
Abstract
CHA2DS2-VASc score includes similar risk factors for coronary artery disease. We hypothesized that admission CHA2DS2-VASc score might be predictive of adverse clinical outcomes for patients with ST-segment elevation myocardial infarction (STEMI) who were undergoing primary percutaneous coronary intervention. A total of 647 patients with STEMI enrolled in this study. The study population was divided into 2 groups according to their admission CHA2DS2-VASc score. The low group (n = 521) was defined as CHA2DS2-VASc score ≤2, and the high group (n = 126) was defined as CHA2DS2-VASc score >2. Patients in the high group had significantly higher incidence of in-hospital cardiovascular mortality (8.7% vs 1.9%; P < .001). Long-term mortality was significantly frequent in the high group (13.4% vs 3.6%, P < .001). Hypertension, admission CHA2DS2-VASc score, and Killip class >1 were independent predictors of long-term mortality. Admission CHA2DS2-VASc score >2 was identified as an effective cutoff point for long-term mortality (area under curve = 0.821; 95% confidence interval: 0.76-0.89; P < .001). CHA2DS2-VASc score is a simple, very useful, easily remembered bedside score for predicting in-hospital and long-term adverse clinical outcomes in STEMI.
Introduction
Many scoring systems have been developed for risk stratification of ST-segment elevation myocardial infarction (STEMI). The Thrombolysis in Myocardial Infarction (TIMI) risk score, the Primary Angioplasty in Myocardial Infarction (PAMI) risk score, the Global Registry of Acute Cardiac Events (GRACE) risk score, the Zwolle primary percutaneous coronary intervention (PCI) risk index, and the Controlled Abciximab and Device Investigation to Lower Late Angioplasty Complications (CADILLAC) risk score are well-known scores for predicting in-hospital and long-term mortality in patients with STEMI. 1 –6 Synergy Between Percutaneous Coronary Intervention With TAXUS and Cardiac Surgery (SYNTAX) score has been developed angiographic variables for evaluation of coronary artery disease (CAD) complexity, which is associated with in-hospital and long-term clinical outcomes in patients with STEMI. 7 The CHA2DS2-VASc score, which has been developed from CHADS2, is easily remembered, well validated, and recommended in practice guidelines for oral anticoagulant therapy in patients with nonvalvular atrial fibrillation (NVAF). 8 Both CHADS2 and CHA2DS2-VASc scoring systems include similar risk factors for CAD. Previous studies have shown the relationship between CHADS2 and CHA2DS2-VASc scores and not only CAD but also acute coronary syndrome (ACS). 9 –12 The impact of admission CHA2DS2-VASc score and in-hospital and long-term unfavorable clinical outcomes in patients with STEMI who were undergoing primary PCI has not yet been investigated. Thus, the aim of this study was to evaluate the association between admission CHA2DS2-VASc scores and in-hospital and long-term clinical outcomes in patients with STEMI.
Methods
There were 647 consecutive patients with STEMI (550 men and 97 women with a mean age of 56.6 ± 12.3 years) admitted to the emergency department of the Siyami Ersek Thoracic and Cardiovascular Surgery Center between January 2010 and December 2010, all of whom were enrolled in this prospective study. The study inclusion criteria are (1) typical chest pain persisting >30 minutes, presenting within 12 hours from the onset of symptoms, (2) ST-segment elevation ≥1 mm and at least 2 contiguous electrocardiography (ECG) leads or new left bundle branch block with increasing cardiac enzymes twice the upper limit of normal within 12 hours of symptom onset, and (3) treatment with primary PCI (angioplasty and/or stent implantation).
The study population was divided into 2 groups according to their admission CHA2DS2-VASc score. The low group (n = 521) was defined as CHA2DS2-VASc score ≤2, and the high group (n = 126) was defined as CHA2DS2-VASc score >2. The study protocol was approved by the ethics committee of the authors’ hospital.
Analysis of Patient Data
The patients’ clinical and demographic characteristics; risk factors such as hypertension (HT), diabetes mellitus (DM), smoking, and hypercholesterolemia; and history of stroke or transient ischemic attack (TIA), heart failure (HF), and vascular disease were recorded.
The CHA2DS2-VASc score was calculated by assigning 1 point each for the presence of HF, HT, DM, age of 65 to 74 years, female sex, and vascular diseases and 2 points for age ≥75 years and a history of stroke or TIA. Angina-to-reperfusion time and door-to-balloon time were noted.
Blood samples were obtained at the time of hospital admission and daily during the hospital stay. A 12-lead ECG was recorded in each patient just after hospital admission, and the type of myocardial infarction (MI) was noted from ECG. Biochemical measurements were performed using Siemens Healthcare Diagnostic Products kits and calibrators (Marburg, Germany). Estimated glomerular filtration rate (eGFR) was calculated by the simplified Modification of Diet in Renal Disease formula. 13 Transthoracic echocardiography was performed using a Vivid 7 system (GE Vingmed Ultrasound AS, Horten, Norway) with a 2.5 MHz phased-array transducer with the left lateral decubitus position. The left ventricular ejection fraction (LVEF) was measured using the modified Simpson method. 14
Coronary Angiography, Primary Angioplasty, and Stenting
All patients received chewable 300 mg aspirin (unless contraindicated) and clopidogrel 600 mg (loading dose) before coronary angiography. The patients’ angiographic data were obtained from the cardiac catheterization laboratory records. Emergency coronary angiography and angioplasty were performed by the percutaneous femoral approach. The contralateral artery was first injected, and after visualizing the coronary arteries, 2.5 mg of nitrate was injected into the infarct-related artery (IRA) to rule out possible coronary spasm. The IRA was evaluated according to the TIMI classification. 15 Heparin (100 U/kg) was administered when arterial anatomy was defined. Angiographic assessments were made by visual evaluation. Primary PCI, including balloon angioplasty/stent implantation, was performed only for IRA according to lesion anatomy. For each procedure, interventional success at the acute phase is defined as reducing to <50% of obstruction and stenosis of the IRA with TIMI 2 or 3 flow just after primary PCI. After angioplasty, all patients were admitted to the intensive care unit, where 100 mg of aspirin and 75 mg of clopidogrel were continued in all patients. The use of glycoprotein IIb/IIIa inhibitors was left to the discretion of the operator. Concomitant medical treatment with statins, angiotensin-converting enzyme inhibitors, and β-blockers were given according to American College of Cardiology/American Heart Association guidelines.
Definitions
Hypertension was defined as the previous use of antihypertensive medications, systolic pressure ≥140 mm Hg, or diastolic pressure ≥90 mm Hg. Diabetes mellitus was defined as the use of insulin or antidiabetic agents in the patient’s medical history or a fasting glucose level ≥126 mg/dL. Chronic HF was defined as reduced LVEF <40%. Vascular disease was defined as previous MI, peripheral arterial disease (PAD), or complex aortic plaques. Hypercholesterolemia was defined as total cholesterol of at least 200 mg/dL. Multivessel disease was defined as a stenosis of more than 50% in all 3 major epicardial coronary arteries. Reperfusion time was measured as the time from symptom onset to the coronary reperfusion obtained with balloon inflation. Door-to-balloon time was defined as the time between hospital admission and balloon inflation. Patients were evaluated according to Killip clinical examination classification. 16 Cardiogenic shock was defined as systolic blood pressure <90 mm Hg for >30 minutes or as catecholamines required to maintain systolic pressure >90 mm Hg and clinical signs of pulmonary congestion and impaired organ perfusion. 17 Cardiovascular death was defined as unexplained sudden death, that is, death due to acute MI, HF, or arrhythmia. Repeat target vessel revascularization (TVR) was defined as the need for PCI or coronary surgery because of restenosis or reocclusion of the IRA. Reinfarction was described as elevation in serum creatinine kinase-MB enzyme levels by twice the upper limit of normal and ST-segment re-elevations.
Follow-Up
All patients were followed up for 6 months after discharge using a standardized protocol that included outpatient visits, telephone contacts, and recording of cardiac events. The primary end point was all-cause mortality. Major adverse cardiac events (MACEs) were defined as cardiovascular death, reinfarction, and repeat TVR. During long-term follow-up, stroke, heart failure-related rehospitalization, and MACE were noted.
Statistical Analysis
Quantitative variables were expressed as mean value ± standard deviation (SD), and qualitative variables were expressed as percentages (%). Comparisons of parametric values between 2 groups were performed with a 2-tailed Student t test. Categorical variables were compared with the likelihood ratio χ2 test or Fisher exact test. A backward stepwise Cox regression analysis, which included variables with P < .1, was performed to identify predictors of all-cause mortality. History of HT, age, female gender, CHADS2, CHA2DS2-VASc, hypercholesterolemia, reperfusion time, Killip class >1, history of HF, history of stroke or TIA, admission eGFR, admission glucose, admission hemoglobin, multivessel disease, and unsuccessful intervention were included into the model. The cumulative survival curves for all-cause mortality were constructed using Kaplan-Meier method, with differences assessed with the log-rank test. P value < .05 was considered statistically significant. All statistical studies were carried out using SPSS version 15.0 (SPSS Inc, Chicago, Illinois).
Reproducibility
The analyses were repeated twice 1 day later, by the same observer, in order to assess intraobserver variability, which was calculated by the average difference between the 10 measurements realized. A second independent observer repeated the analyses for the assessment of interobserver variability, which was calculated as the absolute difference divided by the average of the 2 observations for all parameters. In this study, the intraobserver and interobserver variability were 6.9% and 8.1%, respectively.
Results
Baseline Characteristics
The baseline demographics and clinical data of the patients are listed in Table 1. The mean age of the study population was 56.6 ± 12.3 years, and 97 of the patients were female. Compared with the low group, the patients in the high group were older and predominantly women. History of HT, DM, stroke or TIA, MI, hypercholesterolemia, HF, and PAD were more prevalent in the high group. Additionally, patients in the high group had a higher admission Killip class >1 (10.3% vs 5.5%; P = .05) and low LVEF (42 ± 9.3 vs 46.12 ± 8.2; P < .001). Door-to-balloon time, reperfusion time, admission systolic blood pressure, and admission heart rate were similar between the 2 groups.
Baseline Characteristics of the Study Patients.a,b
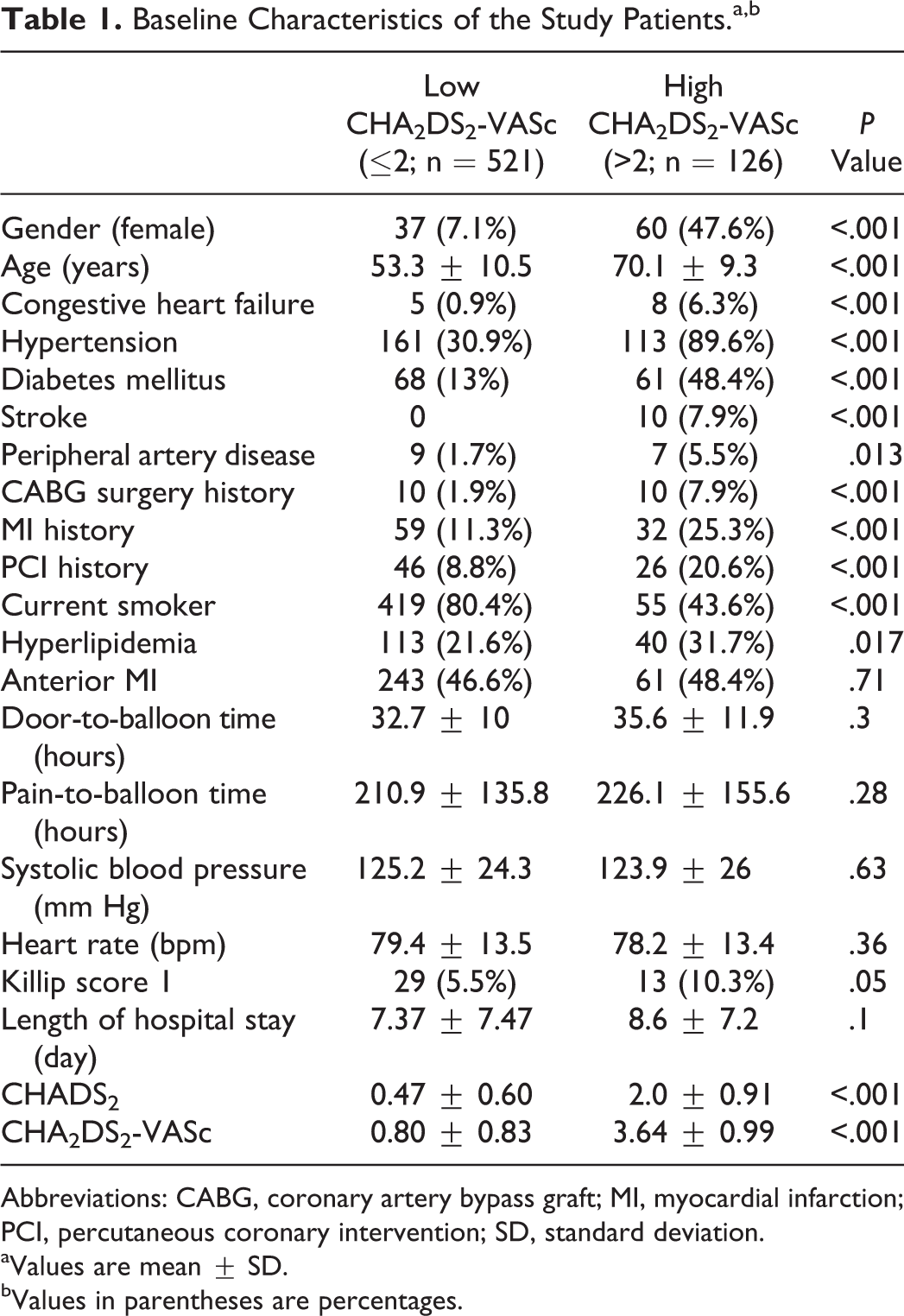
Abbreviations: CABG, coronary artery bypass graft; MI, myocardial infarction; PCI, percutaneous coronary intervention; SD, standard deviation.
aValues are mean ± SD.
bValues in parentheses are percentages.
Laboratory Findings
Table 2 lists the patients’ laboratory data. Admission creatinine (1.06 ± 0.46 mg/dL vs 0.86 ± 0.28 mg/dL; P < .001) and glucose level (185.1 ± 86.8 mg/dL vs 152.9 ± 65.4 mg/dL; P < .001) were higher in the high group. Patients in the high group had lower admission hemoglobin levels (12.9 ± 1.7 g/dL vs 14.4 ± 1.9 g/dL; P < .001).
Laboratory Findings of the Patients.a
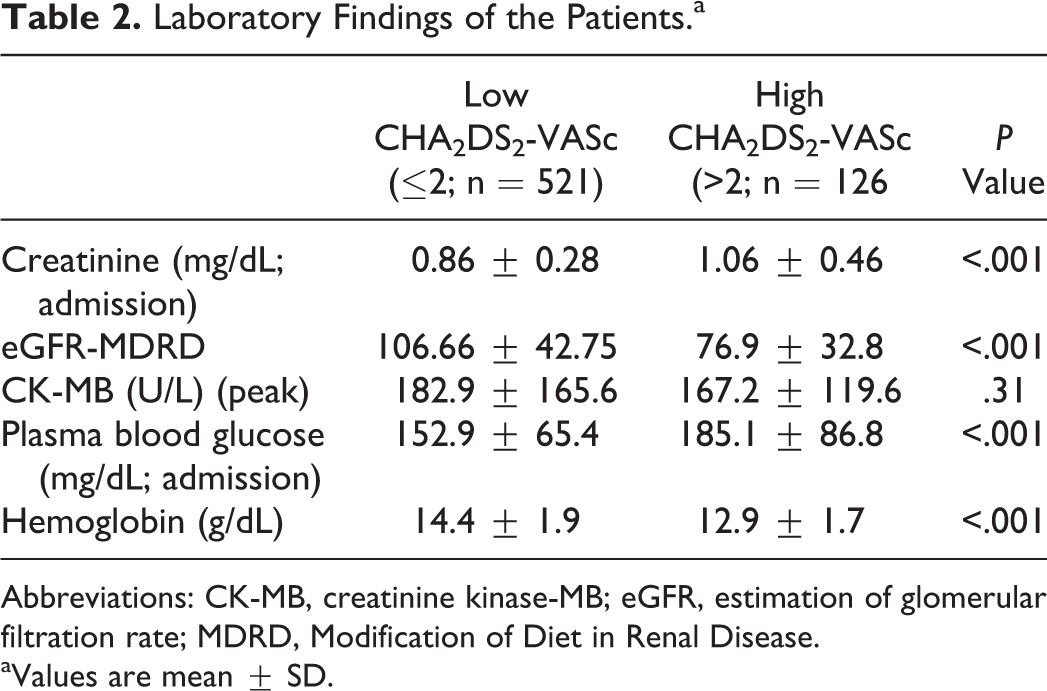
Abbreviations: CK-MB, creatinine kinase-MB; eGFR, estimation of glomerular filtration rate; MDRD, Modification of Diet in Renal Disease.
aValues are mean ± SD.
Angiographic and Procedural Characteristics
Angiographic and procedural characteristics are shown in Table 3. Multivessel disease was more frequent in the high group (23% vs 15.3%; P = .04). Culprit lesion, tirofiban use, successful procedure, and stent use were not statistically different between the 2 groups.
Angiographic and Procedural Characteristics of Study Patients.a
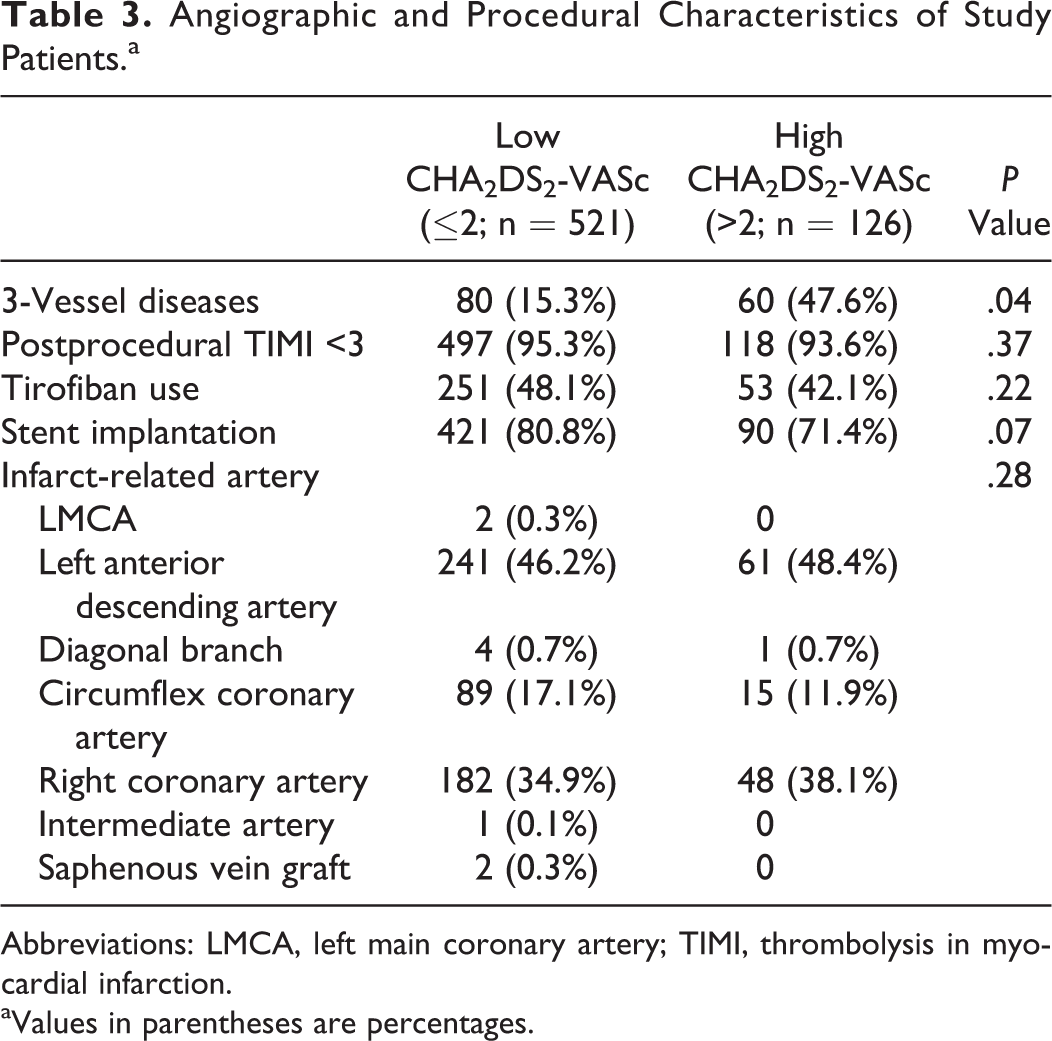
Abbreviations: LMCA, left main coronary artery; TIMI, thrombolysis in myocardial infarction.
aValues in parentheses are percentages.
In-Hospital and Long-Term Outcomes
Table 4 presents in-hospital outcomes after primary PCI. Patients in the high group had significantly higher incidence of in-hospital cardiovascular mortality (8.7% vs 1.9%; P < .001). The MACE, cardiogenic shock, in-hospital hemodialysis treatment, red blood cell transfusion, and complete atrioventricular block requiring transient pacemaker were more frequent in the high group.
In-Hospital Outcomes.a,b
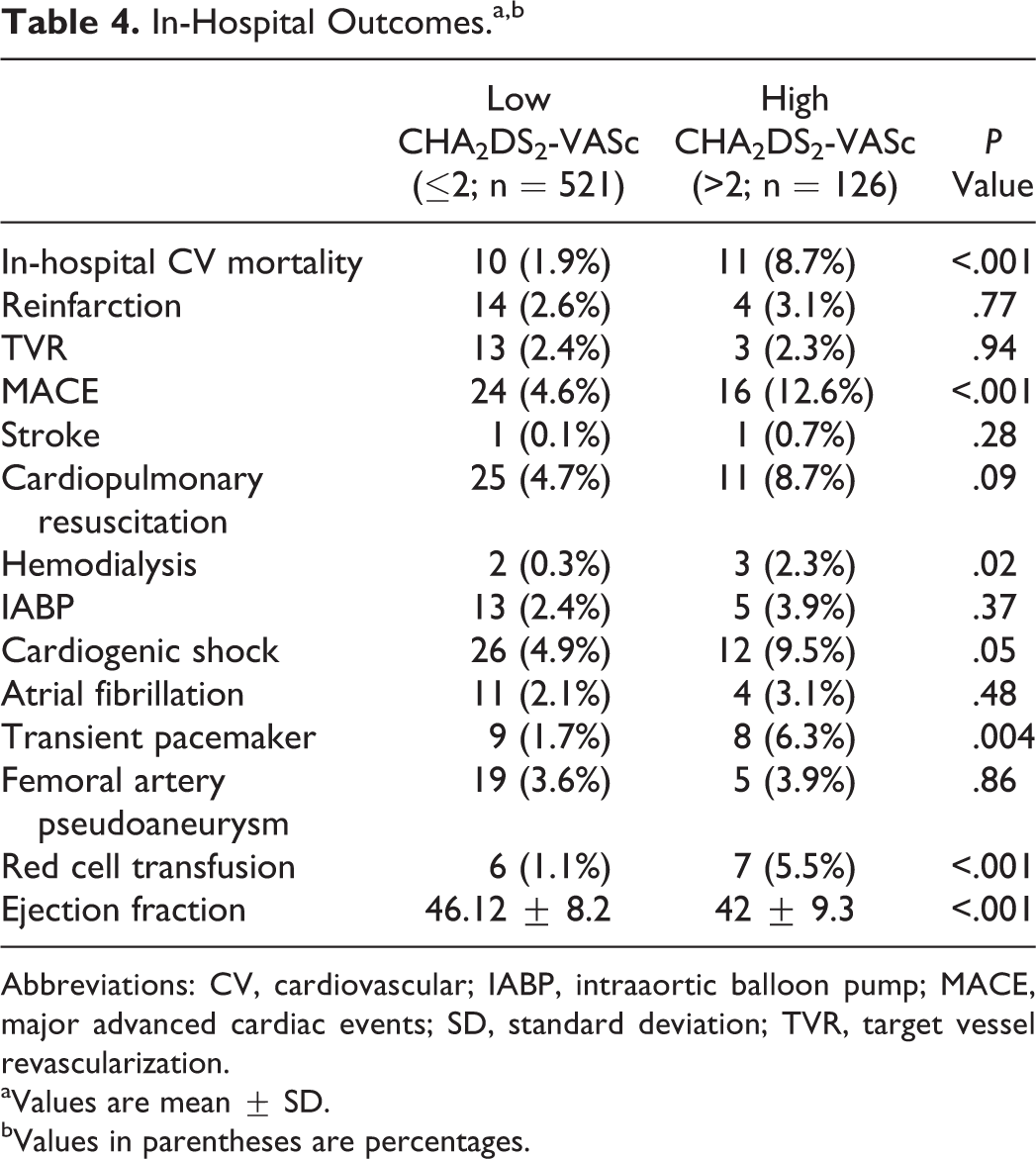
Abbreviations: CV, cardiovascular; IABP, intraaortic balloon pump; MACE, major advanced cardiac events; SD, standard deviation; TVR, target vessel revascularization.
aValues are mean ± SD.
bValues in parentheses are percentages.
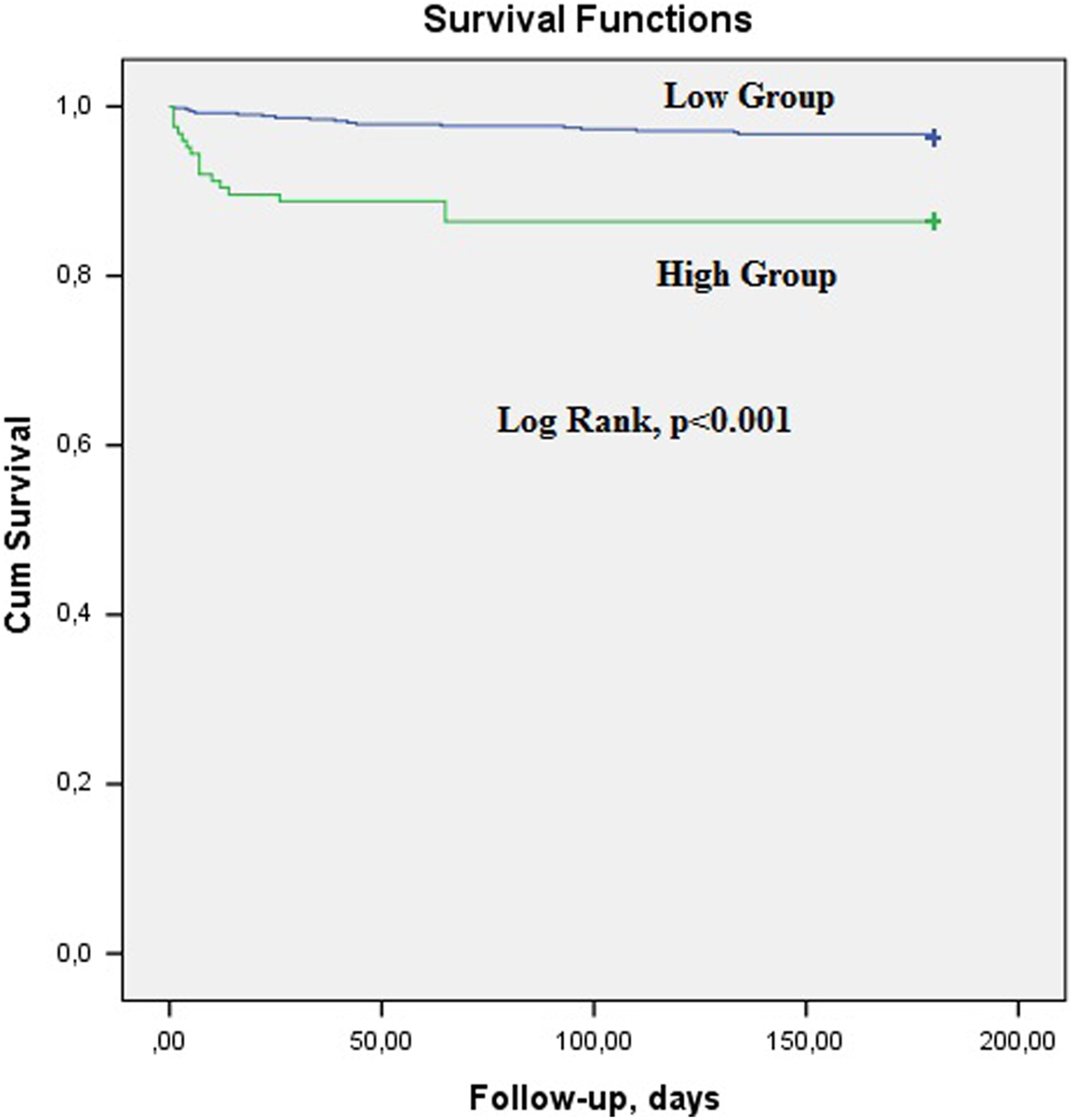
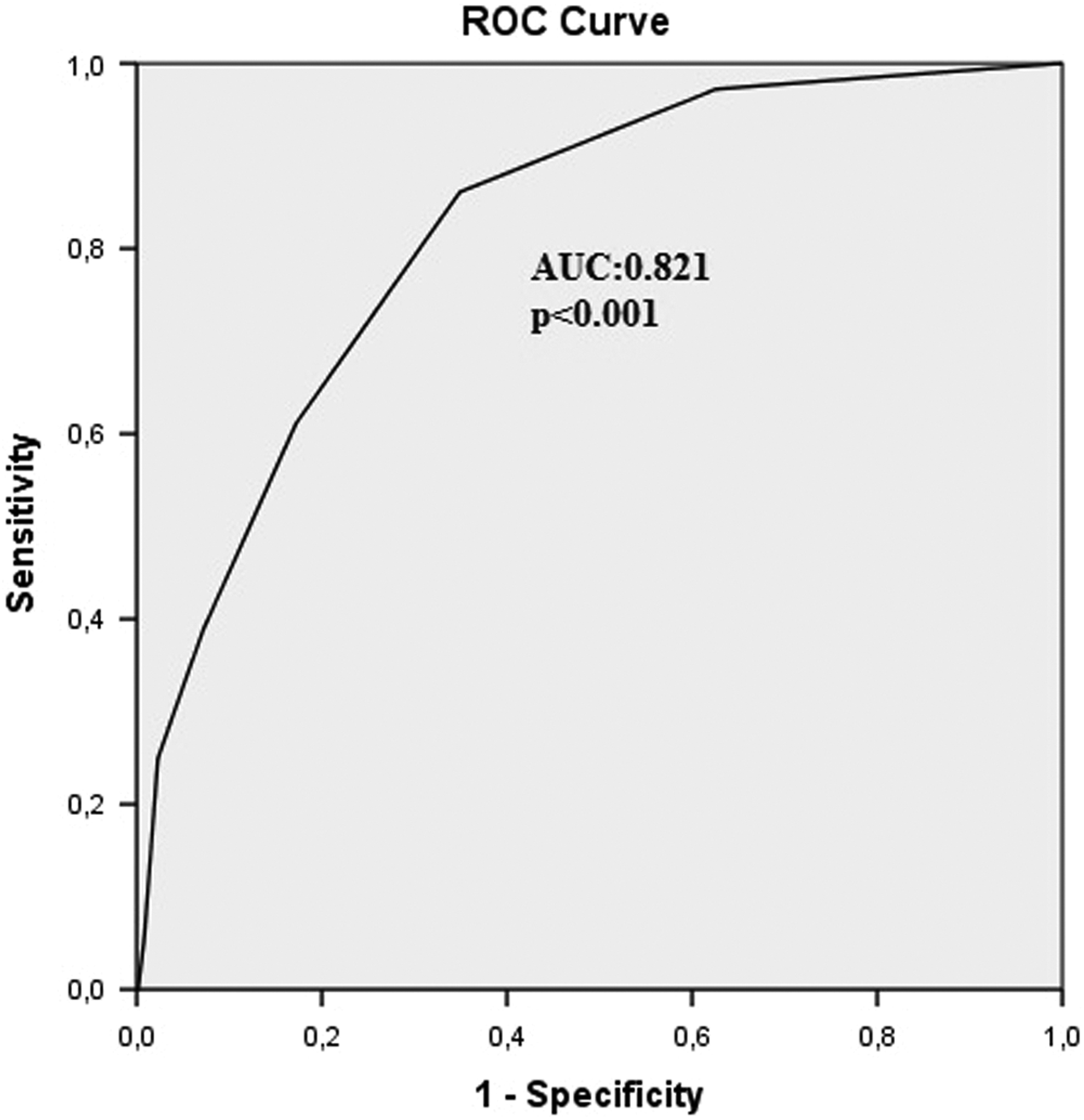
Table 5 shows long-term unfavorable clinical outcomes. In the Kaplan-Meier survival analysis, long-term mortality was 13.4% in the high group and 3.6% in the low group (P < .001; Figure 1), and all of the deaths were cardiovascular in nature. Patients in the high group also had significantly higher MACE and reinfarction rates. The Cox regression analysis was used to identify predictors of long-term mortality. History of HT (odds ratio [OR]: 6.2, 95% confidence interval [CI]: 2.05-18.8, P < .001), admission CHA2DS2-VASc score (OR: 1.77, 95% CI: 1.28-2.45, P < .001), and Killip class >1 (OR: 13.2, 95% CI: 5.94-29.5, P < .001) were independent predictors of long-term mortality (Table 6). Admission CHA2DS2-VASc score >2 was identified as an effective cutoff point for long-term mortality (area under curve = 0.821; 95% CI: 0.76-0.89; P < .001), and it had a sensitivity of 61.1% and a specificity of 82.8% (Figure 2).
Long-Term Follow-Up.a
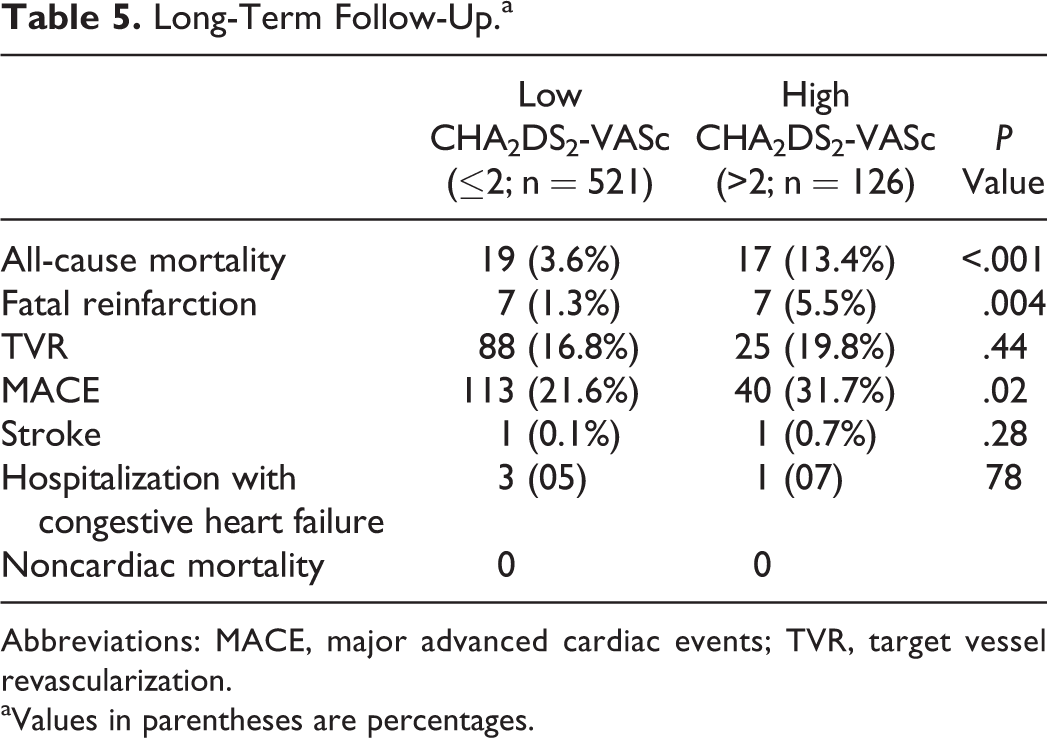
Abbreviations: MACE, major advanced cardiac events; TVR, target vessel revascularization.
aValues in parentheses are percentages.
The receiver–operating characteristic curve for admission CHA2DS2-VASc score >2 was identified as an effective cutoff point for long-term mortality (area under curve = 0.821; 95% CI: 0.76-0.89; P < .001) with a sensitivity of 61.1% and a specificity of 82.8%. CI indicates confidence interval.
Cox Regression Long-Term Mortality.
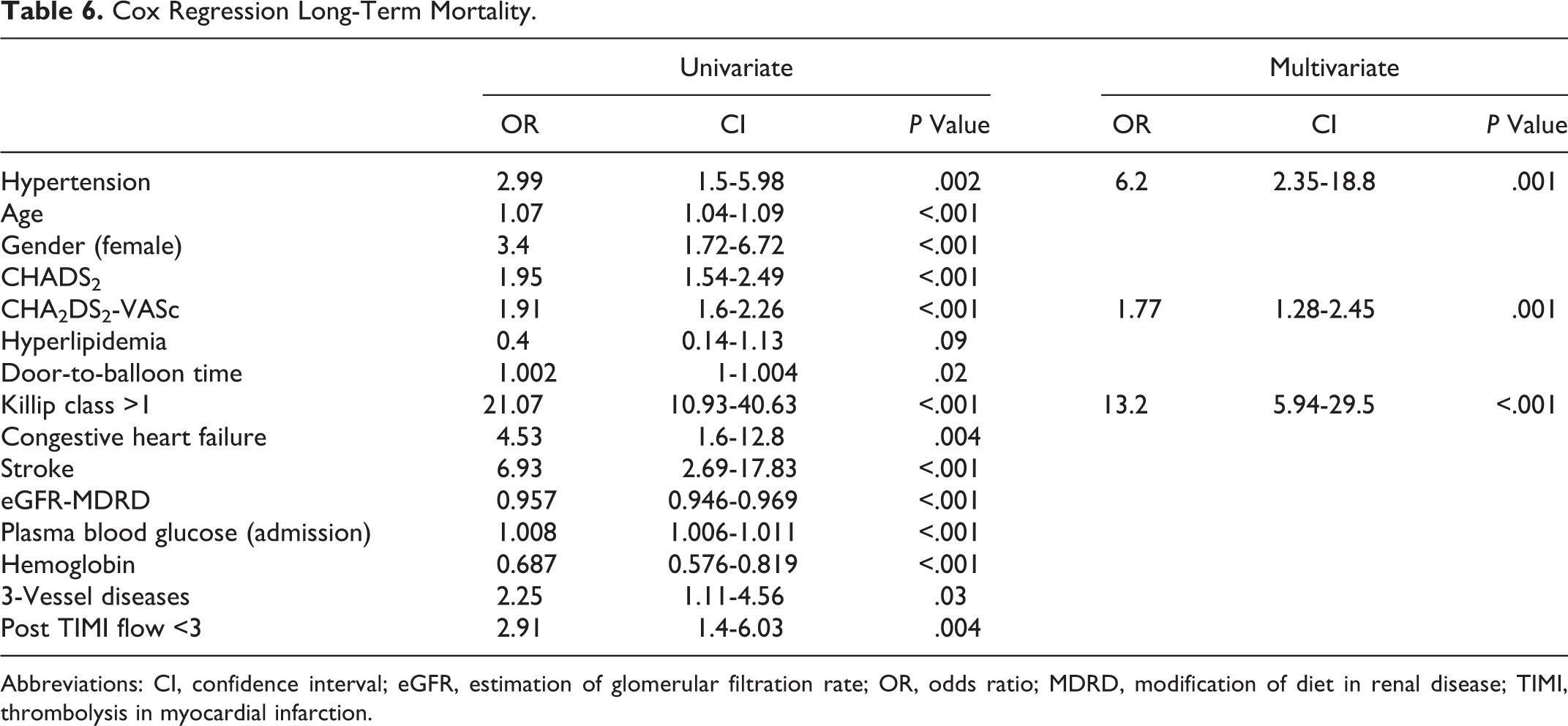
Abbreviations: CI, confidence interval; eGFR, estimation of glomerular filtration rate; OR, odds ratio; MDRD, modification of diet in renal disease; TIMI, thrombolysis in myocardial infarction.
Long-term mortality of the low and high groups.
Discussion
The main findings of this present study were as follows: (1) patients in the high CHA2DS2-VASc group had a higher Killip class, a low LVEF level, and higher incidence of cardiogenic shock; (2) patients with a CHA2DS2-VASc score >2 had remarkable increase in in-hospital cardiovascular mortality, and (3) the CHA2DS2-VASc score was an independent predictor of long-term cardiovascular mortality in patients with STEMI.
CHA2DS2-VASc score, which has been developed from CHADS2, is recommended in practice guidelines for evaluating oral anticoagulant therapy in patients with NVAF. 8 The components of CHADS2 and CHA2DS2-VASc score comprise risk factors for CAD, and the relationship between CHADS2 and CHA2DS2-VASc score with CAD and ACS has been reported in previous studies. Poçi et al 9 evaluated 2335 patients with ACS and they reported that their CHADS2 scores were related to 10-year all-cause mortality in patients with and without AF. Chan et al 10 reported that both CHADS2 and CHA2DS2-VASc scores predict vascular dysfunction, new-onset ischemic stroke, MI, HF, and cardiovascular death in patients without AF. Cetin et al 11 investigated patients who underwent diagnostic angiography, and they found that CHADS2, CHA2DS2-VASc, and CHA2DS2-VASc-HL scores were significantly correlated with the number of diseased coronary vessels and the Gensini score. In this study, they have developed a new score named CHA2DS2-VASc-HL, in addition to the components of the CHA2DS2-VASc score with hyperlipidemia, smoking, and male rather than female gender. In a different large population study, Kim et al 12 evaluated 15 681 patients with ACS who showed that a CHA2DS2-VASc score was an important predictor of long-term mortality.
This present study revealed that CHA2DS2-VASc score was associated with an advanced Killip class, low LVEF level, and a higher incidence of in-hospital and long-term mortality. Several mechanisms might explain the association between CHA2DS2-VASc score and in-hospital and long-term cardiovascular mortality. Previous studies have reported that female gender, which is a component of the CHA2DS2-VASc score, predicts in-hospital and long-term mortality in patients with STEMI. Ayhan et al 18 investigated 2644 patients with STEMI and they found that stroke, cardiogenic shock, and in-hospital and long-term mortality were higher in female gender. Age is a powerful predictor of cardiovascular mortality in STEMI; therefore, it is the main component of risk classification scores, such as TIMI and PAMI risk scores, GRACE risk index, Zwolle primary PCI risk index, and CADILLAC risk score. 2 –6 The DM is another important predictor of adverse cardiovascular events in patients with STEMI, and also the component of TIMI and PAMI risk scores. 3,6 Ergelen et al 19 examined 2529 patients with STEMI who were treated with primary PCI, and they showed that DM and age were predictors of in-hospital and long-term cardiovascular mortality. The HT is well known as a predictor of in-hospital and long-term mortality in patients with STEMI and AMI. 20,21 Cooper et al 22 found that prior stroke was associated with short-term mortality in patients with STEMI. The components of CHA2DS2-VASc scores are predictors of in-hospital and long-term cardiovascular outcomes in patients with STEMI, and these findings were correlated with our results. In our study, patients in a high CHA2DS2-VASc group had a higher incidence of female gender, older age, HT, DM, HF, prior stroke, and PAD. Therefore, our findings might be related to these well-known predictors for cardiovascular mortality in STEMI.
Identifying high-risk patients with STEMI is important, and different scoring systems have been developed for risk stratification. The TIMI risk score, GRACE risk index, Zwolle primary PCI risk index, and CADILLAC risk score are widespread tools for predicting in-hospital and long-term mortality in STEMI. 2 –5 The GRACE risk score is useful for predicting in-hospital all-cause mortality in patients with ACS, but this score is a very detailed system because of data from physical examination and laboratory tests. Although TIMI risk score for STEMI is another useful system, it includes various demographic and electrocardiographic parameters and physical examination findings, and it is not a real-life scoring system because it has been developed based on fibrinolytic therapy. 3 Also, the Zwolle primary PCI risk index, CADILLAC, SYNTAX, and PAMI risk scores include different clinical, demographic, angiographic, echocardiographic, and electrocardiographic parameters and signs of physical examination. These scoring schemes are not practical for physicians because of multiplicity and complexity.
In our study, we found that CHA2DS2-VASc score >2 was associated with cardiogenic shock, high Killip class, low LVEF, fatal reinfarction, and in-hospital and long-term mortality. This is the first study to evaluate the association between admission CHA2DS2-VASc score and in-hospital and long-term unfavorable clinical outcomes in patients with STEMI who were undergoing primary PCI. The CHA2DS2-VASc score is a simple, very useful, easily remembered bedside score for predicting in-hospital and long-term adverse clinical outcomes in STEMI.
Study Limitations
This study has several limitations because it was a single-center design and nonrandomized study. It is subject to selection bias; however, we were careful to include consecutive patients. We did not calculate CADILLAC risk score; Zwolle primary PCI risk index; TIMI, PAMI, and GRACE risk scores; and SYNTAX score. Reperfusion markers, such as myocardial blush grade or ST resolution, could not be determined. Despite adjusting for multiple risk factors, there may have been confounding conditions and medications. In addition, follow-up time was no longer compared to other studies.
Conclusion
Our findings indicate that the CHA2DS2-VASc score was related to in-hospital and long-term unfavorable clinical outcomes in patients with STEMI who were undergoing primary PCI. The CHA2DS2-VASc score is a simple, very useful, easily remembered score for risk stratification in patients with STEMI.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.