
Abstract
The role of activation of the coagulation and fibrinolysis system in the pathogenesis and prognosis of cardiovascular diseases (CVDs) has drawn wide attention. Recently, the D-dimer to fibrinogen ratio (DFR) is considered as a useful biomarker for the diagnosis and prognosis of ischemic stroke and pulmonary embolism. However, few studies have explored the relationship between DFR and cardiovascular disease. In our study, patients were divided into 2 groups according to DFR value: the lower group (DFR < 0.52, n = 2123) and the higher group (DFR ≥ 0.52, n = 1073). The primary outcome was all-cause mortality (ACM) and cardiac mortality (CM). The average follow-up time was 37.59 ± 22.24 months. We found that there were significant differences between the 2 groups in term of ACM (2.4% vs 6.6%, P < 0.001) and CM (1.5% vs 4.0%, P < 0.001). Kaplan–Meier analyses showed that elevated DFR had higher incidences of ACM (log rank P < 0.001) and CM (log rank P < 0.001). Multivariate Cox regression analyses showed that DFR was an independent predictor of ACM (HR = 1.743, 95%CI: 1.187-2.559 P = 0.005) and CM (HR = 1.695, 95%CI: 1.033-2.781 P = 0.037). This study indicates that DFR is an independent and novel predictor of long-term ACM and CM in post-PCI patients with CAD.
Keywords
Introduction
Coronary artery disease (CAD) is the leading cause of morbidity and mortality worldwide. 1 Over the past few years, percutaneous coronary intervention (PCI) has achieved great success in reducing mortality especially for myocardial infarction. 2 Pedersen et al reported that although patients with CAD treated with primary PCI had a lower risk of cardiac death in the short-term prognosis, the risks of death and in-stent restenosis was still increasing over time. 3
In recent years, the role of activation of the coagulation and fibrinolysis system in the pathogenesis and prognosis of CADs has drawn wide attention. 4 As a biomarker of fibrin formation and degradation, elevated D-dimer levels are associated with higher risk of total mortality in patients with different diseases. 5,6 The LIPID Study has demonstrated that high D-dimer levels are able to predict long-term mortality, cardiovascular events and cancer in stable CAD patients, independently of other risk factors. 7 However, the concentrations of D-dimer can be influenced by other clinical conditions associated with additional fibrin formation, including old age, malignancies, infections and postoperative status. 8,9
Fibrinogen, the precursor of fibrin, is a key coagulation factor, which is associated with the thrombotic process and the inflammatory process, and plays a pivotal role in the development of atherosclerosis. 10,11 Previous studies have shown that fibrinogen was not only independently associated with the development of CAD, hypertension and stroke, but also an independent predictor of long-term prognosis in patients after PCI. 12 –14 More recently, it has been reported that the D-dimer to fibrinogen ratio (DFR) is a novel predictor for the outcomes of pulmonary thromboembolism (PTE), ischemic stroke and gastrointestinal stromal tumors (GISTs). 15 –17
However, the relationship between the DFR and prognosis in CAD patients after PCI has not been investigated. In this study, we enrolled 3,196 patients with CAD who underwent PCI and investigated the relationship between the DFR and clinical outcomes.
Materials and Methods
In this study, we enrolled 3,196 CAD patients who underwent PCI at the First Affiliated Hospital of Zhengzhou University. All of the patients were from the Clinical Outcomes and Risk Factors of Patients with Coronary Heart Disease after PCI (CORFCHD-ZZ) study. The study has been registered with the Chinese Clinical Trial Registry (ChiCTR1800019699). The CORFCHD-ZZ study was a large, retrospective cohort study, which included 3561 post-PCI patients with CAD admitted to the First Affiliated Hospital of Zhengzhou University from January 2013 to December 2017. And its data was obtained from case records and follow-up. The inclusion criteria were CAD patients including non-ST-segment elevation acute coronary syndrome (ACS), ST-segment elevation ACS and stable angina, who underwent coronary angiography, showing stenosis 70% and receiving at least one stent implantation. We excluded patients who had severe heart failure, rheumatic heart disease, valvular heart disease, congenital heart disease, pulmonary heart disease, pulmonary thrombosis, deep vein thrombosis and serious dysfunction of the liver or kidney. This study complies with the Declaration of Helsinki and the protocol was approved by the ethics committee of the First Affiliated Hospital of Zhengzhou University.
To investigate the correlation between the DFR and prognosis in patients with CAD after PCI, 3561 patients were initially evaluated. 365 patients were subsequently eliminated due to unavailable baseline D-dimer or fibrinogen data. Finally, there were 3196 eligible patients in our study. Figure 1 shows the flow chart of the inclusion and exclusion criteria used in the selection of participants.

The flow chart of participant’s inclusion.
Clinical and Demographic Characteristics Collection
The demographic, cardiovascular risk factors and laboratory data were collected and recorded for all study populations. Demographic data included gender and age. Cardiovascular risk factors included smoking status, history of hypertension, previous diagnosis of diabetes, alcohol consumption, and family history of CAD. Hypertension was defined as patients who had a clear history of hypertension and were actively taking anti-hypertensive drugs, or patients whose blood pressure were more than 140/90 mmHg took at least 3 resting measurements during at least 2 separate health care visits, as recommended by the American Heart Association. 18 Diabetes was defined as having a clear history of diabetes and using hypoglycemic drugs, or HbA1c ≥ 6.5%, or Fasting blood glucose (FPG) ≥ 126 mg/dl (7.0 mmol/l), or 2-hour plasma glucose ≥200 mg/dl (11.1 mmol/l) after an OGTT, or random plasma glucose ≥ 200 mg/dl (11.1 mmol/l). 19 Height and weight were obtained while the patient wore light clothes without shoes. Persons who reported regular tobacco use in the previous half a year were considered as current smokers. Persons who were ingesting alcohol in the last half a year were considered to be alcohol users. 20
D-dimer and Fibrinogen Detection
Fasting blood was collected before coronary angiography and fasting for at least 12 hours. Vacutainer tubes used sodium heparin as anticoagulant. D-dimer and fibrinogen were measured by a standard method in accordance to the central laboratory standard of the First Affiliated Hospital of Zhengzhou University. The normal concentration of serum D-dimer is 0-0.3mg/L and fibrinogen is 2-4 g/L. Both the D-dimer and fibrinogen were detected in the same laboratory.
Primary Endpoints
The primary endpoint was the long-term mortality, including all-cause mortality (ACM) and cardiac mortality (CM), during 7-year follow-up. The secondary endpoint was major adverse cardiac events (MACEs), which was defined as the combination of cardiac death, recurrent myocardial infarction and target vessel reconstruction, and major adverse cardiac and cerebrovascular events (MACCEs) defined as MACEs plus stroke. Deaths were assumed to result from cardiac causes unless the fatal causes were definitively noncardiac. 21 The outcomes was adjudicated by Clinical Event Committee, which was made blindly.
Follow-Up
In our center, all of the patients who underwent PCI will receive regular follow-up after discharge. All of them were included from January 2013 to December 2017, and the date of the last follow-up was June 2019. The longest follow-up time was 78 months and the shortest was 18 months, along with mean follow-up time as (37.59 ± 22.24) months. The investigators followed the patients, either by office visits or by telephone contacts when necessary. The compliance of the drugs and adverse events was assessed at every visit for clinical follow-up.
Statistical Analyses
All analyses were performed using the SPSS 22.0 for Windows statistical software (SPSS Inc, Chicago, Illinois, United States). Continuous data are presented as the mean ± standard deviation. Categorical data are presented as frequencies and percentages. Patients were divided into 2 groups according to the DFR level (< 0.52, and ≥ 0.52). The differences between normally distributed numeric variables were analyzed by a t-test, while non-normally distributed variables were analyzed by the Mann–Whitney U-test or Kruskal–Wallis variance analysis as appropriate. Chi-square test was employed for the comparison of categorical variables. Kaplan–Meier analysis was used for cumulative incidence rates of long-term outcomes and the log-rank test was used to compare between groups. Multivariable analysis was carried out to assess the predictive value of the DFR for outcomes during and after a 7-year follow-up. Hazard ratios (HRs) and 95% confidence intervals (CIs) were calculated. P-value of < 0.05 was considered significant.
Result
Baseline Data
In our study, patients were divided into 2 groups according to the DFR value: the lower group (DFR < 0.52, n = 2123) and the higher group (DFR ≥ 0.52, n = 1073).
As shown in Table 1. There were significantdifferences between the 2 groups in age, gender, smoking, alcohol drinking, blood urea nitrogen (BUN), creatinine (Cr) and triglyceride(TG) (all P values < 0.05).
Baseline Characteristics of Patients and Clinical Outcomes.

Abbreviations: DFR, D-dimer to fibrinogen ratio; BUN, Blood urea nitrogen; Cr, Creatinine; UA, Uric acid; TG, Triglyceride; TC, Total cholesterol; HDL-C, High-density lipoprotein cholesterol; LDL-C, Low-density lipoprotein cholesterol; MACEs, Major adverse cardiovascular events; MACCEs, Major adverse cardiovascular and cerebrovascular events.
We did not find significant differences in respects of hypertension, diabetes, heart rate, uric acid (UA), total cholesterol (TC), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C) (all P values ≥ 0.05).
Clinical Outcomes
As shown in Table 1, for the primary endpoint, we found that the incidence of ACM in the lower DFR group was 51 (2.4%), while in the higher DFR group was 71 (6.6%), and the difference was significant (P < 0.001); there was also a significant difference in the incidence of CM between the 2 groups (1.5% vs 4.0%, P < 0.001). For the secondary endpoints, the difference was significant in MACCEs (10.8% vs 12.2%, P = 0.010), but there were no significant difference in the incidence of MACEs (11.9% vs 11.1%, P = 0.246).
Significant different variables (P < 0.05) which were shown in univariate models for each of the predictor variables entered into multivariate Cox regression analysis as shown in Tables 2 and 3. The results of multivariate Cox regression analysis showed that compared with the lower group, patients in the higher group had an increased risk of ACM (HR = 1.743, 95%CI: 1.187-2.559, P = 0.005) and CM (HR = 1.695, 95%CI: 1.033-2.781, P = 0.037) after adjusting the influence of age, sex, hypertension, diabetes and other confounding factors of age, gender, smoking, alcohol drinking, BUN, Cr and TG. Furthermore, as shown in Figures 2 and 3, the Kaplan-Meier analyses showed that elevated DFR was closely related to long-term ACM (log-rank, P < 0.001) and CM (log-rank, P < 0.001).
Cox Regression Analysis Results for Long-Term All-Cause Mortality.

Abbreviations: BUN, Blood urea nitrogen; TG, Triglyceride; DFR, D-dimer to fibrinogen ratio.
Cox Regression Analysis Results for Long-Term Cardiac Mortality.
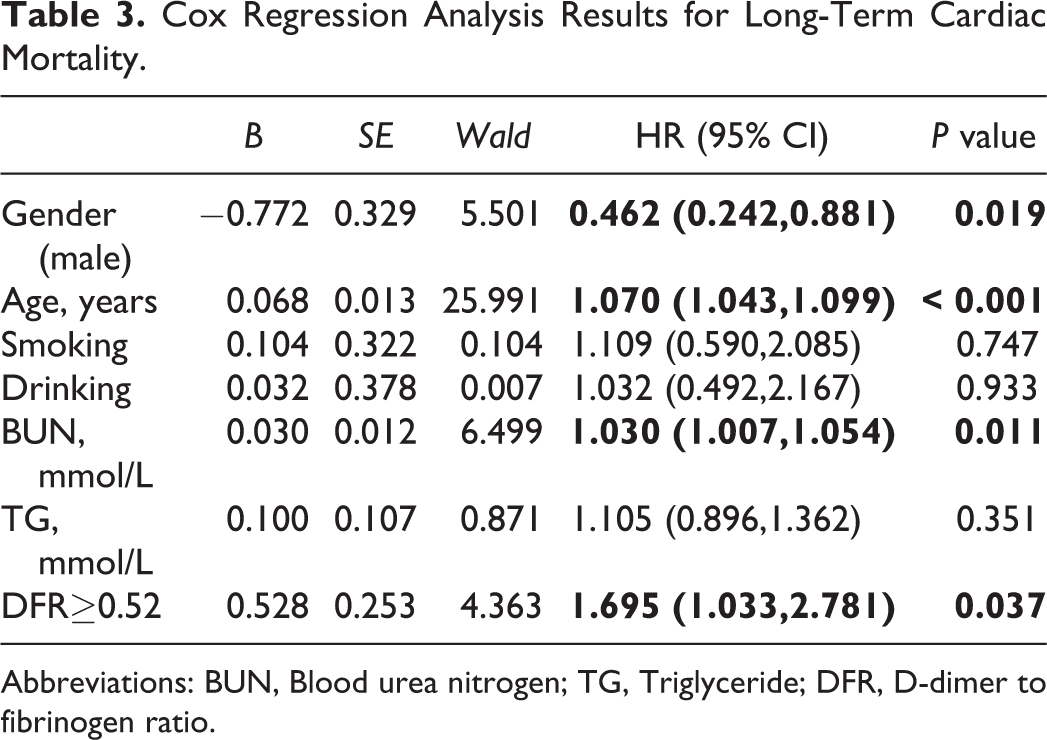
Abbreviations: BUN, Blood urea nitrogen; TG, Triglyceride; DFR, D-dimer to fibrinogen ratio.

Cumulative Kaplan–Meier estimates of the time to all-cause mortality.

Cumulative Kaplan–Meier estimates of the time to cardiac mortality.
Discussion
The results of this study showed that elevated DFR is an independent predictor of long-term ACM and CM in post-PCI patients with CAD. as far as we know, this is the first study to investigate the relationship between the DFR and prognosis in CAD patients.
D-dimer plays an important role in coagulation and fibrinolysis system, which is a degradation product of cross-linked fibrin and commonly considered as a coagulation marker in clinical practice. Increased D-dimer levels is a sensitive marker for thrombosis. 22,23 In recent years, several studies have shown that D-dimer levels are associated with the risk of death in patients with coronary artery diseases. 24,25 In addition, one study showed that elevated D-dimer is a strong independent risk factor for all-cause and cardiac mortality in patients after PCI. 26 Although previous studies have confirmed the relationship between D-dimer and CADs, the mechanism remains unclear.
Fibrinogen is a blood coagulation parameter and acute phase protein that is synthesized by the liver. Fibrinogen is a marker of thrombosis and inflammation, which can cause the migration and proliferation of smooth muscle cells, platelet aggregation, and vascular endothelial dysfunction. Some previous studies showed that fibrinogen is closely related to the prognosis of coronary artery diseases. 27 –29 Liu et al showed that fibrinogen could be used as an independent predictor of MACEs in stable CAD patients. 30 Song et al found that the plasma FIB level is a useful biomarker to predict death or non-fatal reinfarction within 1 year in patients with NSTE-ACS undergoing PCI. 31 Mahmud et al 32 found that elevated serum fibrinogen was associated with major adverse cardiovascular events at 12 months following percutaneous coronary intervention. Since the D-dimer and fibrinogen are both associated with the major cardiovascular events after PCI, we can pay more attention to the DFR. In the coagulation system, FIB can be transformed into fibrin by thrombin, the activation of fibrinolysis results in elevated fibrin degradation products such as D-dimer. Several studies have been reported that the D-dimer to fibrinogen ratio (DFR) is a useful biomarker. Kucher et al showed that the D-dimer to fibrinogen ratio could be a specific predictor for PTE in emergency patients with no other medical condition. 33 Similarly, Hajsadeghi et al demonstrated that the D-dimer to fibrinogen ratio (DFR) appears to be almost as useful as D-dimer in diagnosing PTE in the ICU setting. 34 In addition, a previous study reported that the D-dimer to fibrinogen ratio (DFR) can be used as effective hematological biomarkers for monitoring the prognosis of GIST patients. 16 Alvarez-Perez et al found that the increase of D-dimer to fibrinogen ratio (DFR) was associated with cardioembolic stroke patients. 17 Moreover, Wuillemin et al showed that the D-dimer to fibrinogen ratio (DFR) was significantly higher in patients who had deep vein thrombosis than those who did not have. 35
Limitations
There are also some limitations in our study. Firstly, we only collected the baseline D-dimer and fibrinogen data, the dynamic changes of the DFR did not be analyzed. Secondly, this study included patients with CAD who underwent PCI, but future research needs to explore the role of DFR in the prognosis of different types of cardiovascular diseases, such as unstable angina and stable angina. Thirdly, our study is a single retrospective cohort design in Chinese patients with CAD who underwent PCI. Considering racial differences, this result needs to be further confirmed in a multi-ethnic, multi-center, prospective study confirm these results. Considering the limitations of retrospective research, there is inevitable information bias and selection bias. Therefore, the interpretation of the data should be careful. Last but not least, in this study, we divided patients into 2 groups according to FDR values. Baseline characteristics showed that there were large differences in multiple factors between the 2 groups. Although we use the COX regression method to explore the role of FDR in evaluating the prognosis of patients, there may still be the influence of confounding factors.
Conclusions
In conclusion, our study demonstrates that the D-dimer to fibrinogen ratio (DFR) was an inexpensive, reliable and easily detected effective predictor of long-term ACM and CM in post-PCI patients with CAD.
Footnotes
Authors’ Note
Yan Bai and Ying-Ying Zheng contributed equally. YB and YYZ made substantial contributions to study conception and design, performed the statistical analyses, and drafted the manuscript. JNT, XMY, QQG, JCZ, MDC, FHS, KW, ZLZ, ZYL, LZJ, LF, XTY, XYD, RJZ participated in the collecting and analyzing of the data, written and reviewed the manuscript. JYZ conceived the study, participated in the design, drafted and critical revision of the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declare that they have no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Nature Science Foundation of China (81870328, 81760043 and 81800267) and China Postdoctoral Foundation (2019 M 652593).