
Abstract
Aim:
The aim of this study was to analyze how the consumption of medication over time affects the survival rate in patients with a coronary event and whether there is a gender difference.
Methods:
The study included 804 patients admitted to 4 hospitals with a coronary event during 2007. Monitoring after coronary event was carried out during 2007 and every 6 months in the subsequent 2 years (2008 and 2009) throughout the review of the clinical history of the patient. The main outcome was the analysis of mortality after the coronary event. Kaplan-Meier survival curves were plotted to calculate the time to death, comparing women versus men for 4 medication groups: aspirin, statins, β-blockers, and angiotensin-converting enzyme inhibitors/angiotensin receptor blockers (ACEIs/ARBs). A Cox regression model was used for the final mortality analysis.
Results:
During the follow-up time, 172 deaths were assessed. Each month of treatment with aspirin, statins, β-blockers, or ACEI/ARB was associated with a decrease in mortality between 13.0% and 0.5% (univariate analysis). The Kaplan-Meier method revealed a significant reduction in mortality after the coronary event for each month of treatment with aspirin (men), statins (men), and β-blockers (both men and women). No significant effect in survival was observed in either gender with ACEI/ARB treatment. The final multivariable model (Cox regression) showed that the taking of aspirin, statins, β-blockers, or ACEI/ARB is able to reduce mortality rates up to 7.0% (aspirin) throughout each month of treatment after a coronary event without any influence of gender.
Conclusion:
Aspirin, statins, β-blockers, and ACEI/ARB revealed a protective character with each month of treatment throughout the follow-up period, in terms of risk reduction of death. Aspirin and statins showed the maximum benefit, followed by ACEI/ARB and β-blockers.
Introduction
Coronary illness is one of the principal causes of death in both men and women in Western countries. 1 The introduction of new diagnostic procedures, reperfusion intervention, and preventative measures, such as the initiation of new methods of treatment, has contributed in recent years to a decrease in mortality in myocardial infarction. 2 –5 The differences in mortality figures between men and women have been described not only in the way symptoms appear but also by treatment that is received and in the observed prognosis. 1,6,7 Studies undertaken have demonstrated that certain risk factors are associated with an increased risk of death after a heart attack, such as specific associated pathologies (hypertension, diabetes, and previous coronary history), the affected cardiac area, the time and type of clinical/hospital intervention or the treatment used, among others. 8,9
The implementation of new intrahospital procedures and the application of specific treatments, recommended by various scientific societies and evidence-based documentation, 10,11 can vary according to countries and clinical care practice. 12 –16 In its turn, inadequate control of cardiovascular risk factors means not only an excessive risk of morbidity and mortality for the patient but also a high consumption of resources which require that health efforts be directed toward primary prevention of coronary illness. 17
Studies have addressed analysis based on various cardiovascular risk factors, patient comorbidities, or reperfusion interventions across the hospital group. Most of them have evaluated the relationship between the use of drugs and certain subrogate variables such as achievement of therapeutic goals (low-density lipoprotein [LDL], blood pressure, etc). The objective of this study is to analyze how the monthly consumption of medication over time affects the survival rate in patients who have experienced a coronary event and whether there is a gender difference.
Methods and Materials
Study Cohort
We carried out a retrospective analysis which included patients admitted with a coronary event during 2007 to the following hospitals: S. Juan de Dios de Bormujos (Seville), La Inmaculada de Huercal-Overa (Almería), La Serranía de Ronda (Malaga), and the Hospital de Jerez (Cádiz), which encompass populations of 236 532, 150 000, 124 000, and 420 000 inhabitants, respectively. The study included patients selected from the records of hospital discharges or emergency consultations with the following ICD-9 codes (ninth version of the World Health Organization’s International Classification of Diseases): acute heart attack (410), unstable angina (411, 413.0, 413.1), or chronic ischemic heart disease (412-414, excluding 413 and 413.1).
As in real life, more men suffer a cardiac event than women; in order to assess a sampling where men and women were equally represented, the sample size was estimated by including all the women with diagnosed acute heart attack, unstable angina, or chronic ischemic heart disease identified by the presence of the mentioned ICD-9 codes in 2007. A total of 461 women were included according to these criteria. The same proportion of men was also selected across a sampling of random lists from the records of hospital discharges or emergency consultations from the four hospitals included in the study (Figure 1). All clinical data from the patient, the diagnostic procedures, and the prescribed medication upon discharge were extracted from these reports. The identification data of the patient permitted an informed revision of their digital history in primary care with the objective of analyzing the cardiovascular risk factors that the patient exhibited prior to their admission (hypertension, diabetes, and smoking) as well as the medication they were taking to control such risk factors (antihypertensive, statins, aspirin) throughout the follow-up period. Monitoring after coronary event was carried out during 2007 and every 6 months in the subsequent 2 years (2008 and 2009) throughout the review of the clinical history of the patient. It was assumed therapeutic compliance to treatments when prescriptions were active in digitized health records. Patients younger than 18, a hospital admission of less than 2 days (in order to rule out cases of admission for only diagnostic tests), and the absence of clinical data and/or unrecoverable patient treatment were all excluded.
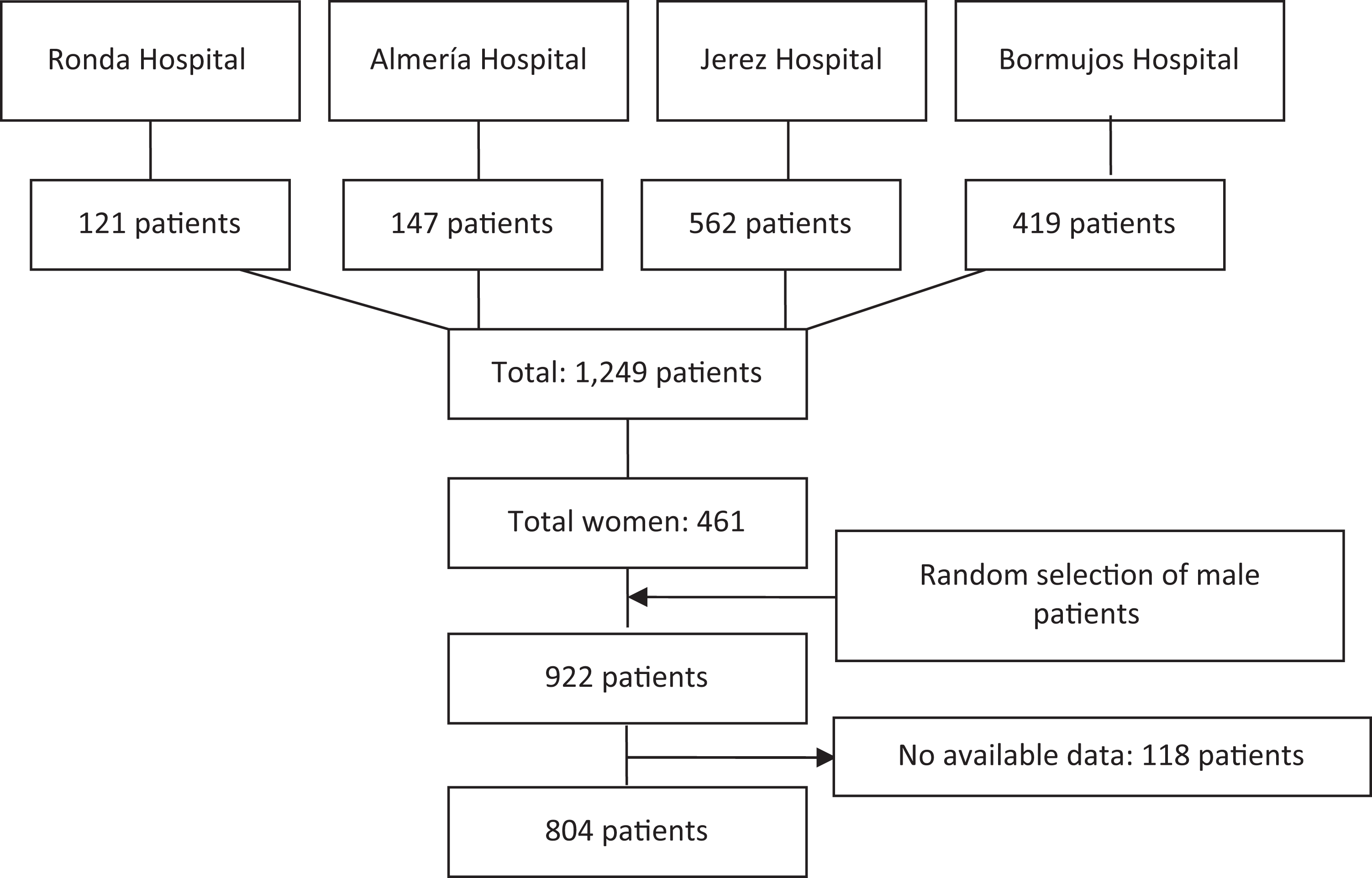
Study population.
Objective
The primary clinical outcome in the study was the analysis of mortality after a coronary event. The factors selected for analysis included age, gender, cardiovascular risk factors (smoking, hypertension, diabetes, and dyslipidemia), previous cardiovascular illness, coronary interventions (primary percutaneous coronary intervention or surgery), treatment upon hospital discharge, and medication during the subsequent 2 years after the coronary event such as β-blockers, angiotensin-converting enzyme inhibitors/angiotensin receptor blockers (ACEIs/ARBs), aspirin, and statins. Hypertension, diabetes, and hypercholesterolemia were monitored during the follow-up based on drug consumption or diagnostics extracted from primary care records.
Statistical Analysis
Continuous variables were summarized with typical and average deviations and, in the case of very asymmetrical distributions, with medians and inter quartile procedures (P25 and P75). Tables of frequency and percentages were employed for categorical variables. Accurate estimates and 95% confidence intervals (95% CIs) for the different statistics were obtained. Cross tabulations were performed, and χ2 test, χ2 test with continuity correction, or Fisher test (for 2 × 2 small population tables) was applied in order to validate the relationship between 2 qualitative variables. Kaplan-Meier survival curves were plotted to calculate the time to death comparing women versus men for the 4 medication groups (β-blockers, ACEI/ARB, aspirin, and statins). The log-rank test was employed in order to compare the uniformity of the distributions of survival rates among the different groups.
A Cox regression model has been used in order to study the possible variable confounders in the analysis of mortality after a coronary event. A prior univariate analysis was performed that identified those connected variables to the time factor leading to death. A multivariable analysis to construct the final model was created with such selected variables. It allowed the examination of the relationship between the time of death and each variable while monitoring the rest of the variables included in the model. A standard significance of 0.15 in the univariate analysis prior to the multivariable analysis was taken into account. The hazard ratios and 95% CI were calculated for the selected variables. All analyses were conducted using SPSS version 22.0.
Results
A total of 1249 patients with a coronary event were admitted to the 4 hospitals included in this study during 2007. The final sample analyzed was 804 patients (Figure 1). The basic characteristics of the patients are shown in Table 1. The main risk factor was hypertension (53.6%), followed by mellitus diabetes (43.7%). The medication mostly given upon hospital discharge was aspirin (78.5%).
Baseline Characteristics for Survival Analysis in Patients After a Coronary Event.
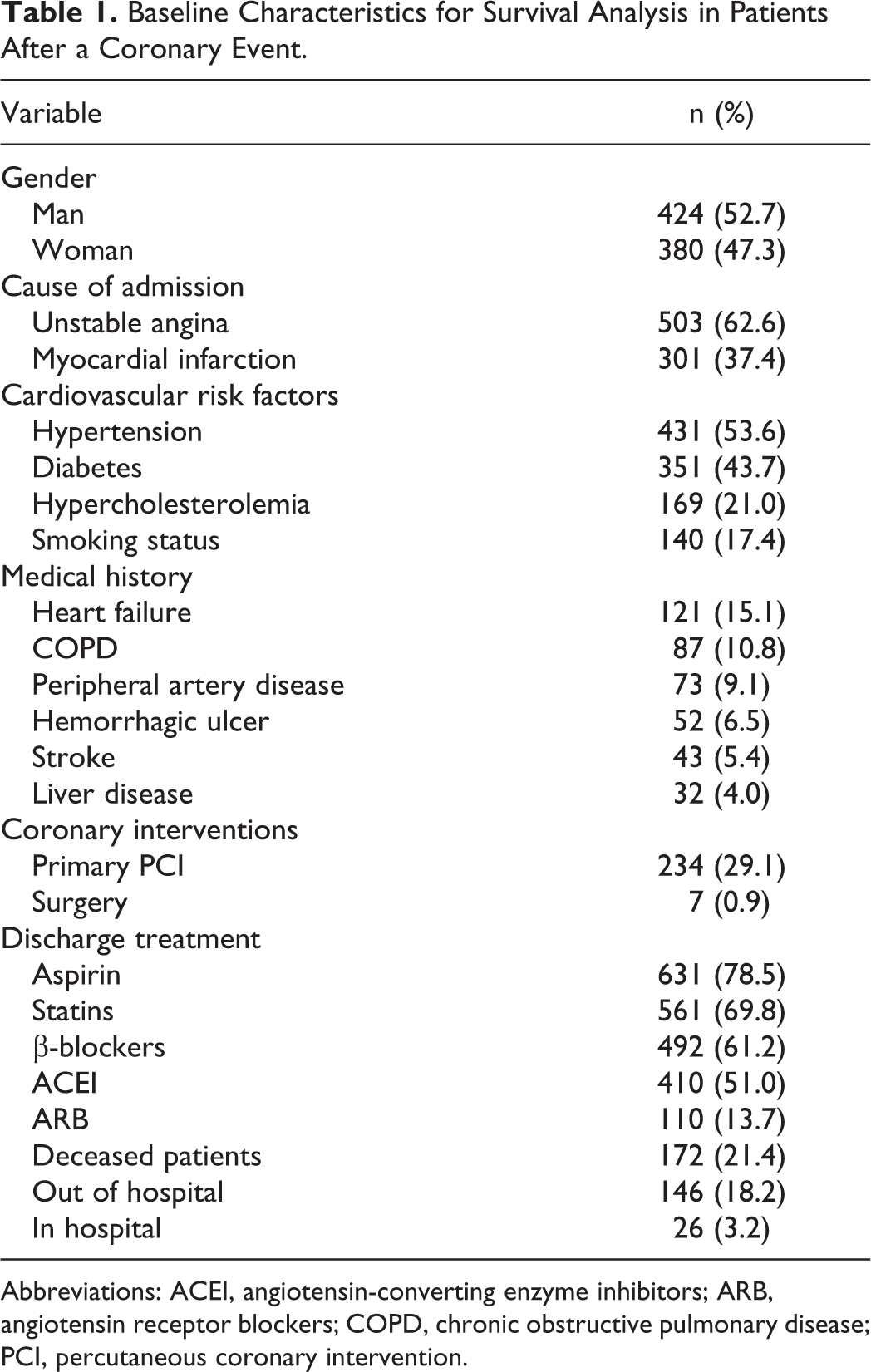
Abbreviations: ACEI, angiotensin-converting enzyme inhibitors; ARB, angiotensin receptor blockers; COPD, chronic obstructive pulmonary disease; PCI, percutaneous coronary intervention.
During the follow-up time, 172 deaths were assessed. Significant differences were observed in the age distribution between the dead patients and those surviving (P < .001): 76.4 (95% CI: 74.9-78.0) years versus 67.5 (95% CI: 66.6-68.4) years, respectively. A total of 50% of the surviving patients showed a superior follow-up time to that of those who died (P < .001): 894 (789.0) days versus 228 (110.4) days, respectively.
The patients who died during the follow-up period showed a greater incidence of diabetes, hypertension, hemorrhagic ulcer history, heart failure, peripheral artery disease, and stroke. Coronary intervention was predominant in surviving patients in relation to those dying (35.8% vs 8.7%; Table 2).
Baseline Characteristics of Survival and Deceased Patients After a Coronary Event.

Abbreviation: COPD, chronic obstructive pulmonary disease.
Univariate analysis based on Cox regression showed that patients with hypertension had a 2.02 times (95% CI: 1.43-2.86; P < .0001) greater risk of dying at any moment of the follow-up period than those who were nonhypertensive. The stroke and previous hemorrhagic ulcer were the clinical situations that showed a great risk of death: 2.44 (95% CI: 1.43-4.17; P < .001) and 2.32 (95% CI: 1.43-3.75; P < .001), respectively. Each month of treatment with aspirin, statins, β-blockers, or ACEI/ARB was associated with a decrease in mortality between 13.0% (aspirin) and 0.5% (β-blockers; Table 3).
Univariate Analysis Based on Cox Regression for Variables Related to Mortality Risk After a Coronary Event.

Abbreviations: ACEI/ARB, angiotensin-converting enzyme inhibitors/angiotensin receptor blockers; COPD, chronic obstructive pulmonary disease.
The Kaplan-Meier method, categorized by gender and without considering other possible variable confounders, revealed a significant reduction in mortality after a coronary event for each month of treatment with aspirin (men), statins (men), and β-blockers (both men and women). No significant effect on survival was observed in either gender with ACEI/ARB treatment (Figure 2).

A, Kaplan-Meier survival curves in men with a coronary event and in treatment with aspirin (P < .001), statins (P < .001), β-blockers (P < .001), or angiotensin-converting enzyme inhibitors/angiotensin receptor blockers (ACEIs/ARBs; P = .217). B, Kaplan-Meier survival curves in women with a coronary event and in treatment with aspirin (P = .499), statins (P = .161), β-blockers (P = .037), or ACEI/ARB (P = .054).
The final multivariable model showed that the taking of aspirin, statins, β-blockers, or ACEI/ARB is able to reduce mortality rates up to 7% (with monthly aspirin consumption) through each month of treatment after a coronary event without influence of gender and monitoring the rest of the variables included in the model (Table 4).
Multivariate Analysis Based on Cox Regression for Variables Related to Mortality Risk After a Coronary Event.
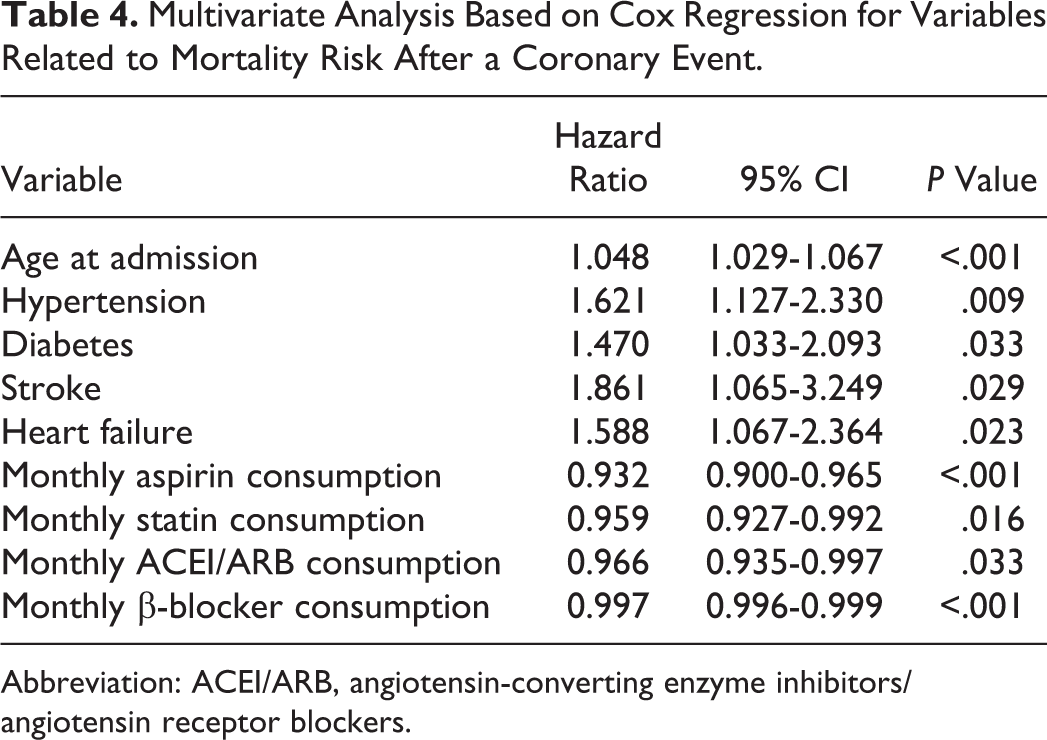
Abbreviation: ACEI/ARB, angiotensin-converting enzyme inhibitors/angiotensin receptor blockers.
Discussion
The prescribing of treatment upon discharge is not always continuous for the patient when it deals with chronic conditions. One of the principal aspects of this study has been to assess the use of monthly medication by patients throughout the follow-up period and its effect on survival after a coronary event. The results of our study reveal a protective character with each month of treatment by aspirin, statins, β-blockers, or ACEI/ARB, throughout the follow-up period in terms of risk reduction of death, monitoring other cardiovascular risk factors. These treatments are in line with recommendations from the clinical practice guidelines and the major scientific societies, 10,11,18 –20 yet the impact of monthly death rates had not been previously analyzed.
There are 2 strengths to be highlighted in this study. First, this is a unique study to compare gender differences in survival rate with medications used after a coronary event. The other important point is to note that hypercholesterolemia is not as much of a risk factor as hypertension and diabetes in case of coronary events. It might indicate that we should revisit the association of cholesterol levels and cardiovascular functions.
Analysis of survival by means of Kaplan-Meier graphs (Figure 2) showed a tendency toward mortality reduction through the monthly use of aspirin, statins, β-blockers but not so with ACEI/ARB, although without a statistical significance. The gender analysis by Kaplan-Meier did not show relevant significant reduction in mortality after a coronary event in women for each month of treatment with aspirin or statins. These results were not confirmed by multivariate Cox regression model, adjusting by other variable confounders.
The recent meta-analyses performed with ACEI/ARB have shown that in the hypertensive or diabetic patient, ACEIs, as opposed to ARBs, reduced mortality. 21,22 The lack of a “protective” effect of ACEIs/ARBs has been reflected in different studies, 2,8,9,23 suggesting that other confounding factors may exist in the reason for which they were prescribed. A subsequent analysis should be done to evaluate whether those patients taking an ACEI/ARB would have a more critical prognosis. The European Society of Cardiology stated that, given the relatively modest effect provided by ACE inhibitors, its long-term use cannot be considered mandatory in patients with ST-segment elevation myocardial infarction (STEMI), with no high blood pressure, without heart failure, or in those who did not have left ventricle dysfunction or diabetes. 10 The analyzed sample of patients did not show differences in the incidence of standardized heart failure by gender, though there was a greater proportion of male hypertensive patients. A recent observational study has shown that ARBs confer greater protection than ACEIs in patients with high-risk cardiovascular disease. 24 We have not analyzed ACEIs and ARBs separately, as the aim was to study the effect of mortality on defined drug groups (statins, β-blockers, or those targeting the renin–angiotensin system). Nevertheless, those results might not be comparable with this work, as patients included in our study were only those suffering a coronary event.
Background histories of hypercholesterolemia, based on the taking of statins, revealed no significant association with survival. Living patients showed a greater hypercholesterolemic profile compared to those who died (22% vs 17%; Table 2). These data did not show statistical significance but concur with observations by other researchers. 23 Results obtained from the clinical trials with lipid-lowering drugs in the primary prevention of cardiovascular illness demonstrated a limited clinical relevance without any reduction in mortality. 25 These facts suggest that hypercholesterolemia presents a lesser contribution to the risk of death compared to that observed in smokers, patients with hypertension, or those with diabetes. Such tendency is in line with recent evidence in the cardiovascular field, which points to a nonattainment of objective levels of LDL-cholesterol when a lipid-lowering treatment is indicated in a high-risk cardiovascular patient. 26,27 The final model of mortality risk presumes a new focus of analysis to evaluate the benefit of each month of treatment in the reduction of death rates after a coronary event. Data show how the positive effects of monthly medication are able to be influenced by different cardiovascular risk factors. Hypertension or diabetes possesses an important impact on mortality after a coronary event with increments of 62% and 47%, respectively. Heart failure or stroke also negatively contributes in the model, increasing mortality by 59% and 86%, respectively. Our results concur with previous studies in which age, hypertension, mellitus diabetes, and histories of stroke or heart failure were identified as determinants of death in patients with coronary events. 2 –4,6
Each month of treatment with acetylsalicylic acid was associated with a reduction of 7% in monthly mortality after a coronary event, once the other variables in the model were controlled. This drug is assumed to provide a major contribution to survival among other analyzed drugs. Nevertheless, surprisingly only 78.5% of patients were nominated for such treatment upon hospital discharge. The use of dual antiplatelet therapy (aspirin and clopidogrel, prasugrel, or ticagrelor) was not evaluated as this treatment is recommended for between 6 and 12 months and the aim of the study was to investigate the effect of drugs on mortality for 2-year follow-up period.
The gender variable does not appear in the final analysis, as no difference was observed in the protective monthly model of treatment between men and women, after controlling the remaining cardiovascular risk factors assessed (hypertension, diabetes, stroke, or heart failure). These results contrast with those derived from other researchers who observed significant differences in the mortality risk between men and women. 3,6,8 Results from the present study analyze mortality associated with each month of medication, taking into consideration possible confounders that have not been addressed by other researchers. It may explain the different results obtained, as well as the possible variations in follow-up treatment, the different hospital procedures for women, and the different proportion of men included in the other studies. The rates of death observed in other publications are not comparable with the results of this work, having been made in different years, different periods of follow-up time (months or years), or patients classified by types of heart attack or across their sociodemographic characteristics. 2,3,6,8,9,12,23,28,29 The results showed that 36% of survival patients received revascularization (coronary aortic bypass or percutaneous coronary intervention) compared with 9% of those dying. A decrease in mortality was 81% in those patients who had undergone some form of revascularization process (Table 3). Nevertheless, the final version of multivariable analysis did not include coronary intervention in the patient risk of death after a coronary event, different to other published works. 6,3 Some studies have observed that these procedures are able to improve survival; yet in others, a reduction in mortality has not been verified, in the short or the long term. Some researchers conclude that the protective effect could lie in the medical care administered at the moment of hospital admission. The large sample taken from hospital admissions of coronary events in different provinces of Andalucía confers a high representation in clinical skill and the prognostic factor for these patients.
There are limitations in our study. This is an observational study and it is not possible to rule out the existence of an inclusive bias. The cause–effect association has to be given importance with caution. The contraindications of the drugs given to the sample patients of the study have not been collected as it could have influenced the use of certain medications and could be a possible confounding element. Nevertheless, a high prevalence of contraindications in antiplatelets, lipid-lowering drugs, or β-blockers is not expected. One of the limitations of the study is the source of the collection of monitoring data from digitized health records. Smoking showed a lower data in publications from other studies, which suggests a lower record in this risk factor. The diagnoses of diabetes, hypercholesterolemia, and hypertension may be extended equal consideration. Personal interviews with the physician assisted in such cases to gather those data that were not collected in the patient’s records.
More sophisticated measures such as ejection fraction, indices of infarct size, and information on delay between onset of symptoms and arrival at hospital, which are not routinely available in hospital records, might be predisposed elements to a less survival rate in the long term after a coronary event. These data were not available for the analysis. Socioeconomic status and educational level were not represented as collectable in the clinical records of the patients and could be misleading variables, as has been described in some studies. 30,31 The differentiation between patients with or without STEMI or unstable angina which might show clear examples of anticipated risk has not been considered because the study’s objective was the overall analysis of the approach to the patient at their admission for a coronary event. The evaluation of biomarkers, such as troponin concentration or peak creatine kinase activity, as predictors of mortality risk, was excluded from the study.
The adherence to treatment may affect the attainment of the objectives. The study assumed the prescriptions given by the primary care physician were accompanied with an adequate therapeutic compliance on the part of the patient. This issue is important to be considered as a limitation of the study due to the expected impact of the adherence on the final results. Nevertheless, it might be assessed as an adjusted result to the real consumption behavior of patients with chronic diseases.
In conclusion, results from this study indicate an increasing tendency in dying after a coronary event, which is aggravated by chronic diseases such as hypertension and diabetes. Current chronic medications present a clear protective effect for the patient, both in the short and long term, with contributions in the reduction of mortality from 0.3% (β-blocker) to 7% (aspirin) monthly. This benefit might be increased promoting an adequate therapeutic compliance to treatments. Health-care systems should face the future with preventive strategies that set out to reinforce the chronic use of primary optimal medications in patients who have suffered coronary events, as well as enabling heart-friendly healthier lifestyles.
Footnotes
Author Contributions
MC Montero-Balosa contributed to conception and design, contributed to acquisition, analysis and interpretation, and drafted the manuscript. R. Fernández-Urrusuno contributed to design and interpretation. Angel Vilches-Arenas contributed to conception and design, and contributed to analysis and interpretation. All authors critically revised the manuscript, gave final approval, and agreed to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Andalusian Regional Ministry of Health through a research project in Spain.