not obtained because this was a retrospective cohort study.