
Abstract
Introduction
Lupus anticoagulant (LA) is one of the laboratory diagnostic criteria for antiphospholipid antibody syndrome (APS) and is an established risk factor for thrombosis. 1 It can also be detected transiently in patients with infections or underlying malignancies and in patients using certain drugs. 2 In laboratory, LA status is determined via a functional assay, which shows that a phospholipid-dependent clotting time is prolonged and the prolongation is corrected by adding excessive phospholipid. 1 Persistent LA is the most representative acquired risk factor for thrombosis, but the significance of transient LA varies depending on the clinical situation. 2
It is well known that SARS-CoV-2 (COVID-19) infection is associated with a unique hypercoagulable state and thrombosis and its features overlap partially with other types of coagulopathy including APS.3–5 Until now, studies have reported hypercoagulability and high prevalence of LA and antiphspholipid antibodies (aPLs) in patients with COVID-19 infection.6–9 However, whether LA or aPLs contribute to the hypercoagulable states of COVID-19 has been disputed. Studies suggest that LA is more prevalent than other aPLs in COVID-19 infection, and LA or aPL positivity is possibly associated with more severe disease.7–9 However, the association between LA or aPL positivity and thrombotic complications or mortality is still unclear.7–9 In addition, most studies conducted to date have major drawbacks. Some of them did not consider variables such as C-reactive protein (CRP) or the anticoagulant effect due to unfractionated heparin (UFH), low-molecular-weight heparin (LMWH), and direct oral anticoagulants (DOACs), which can affect LA test results. In addition, only few studies investigated the persistence of LA or aPL positivity in COVID-19 infection.10,11 To the best of our knowledge, none of the studies reported the exact timing of the positive LA test result during COVID-19 infection.
This study investigated the clinical significance of LA results in hospitalized patients with reverse-transcription polymerase chain reaction (RT-PCR)-confirmed COVID-19 infection. We determined the prevalence of LA in COVID-19 infection and significant changing patterns in LA positivity to identify the timing of the positive LA test result during the course of infection and hospitalization. Additionally, we investigated the association between LA positivity or the changing pattern in LA results and the clinical course and laboratory results.
Materials and Methods
Patients and Data Collection
The study included 41 patients with RT-PCR-confirmed COVID-19 infection who were hospitalized between June 2020 and March 2021 in Soonchunhyang University Cheonan Hospital. We reviewed medical records of each patient to investigate the anticoagulant type and dose to determine the effect on LA result. We recorded the dates of administration if any anticoagulants such as UFH, LMWH, and DOAC were used in a patient. The course of COVID-19 infection including survival and death was also studied. Lastly, laboratory results of each patient including complete blood counts (CBC), erythrocyte sedimentation rate (ESR), prothrombin time (PT), activated partial thromboplastin time (aPTT), fibrinogen, fibrinogen degradation product (FDP), D-dimer, LA, and C-reactive protein (CRP) were collected. LA assay was performed with both dilute Russell's viper venom time (dRVVT) and aPTT-based silica clot time (SCT) (HemosIL, dRVVT and HemosIL SCT, Werfen, Barcelona, Spain), according to ISTH guidelines. 1 In other words, dRVVT and SCT screening assays were performed in all patient and if any test showed a positive result, confirmatory test with the same system was carried out. The cut-off ratios for each confirmatory test were as follows: dRVVT 1.21, and SCT 1.26. All laboratory tests including LA test were performed at least once in every patient during hospitalization.
Disease severity of COVID-19 infection was classified according to guidelines in response to coronavirus disease 2019 published by Korean Disease Control and Prevention Agency. 12 Mild COVID-19 was defined as infection without viral pneumonia or hypoxia. Moderate and severe disease were characterized by respiratory rate and oxygen saturation on room air. Severe infection requiring intubation was considered as critical disease. Thrombotic complications were confirmed when there was radiologic evidence of thrombosis or it was clinically suspected strongly based on the typical symptoms of thrombosis in each site. For example, complaints of acute exacerbation of dyspnea or chest pain and elevated D-dimer prompted a presumptive diagnosis of pulmonary embolism. 13
All enrolled patients were classified into two groups according to the frequency of positive LA test results: “LA (−)” (consistently LA negative) and “LA (+) ≥1” (positive for LA at least once). As the latter group showed inconsistent results, we hypothesized that the change in LA results was more important than the LA positivity. So, we divided it again according to the frequency of changes in LA test results: 0 (consistently positive LA results until discharge), 1 (LA results changed once: from (+) to (−) or vice versa), and ≥2 (LA results changed more than twice). In group “LA (+) ≥1”, the date of change in LA test result was recorded. Two date criteria were established: date of diagnosis (DD), which means the number of days after the COVID-19 infection was first confirmed by molecular test (DD0), and hospital day (HD), which refers to the number of days after transfer to the tertiary care hospital (HD1). Because HD does not accurately reflect the disease course and COVID-19 infection was generally established at the earliest detectable time due to proactive preventive measures of Korean government, we implemented the concept of DD in addition to HD.
To evaluate the clinical significance of LA positivity, disease severity, mortality and thrombotic complications were compared between LA (−) group and LA (+) ≥1 group. Also, the association between the changing pattern in LA results (negative to positive or positive to negative) or the frequency of change in LA test results and disease severity, mortality, and thrombotic complications were evaluated. Overall survival of each group was also compared.
To determine the possible difference in laboratory results during the course of infection or the course of hospitalization between groups “LA (−)” and “LA (+) ≥1”, laboratory results on DD 0 (at the time of initial diagnosis), 6 (a week before the first change in LA results), 12 (at the time of the first change in LA results), and 15 (at the time of second change in LA results) and on HD 1 (at the time of hospitalization), 9 (at the time of the first change in LA results), and the last day of hospital stay were compared. For this analysis, patients whose laboratory results (other than LA results) were recorded at less than two time points were excluded in this analysis because this analysis was focused on the change with time.
This study was approved by Institutional Review Board of the Soonchunhyang University Cheonan Hospital (2021-10-005).
Statistical Analysis
Categorical variables were compared via Chi-squared test or Fisher's exact test. Continuous variables were compared via t-test or Mann-Whitney test. The results were considered significant if the P value was < .05. IBM SPSS ver.26.0 (SPSS Inc., Chicago, IL, USA) was used to perform all statistical analyses.
Results
The characteristics of 41 patients are listed in Table 1. The median age of enrolled patient population was 72 years. No patient had been previously diagnosed as APS or other diseases that could cause LA positivity. Twenty-nine of the 41 patients survived, and 12 patients died. The median length of hospital stay was 14 days. Seven patients experienced thrombotic complications. The number of patients who had mild, moderate, severe, and critical COVID-19 infection at admission were 8, 7, 23, and 3, respectively. Ten out of 41 patients experienced disease aggravation during hospitalization.
Patient Demographics.

Twenty patients (48.8%) tested consistently negative for LA during hospitalization in the tertiary care hospital (LA (−) group), while 21 (51.2%) patients were positive for LA at least once (LA (+) ≥1 group). All positive results were confirmed in the dRVVT tests, suggesting that none of the SCT confirmatory tests were positive. The numbers of patients in subgroups of LA (+)≥1 were as follows: 0 (Consistently LA positive until discharge); 2 (4.9%), 1 (LA results changed once: from (+) to (−) or vice versa); 11 (26.8%), and ≥2 (LA results changed more than twice); 8 (19.5%). Two patients in the LA (+)≥1 group showed positive results in every LA test during their hospital stay and three of 11 patients in subgroup 1 (LA results changed once) tested negative during the early period of infection but consistently positive after a specific time point. On average, the first change occurred on DD12∼13 or HD9∼10, and the second change on DD15∼16 or HD13∼14 in LA (+) ≥1 group.
Age, sex, survival status, the results of CRP and coagulation tests, and the types and dates of anticoagulant administration of 20 patients in LA(−) group and 21 patients in LA (+)≥1 group are presented in supplementary Tables 1 and 2, respectively. The mean age in LA (−) group was 61.3 ± 19.6 years, with a male/female ratio of 8/12. The mean age in LA (+) ≥1 group was 75.19 ± 10.4 years, with a male/female ratio of 10/11. Between two groups, the mean age was significantly higher in LA (+) ≥1 group (P = .009), but the numbers of males and females were not significantly different (P = .623). With regard to other variables, only fibrinogen level was significantly higher in LA (+) ≥1 group (LA (−) group: 389.73 ± 94.59, LA (+) ≥1 group: 537.69 ± 112.45, P = .002) on HD1. There were no differences in CRP (P = .064), PT (P = .629), aPTT (P = .201), D-dimer (P = .296), AT (P = .900), and FDP (S = 0.082) between two groups on HD1.
Differences in Laboratory Results Before and After the Change in LA status {Results are Expressed as Median (Interquartile Range)}.
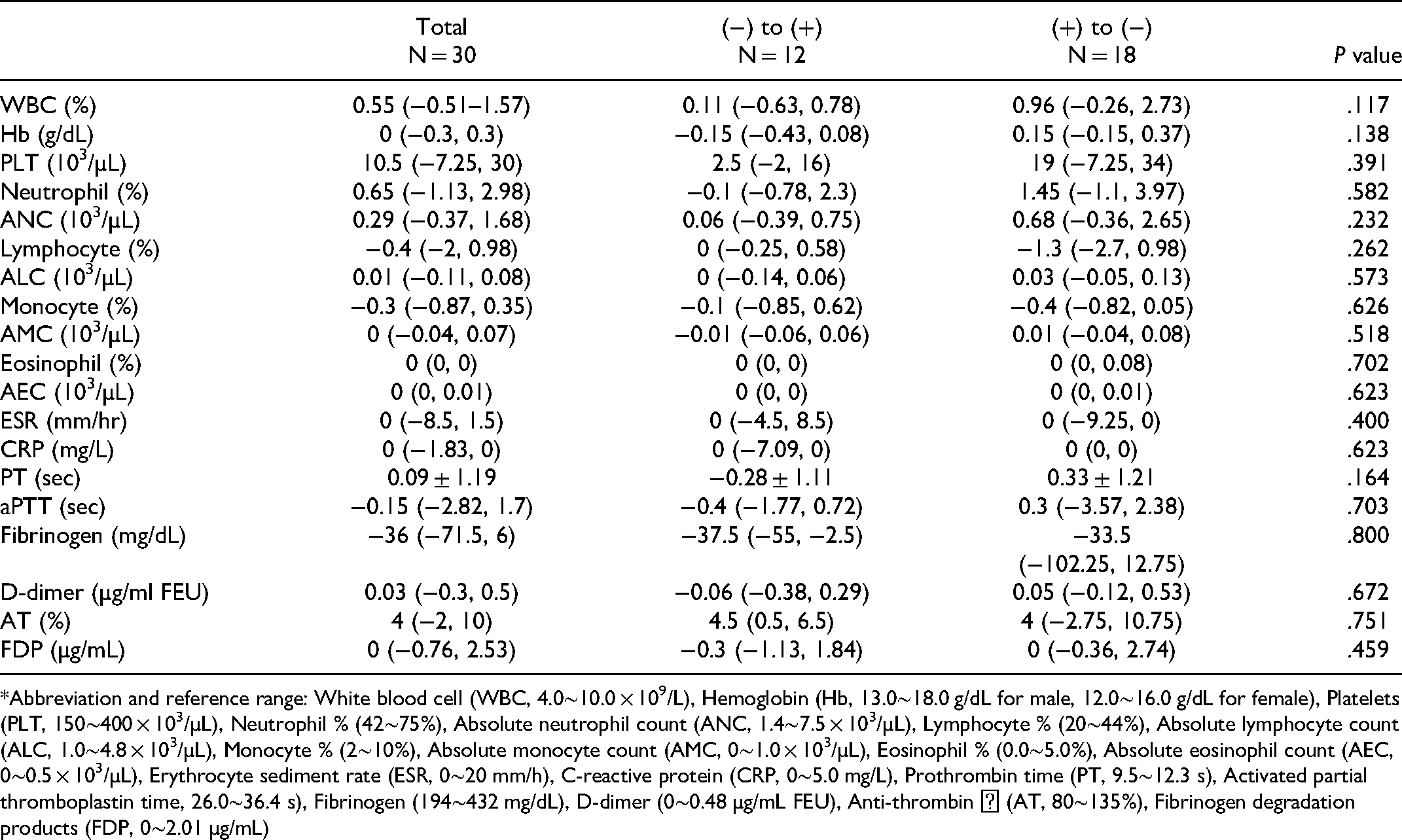
Abbreviation and reference range: White blood cell (WBC, 4.0∼10.0 × 109/L), Hemoglobin (Hb, 13.0∼18.0 g/dL for male, 12.0∼16.0 g/dL for female), Platelets (PLT, 150∼400 × 103/µL), Neutrophil % (42∼75%), Absolute neutrophil count (ANC, 1.4∼7.5 × 103/µL), Lymphocyte % (20∼44%), Absolute lymphocyte count (ALC, 1.0∼4.8 × 103/µL), Monocyte % (2∼10%), Absolute monocyte count (AMC, 0∼1.0 × 103/µL), Eosinophil % (0.0∼5.0%), Absolute eosinophil count (AEC, 0∼0.5 × 103/µL), Erythrocyte sediment rate (ESR, 0∼20 mm/h), C-reactive protein (CRP, 0∼5.0 mg/L), Prothrombin time (PT, 9.5∼12.3 s), Activated partial thromboplastin time, 26.0∼36.4 s), Fibrinogen (194∼432 mg/dL), D-dimer (0∼0.48 µg/mL FEU), Anti-thrombin Ⅲ (AT, 80∼135%), Fibrinogen degradation products (FDP, 0∼2.01 µg/mL)
The presence of LA was associated with more severe disease (P = .004); however, there was no statistically significant association with thrombotic complications and mortality (P = .410 and .353, respectively) (Figure 1). However, thrombotic complications occurred in 2 out of 20 patients (10.0%) in the LA (−) group, and 5 out of 21 patients (23.8%) in LA (+) ≥ 1 group. The number of deaths in each group was 4 out of 20 patients (20.0%) in the LA (−) group and 8 out of 21 patients (38.1%) in the LA (+) ≥ 1 group. Thus, the numbers of thrombotic complications and deaths were higher in the LA (+) ≥1 group than in the LA (−) group. There was no significant difference in overall survival between the two groups (Figure 2).

Differences in (A) disease severity, (B) presence of thrombotic complications, and (C) survival status between LA (−) and LA (+) ≥1 groups.

Comparison of Kaplan-Meier survival curves according to (A) hospital days (HD) and (B) date of diagnosis (DD).
LA results changed 30 times from (+) to (−) or vice versa in 21 patients belonging to LA (+) ≥1 group. There was no difference in the disease course (neither improved nor worsened) according to the changing pattern of LA results (P = .203). In addition, no significant differences in laboratory results were found before and after specific changes in LA (Table 2). Finally, the frequency of change in LA was not associated with disease severity, presence of thrombosis, or survival status (Table 3).
Clinical Implications of Changes in the Frequency of LA Results.

Significant differences in three parameters were found on DD6 between LA(−) and LA (+) ≥ 1 groups: eosinophil (P = .042) and absolute eosinophil count (P = .039) were significantly lower in LA (+) group, whereas CRP (P = .022) was significantly higher in LA (+) ≥1 group than in LA (−) group, which are well-known laboratory parameters associated with worse prognosis in COVID-19 infection.14–16 In addition, ESR was significantly higher in LA (+) ≥1 group on DD 12 (P = .026) (Figure 3). On HD9, both absolute neutrophil and lymphocyte counts were significantly lower in LA (+) ≥1 group than in LA (−) group (P = .031 and .004, respectively), which were also associated with worse clinical course of COVID-19 infection (Figure 4). 16

Laboratory results showing differences between LA (−) and LA (+) ≥1 groups on DD 6 and DD12: (A) Percent of eosinophils on DD6, (B) Absolute eosinophil count (AEC) on DD6, (C) C-reactive protein (CRP) on DD 6, and (D) Erythrocyte sediment rate (ESR) on DD 12.

Differences in laboratory results between LA (−) and LA (+) ≥1 groups on HD 9: (A) Absolute neutrophil count (ANC) on HD9 and (B) Absolute lymphocyte count (ALC) on HD9.
Discussion
LA positivity is common in COVID-19 infection, so its clinical implications have been investigated.7–9 However, most of the previous studies did not provide sufficient evidence to validate the results of LA tests. Thus, the possibility of false-positive results due to interference of CRP or anticoagulants was not eliminated.
In this study, the prevalence of LA was 51.2% among all the patients hospitalized with COVID-19, which was similar to the pooled prevalence of LA (46.8%) reported by a systematic review of 21 studies comprising a total of 1159 COVID-19 patients. 9 We confirmed that LA positivity was associated with severe disease, which was consistent with previous findings.7–9 Furthermore, lymphopenia, eosinopenia, and the increase in the levels of inflammatory markers were poor prognostic factors in COVID-19 infection and more severe in patients with LA (+) ≥1 than in LA (−). The change in laboratory parameters preceded the first change in LA results or appeared concurrently with the first change in LA results. These findings strengthen the association between LA positivity and worse clinical course.
Among all LA assays conducted in 41 patients (total 235 tests), 40 tests (17.0%) were positive, but only five of 40 positive tests were accompanied by prolonged aPTT. In this study, we used SynthasIL® (Instrumentation Laboratory, Milan, Italy) aPTT reagent, which has increased sensitivity to detect LA in clinical hospital laboratories. 17 Accordingly, the detection of LA without prolonged aPTT using the SynthasIL® aPTT reagent may indicate insufficient or weak LA, which failed to trigger thromboembolism in patients with COVID-19. According to ISTH guideline for LA assay, the combination of two different tests with different assay principles is recommended for enhanced sensitivity. 1 The dRVVT system is robust and specific for detecting LA in patients at high risk of thrombosis, while aPTT has high sensitivity for LA detection.1,18
The numbers of patients with suspected thromboembolism were not statistically different between LA (+) ≥1 group and in LA (−) group. There was no statistical difference in mortality either. This may be due to the small numbers of enrolled patients in this study. However, the numbers of thrombotic complications and deaths were higher in the LA (+) ≥1 group than in the LA (−) group. Therefore, we can conclude that there seems to be at least a trend that LA positivity is associated with thrombosis and mortality in COVID-19 patients although no significant association was confirmed statistically between LA positivity and thrombosis and mortality.
In our study, LA tests were performed more than once in every enrolled patient. Interestingly, most patients did not test positive for LA consistently. Only 5 of 21 patients in LA (+) ≥1 group (23.8%) tested positive consistently until the end of their hospital stay. No significant differences existed in disease severity, the presence of thrombotic complications and mortality between these five patients and the rest of LA (+) ≥1 group (P = .1073, > .99, and .0475, respectively). No significant changes in laboratory results or clinical conditions were found when LA results changed from negative to positive or from positive to negative.
Of note, our study minimized the likelihood of false-positive results caused by two most important variables, CRP and the use of anticoagulants. The level of CRP did not differ statistically between LA (+) ≥1 group and LA (−) group in every comparison except on DD6. Additionally, according to an experimental study, the CRP dose not interfere with the dRVVT test system19 and all the positive results in our study were based on the dRVVT test. Thus, we excluded the interference of CRP with LA assay. Anticoagulants frequently used in COVID-19 infection can interfere with the LA test results. Although some dRVVT or LA-specific aPTT reagents contain heparin neutralizers, UFH and LMWH can affect LA test results, especially in patients with supra-therapeutic anti-Xa levels. 1 Further, DOACs can also lead to false-positive LA results. 1 In this study, the possibility of false-positive LA test results due to anticoagulants was very low for the following reasons. First, the dRVVT and SCT reagents used in our study contained polybrene, which neutralized serum heparin up to 1 U/mL. Because all enrolled patients received preventive or therapeutic doses of UFH or LMWH, it was expected that they did not affect the LA result. Second, despite the failure to evaluate the effect of DOAC on LA results, no positive result was found during the half-life of administered DOAC. Finally, the numbers of patients with unpredictable effects of anticoagulants, ie, patients who were administered supratherapeutic doses of UFH and who were treated with more than two types of anticoagulants, were negligibly few in both groups each time during the comparison (0-2 patients at each time point).
This study has some limitations. First, the study population was relatively small. Because our study was implemented in a tertiary hospital, patients with mild-to-moderate disease were not as many as those with severe-to-critical disease. Among patients who were transferred to our hospital several days after confirmation of COVID-19 infection, no laboratory results were evaluated at an early stage of infection. Because screening imaging tests for asymptomatic patients and some of confirmatory imaging tests were omitted, thrombotic complications may have been over or underestimated. Although LA assay was performed repeatedly in every enrolled patient, the timing of the first LA test differed among patients and no LA tests were done according to strict criteria determining the test interval. Therefore, we could not compare the results of LA on the same DD or HD in each patient. Although the interference with LA results by anticoagulants was excluded for the reasons mentioned above, serum anticoagulant concentrations were not measured. And, because the overall survival rate was high and there was no severe complication, the follow-up test for LA was not performed. Finally, we did not evaluate the effect of aPLs other than LA, such as anti-cardiolipin and anti-β2-glycoprotein I antibodies, on the disease course or the occurrence of thromboembolic complications of COVID-19 infection.
In conclusion, LA positivity is one of the findings suggesting more serious COVID-19 infection. Although none of the analyses from various angles revealed statistically significant result, there was a trend of increasing death and thrombosis in LA (+) ≥1 group. The significance should be confirmed further studies with larger numbers of COVID-19 patients. Change in LA test does not show predictive ability either. Considering that previously established poor prognostic factors are included in a routine blood test for a hospitalized patient, additional LA test in a COVID-19 patient seems to be not an essential part because it does not provide further information regarding disease course. Further studies should be required to evaluate the exact relationship between LA positivity in COVID-19 and the presence of other antiphospholipid antibodies, including patients with side spectrum of disease severities.
Supplemental Material
sj-docx-1-cat-10.1177_10760296221127276 - Supplemental material for Association of Lupus Anticoagulant status with Disease Course in SARS-CoV-2 (COVID-19) Infection
Supplemental material, sj-docx-1-cat-10.1177_10760296221127276 for Association of Lupus Anticoagulant status with Disease Course in SARS-CoV-2 (COVID-19) Infection by Suhyeon Woo, MD, Bohyun Kim, MD, PhD, Nam Hun Heo, MS, Min-sun Kim, MD, Young Ahn Yoon, MD, and Young-Jin Choi, MD, PhD in Clinical and Applied Thrombosis/Hemostasis
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This study was supported by the Soonchunhyang University Research Fund.
Ethics Approval
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Ethics Committee of Soonchunhyang University (No. 2021-10-005).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.