
Abstract
Coronary artery disease (CAD) is a systemic chronic inflammatory disease, and serum fibrinogen and albumin are 2 important factors in systemic inflammation. We aimed to investigate the relationship between the fibrinogen–albumin ratio (FAR) and outcomes in patients with CAD who underwent percutaneous coronary intervention (PCI). All patients were from the Clinical Outcomes and Risk Factors of Patients with Coronary Heart Disease after PCI (CORFCHD-PCI) study, which is a retrospective cohort study (Identifier: ChiCTR-ORC-16010153) that includes a total of 6050 patients with CAD after PCI from January 2008 to December 2016. A total of 5829 patients with CAD after PCI were recruited in the present study. They were divided into 2 groups according to the FAR cutoff value, which was calculated using a receiver operating characteristic curve, a low group (FAR < 0.095, n = 3811), and a high group (FAR ≥ 0.095, n = 2018). The average follow-up time was 35.9 ± 22.6 months. The multivariate Cox proportional hazards model showed that FAR was independently correlated with all-cause mortality (adjusted hazard ratio [HR] = 1.432 [1.134-1.808], P = .003), cardiac mortality (adjusted HR = 1.579 [1.218-2.047], P = .001), major adverse cardiac and cerebrovascular events (adjusted HR = 1.296 [1.125-1.494], P < .001), major adverse cardiac events (adjusted HR = 1.357 [1.170-1.572], P < .001), and heart failure (adjusted HR = 1.540 [1.135-2.091], P = .006). The present study indicated that the FAR was associated with adverse outcomes in patients with CAD who underwent PCI.
Keywords
Introduction
Coronary artery disease (CAD) is a major cause of morbidity and death worldwide. The pathophysiological mechanisms of CAD are complex. Previous studies have confirmed that inflammation and oxidative stress lead to plaque rupture, and oxidative stress can further promote plaque rupture by stimulating inflammation. 1,2 Coronary artery disease is a chronic inflammatory state, and inflammation is involved throughout the pathological course of atherosclerosis. It is known that inflammatory markers are associated with increased adverse cardiac events in patients with CAD. 3 Albumin is an essential protein in human plasma. It has been proposed that the serum albumin concentration is related to inflammatory and hemostatic processes. 4,5 In addition, albumin can inhibit platelet activation. 6,7 Several studies have shown that serum albumin levels are inversely associated with cardiovascular mortality and morbidity. 8,9 Furthermore, lower albumin levels were reported to be significantly associated with long-term all-cause mortality (ACM) in acute myocardial infarction (AMI). 10 Additionally, hypoalbuminemia can predict the no-flow phenomenon in patients with AMI after percutaneous coronary intervention (PCI). 11 Fibrinogen, produced by the liver, serves as an indicator of the procoagulant state and plays a role in inflammatory responses at various levels. 12 Previous studies have shown that the plasma fibrinogen level is associated with the severity of CAD and may predict cardiovascular events in the general population. 13,14
Therefore, both fibrinogen and albumin are important factors of systemic inflammatory and hemorheological alterations. The fibrinogen–albumin ratio (FAR), comprising these 2 indicators, has been reported as a new inflammatory marker closely related to tumor progression and severity of CAD. 15 –18 However, the prognostic value of the FAR for patients with CAD who underwent PCI remains unclear. Therefore, the purpose of this study was to explore the relationship between the FAR and prognosis in patients with CAD who underwent PCI.
Methods
Study Design and Population
The design of the study has been described previously. 19 –21 Briefly, this is a single-center, observational, retrospective cohort study based on case records and follow-up registry. A total of 6050 patients with CAD who underwent PCI in the First Affiliated Hospital of Xinjiang Medical University from January 2008 to December 2016 were enrolled. The details of the design are registered at http://www.chictr.org.cn (identifier: ChiCTR-ORC-16010153). The PCIs were performed by experienced interventionalists in the Department of Cardiology at the First Affiliated Hospital of Xinjiang Medical University. As shown in Figure 1, Patients without baseline serum albumin and fibrinogen were excluded. A total of 5829 patients were included in the present study. The study protocol was reviewed and approved by the Ethics Committee of the First Affiliated Hospital of Xinjiang Medical University in accordance with the Declaration of Helsinki.
Clinical and Demographic Characteristics Collection
Clinical risk factors for CAD, such as demographic data, previously diagnosed diabetes mellitus (DM), history of hypertension (HP), smoking, drinking, family history of cardiovascular disease, and previous history of CAD, were recorded. The medical history, including the use of antiplatelet therapy, calcium channel blockers, angiotensin-converting enzyme inhibitors or angiotensin receptor blockers, β-blockers, and statins, was also recorded.
All patients had venous blood samples collected from the antecubital veins after admission; the blood collection was performed prior to coronary angiography. Fibrinogen, albumin, γ-glutamyl transferase (GGT), glucose (GLU), total bilirubin (TBil), blood urea nitrogen (BUN), creatinine (Cr), uric acid (UA), total cholesterol (TC), triglyceride (TG), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), apolipoprotein A1 (apo A-I), apolipoprotein B (apo B), and lipoprotein (a) were measured using standard methods in the Central Laboratory of the First Affiliated Hospital of Xinjiang Medical University.
End Points
The primary end points were long-term ACM and cardiac mortality (CM). Secondary end points were stroke, heart failure, bleeding events, readmission, major adverse cardiac events (MACEs), and major adverse cardiac and cerebrovascular events (MACCEs). Major adverse cardiac events were defined as combined cardiac death, recurrent myocardial infarction, and target vessel reconstruction. Major adverse cardiac and cerebrovascular events were defined as combined cardiac death, recurrent myocardial infarction, target vessel reconstruction, and stroke.
Follow-Up
All patients were scheduled for elective clinical follow-up at 1 month, 3 months, 6 months, 1 year, 3 years, and 5 years, and the longest follow-up time was 10 years. We clinically monitored the patients for cardiovascular events and medication status. The investigators followed up with the patients, either by office visits or by telephone contact, as necessary.
Statistical Analyses
All analyses were performed using SPSS 22.0 software (SPSS Inc). Continuous variables were expressed as the mean ± standard deviation, and categorical variables were expressed as the number of patients and percentages. The differences between the 2 groups were analyzed by independent t test or χ2 test. Multivariable analysis was performed to assess the predictive value of the FAR for outcomes during follow-up. Moreover, the variables found to be significant in the univariate model were included in the multivariate Cox model. The results are reported as hazard ratios (HRs) with their 95% CIs. A P < .05 (2-sided) was considered significant.
Results
Baseline Data
All patients were administered standard dual antiplatelet therapy during the first 6 months after PCI. The study included 5829 patients who were divided into 2 groups according to the FAR cutoff value, which was calculated using a receiver operating characteristic curve: a low group (FAR <0.095; n = 3811) and a high group (FAR ≥0.095; n = 2018). The baseline data are shown in Table 1. Several variables were significantly different between the 2 groups, including sex, GLU, TG, and HDL-C (all P < .05). There were no significant differences in age, smoking, alcohol consumption, DM, HP, BUN, Cr, TC, or LDL-C.
Characteristics of Participants of the 2 Groups.

Abbreviations: BUN, blood urea nitrogen; Cr, creatinine; FAR, fibrinogen–albumin ratio; GLU, glucose; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; TC, total cholesterol; TG, triglyceride; UA, uric acid.
Clinical Outcomes
There were 297 ACMs during the follow-up. The incidence of ACM in the high FAR group was 124 (6.1%) and in the low FAR group was 173 (4.5%). The ACM incidence was significantly higher in the high FAR group than in the low FAR group (P = .008). Cardiac mortality was significantly higher in the high FAR group than in the low FAR group (5.2% vs 3.5%, P = .002). Major adverse cardiac and cerebrovascular events occurred in 824 patients. The incidence of MACCE was higher in the high FAR group than in the low FAR group (16.3% vs 13.0%, P = .001). Additionally, the MACE incidence was 15.3% in the high FAR group and 11.6% in the low FAR group (P < .001). Furthermore, HF incidence was more frequent in the high FAR group than in the low FAR group (3.9% vs 2.5%, P = .003). The multivariate Cox proportional hazards model showed that the FAR was an independent predictor of ACM (adjusted HR = 1.432 [1.134-1.808], P = .003), CM (adjusted HR = 1.579 [1.218-2.047], P = .001), MACCE (adjusted HR = 1.296 [1.125-1.494], P < .001), MACE (adjusted HR = 1.357 [1.170-1.572], P < .001), and HF (adjusted HR = 1.540 [1.135-2.091], P = .006). The data are shown in Tables 2 and 3 and Figure 2.
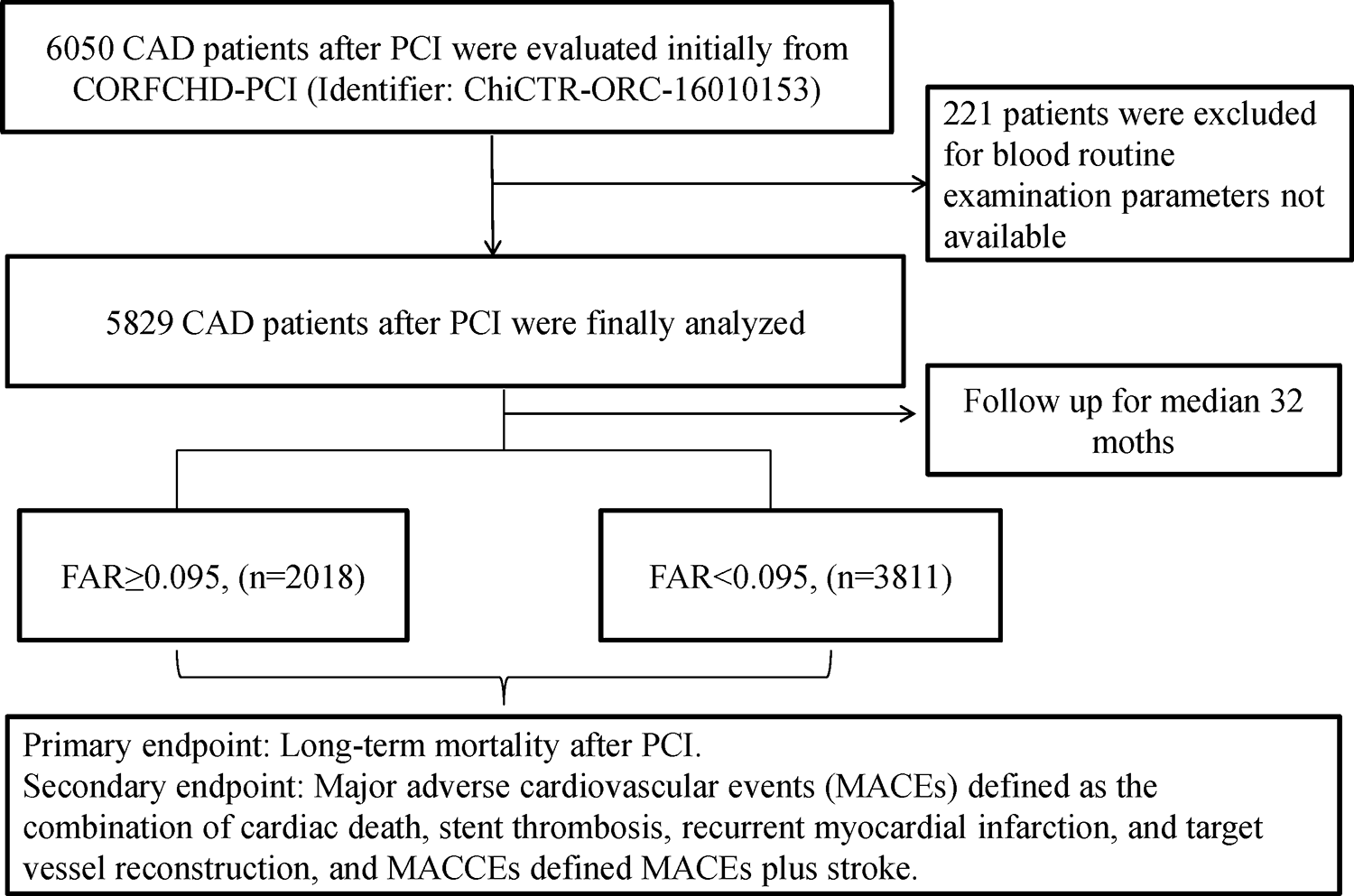
The participant flow chart.

Cumulative Kaplan-Meier estimates of the time to the first occurrence of the primary or secondary end points.
Outcomes Comparison Between Groups.

Abbreviations: ACM, all-cause mortality; CM, cardiac mortality; MACE, major adverse cardiovascular events; MACCE, major adverse cardiovascular and cerebrovascular events; TVR, target vessel reconstruction.
Hazard Ratio for Outcomes Before and After Adjustments.

Abbreviations: ACM, all-cause mortality; CM, cardiac mortality; HR, hazard ratio; MACE, major adverse cardiovascular events; MACCE, major adverse cardiovascular and cerebrovascular events; TVR, target vessel reconstruction.
Discussion
In the present study, we demonstrated that the FAR was significantly associated with long-term outcomes in patients with CAD who underwent PCI. This is the first study of a large sample size population with a long-term follow-up time to report the association of the FAR with outcomes of patients with CAD who underwent PCI.
Previous studies suggested that both higher plasma fibrinogen levels and lower serum albumin levels were correlated with adverse cardiovascular outcomes. 4,5,11,12 Albumin, which is mainly synthesized in the liver, is the most abundant protein in serum. Studies have shown that albumin ≤35 g/L at admission is an independent predictor of new-onset heart failure and in-hospital death in patients with acute coronary syndrome. 22 Plasma fibrinogen, an acute-phase reactant, is a particularly appealing molecule to evaluate the development and progression of coronary atherosclerosis. Fibrinogen and its degradation products can interact with endothelial cells, platelets, monocytes, and lymphocytes to participate in the inflammatory response of atherosclerosis, causing thrombosis, vascular endothelial injury, and hemorheological changes. 23 Therefore, recently, the ratio of fibrinogen to albumin, FAR, has been considered in relation to thrombotic events. Both fibrinogen and albumin are major components of whole-blood viscosity, a risk marker for cardiovascular disease. 24 –27 Coronary artery disease is a complex disease with many risk factors. Older age, type 2 DM, HP, smoking, hyperlipidemia, and inflammation are risk factors for CAD. We believe that the FAR, as a readily available and less expensive marker, has an important role in the evaluation of inflammation and hemorheology and may help clinicians predict the outcomes of CAD after PCI.
As a novel biomarker, the FAR was an independent predictor of patients with CAD as described in several recent publications. 15,16,18 Karahan et al 15 reported that the FAR was significantly related to the SYNTAX score in patients with CAD. Xiao et al 16 analyzed 475 patients with ST-segment elevation myocardial infarction (STEMI) patients undergoing PCI and found that the FAR is an independent predictor of patients with STEMI undergoing PCI. Zhao et al 18 also reported that the FAR was independently and positively associated with 30-day ACM in patients with STEMI. Similarly, in our study, we found that the FAR was an independent predictor of long-term outcomes (including ACM, CM, MACCE, and MACE) in patients with CAD who underwent PCI.
The 2 mechanisms associated with ischemic events and the FAR are as follows: (1) The inflammatory response might be the main mechanism. A previous study suggested that fibrinogen is an acute-phase reactant protein with positive pro-inflammatory effects, 28 and fibrinogen upregulates the synthesis of pro-inflammatory cytokines such as interleukin-1 and tumor necrosis factor. 29,30 (2) In addition, serum albumin is also involved in acute inflammatory reactions but acts as a negative inflammatory protein that has been shown to have protective anti-inflammatory properties. 31 Therefore, a high FAR results in an increased risk of ischemic events.
In our study, we also found that TG and LDL-C levels were significantly higher in the low FAR group than in the high FAR group. As described earlier, a low FAR can result from decreased plasma fibrinogen levels and/or increased albumin levels. Therefore, the reason why TG and LDL-C levels are increased in the low FAR group remains unclear. We also found that male sex, GLU, and HDL-C were significantly different between the high FAR group and the low FAR group. After adjustment for these confounders, the FAR remained independently associated with the adverse outcomes of patients with CAD who underwent PCI.
Nevertheless, several limitations of our study should be stated. On the one hand, the present study is a single-center, retrospective cohort study. Therefore, some variables, such as the parameters of platelet activation, coagulation, and thrombosis, could not be collected at baseline. On the other hand, we only collected the baseline characteristics of the patients. Therefore, the relation between the dynamic changes in the FAR and outcomes could not be analyzed.
In conclusion, this study suggests that the baseline FAR is a simple, inexpensive, and independent predictor of adverse outcomes in patients with CAD who underwent PCI.
Footnotes
Acknowledgments
The authors are grateful to the Department of Cardiology at the First Affiliated Hospital of Xinjiang Medical University for their support and expertise in conducting this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the National Natural Science Foundation of China (U1603381, 81760043), China Postdoctoral Science Foundation (2019M652593), Xinjiang Science and Technology Aid Project (2019E0278), Tianshan Xuesong Project (2018XS17), and Henan Postdoctoral Science Foundation (1902006).