
Abstract
Background
Previous evidences have been proved that age, N-terminal pro-B-type natriuretic peptide (NT-proBNP), and ejection fraction are tightly associated with the long-term outcomes in patients suffered from coronary artery disease (CAD). Therefore, the present study aimed to assess the prognosis value of age, NT-proBNP, and ejection fraction (ABEF) score in CAD patients who underwent percutaneous coronary intervention (PCI).
Methods
Observational cohort methodology was used in this study which enrolled totally 3561 patients. And the patients were followed up regularly for 37.59 ± 22.24 months. Patients were classed into three groups based on the tertiles of ABEF sore: first tertile (<5.06, n = 831), second tertile (5.06-6.25, n = 839), and third tertile (≥ 6.25, n = 834). The ABEF score was calculated as follows: age (years)/ejection fraction (%) + NT-proBNP (NT-proBNP<177pg/mL was 1, 177≤NT-proBNP≥524pg/mL was 2 and NT-proBNP > 524pg/mL is 3). The association between ABEF score and adverse prognosis, including all-cause death (ACD), cardiac death (CD), major adverse cardiovascular events (MACEs) and major adverse cardiac and cerebrovascular events (MACCEs), in patients who underwent PCI was analyzed.
Results
According to the risk category of ABEF score, the incidences of ACD (P < .001), CD (P < .001) and MACCEs (P = .021) among the three groups showed significant differences. Multivariate Cox regression analysis suggested that the respective risks of ACD and CD were increased 3.013 folds (hazard risk [HR] = 4.013 [95% confidence interval [CI]: 1.922-8.378], P < .001) and 4.922 folds ([HR] = 5.922 [95% [CI]: 2.253-15.566], P < .001) in the third tertile compared with those in the first tertile. Kaplan-Meier survival analyses showed that the cumulative risks of ACD,CD and MACCEs in patients with the high ABEF score tended to increase.
Conclusion
The present study indicated ABEF score was a novel biomarker suitable for predicting adverse prognosis in patients after PCI, which may be used for early recognition and risk stratification.
Introduction
Ischemic heart disease, particularly the CAD, remains the leading cause of death in either developed countries or developing countries. 1 According to the data on the epidemiology and prevention of CVD in China, about 2.4 million deaths from CAD in 2016, accounting for 25% of all deaths. 2 Although there are significant breakthroughs in prevention, diagnosis and treatment of CAD, 3 particularly the usage of percutaneous coronary intervention (PCI), as well as stains and antithrombotic drugs, the prognosis of patients with CAD is still unsatisfactory, and early risk stratification of these patients has aroused widespread concern among physicians. Overwhelming evidences suggest that clinical characteristic, cardiac biomarkers and left ventricular ejection fraction (LVEF) have a tight relation with adverse clinical outcomes of CAD patients,4‐6 therefore these parameters have been selective to establish different risk stratification models.5,7,8
Recent studies show that advancing age is a crucial risk factor for the development and endpoints of CAD, 9 and the mechanisms of how ageing influences the pathology of atherosclerosis may include: First, ageing can influence the development of immune cells including macrophages 3 and dendritic cells, 10 which could promote atherosclerosis by producing cytokines (like IL-6); Second, ageing results in dysfunctions in vascular mitochondrial and impaired mitophagy which contributes to the accumulation of reactive oxygen species. 11 The neurohormone pro-brain natriuretic peptide is synthesized and released when cardiac myocytes are exposed to hemodynamic stress, 12 and it is further cleaved into NT-proBNP by proteolytic enzymes. NT-proBNP has been shown to be an effective and sensitive biomarker in heart failure, 13 and it was also used to predict the severity of the coronary lesions in acute coronary syndromes (ACS) patients. 14 Moreover, recent studies have shown that the elevated NT-proBNP levels is an independent predictive factor of high mortality in patients with ACS.15‐17 Most CAD patients will eventually develop left ventricular insufficiency, and LVEF have been widely performed to predict the outcomes of CAD patients. 18
Older age and cardiac dysfunction were accepted prognostic markers in patients with CAD. Although these parameters of older age, NT-proBNP, and LVEF have gained popular attention, there still remains a gap on relationship between the combined biomarker, age, NT-proBNP, and ejection fraction (ABEF) score, and the outcomes of patients after PCI. Therefore, we will evaluate the value of ABEF sore on predicting the long-term adverse events of patients undergoing PCI.
Methods
Study Design and Population
The present study enrolled 3561 CAD patients undergoing PCI (CORFCHD-ZZ; identifier: ChiCTR1800019699). All the data of CAD patients who had been hospitalized in the First Affiliated Hospital of Zhengzhou University from January 2013 to December 2017 and been diagnosed by coronary angiography (CAG), were collected retrospectively from case records. The inclusion criteria included: (1) patients >18 years old; (2)coronary artery stenosis ≥75% confirmed by CAG; (3) at least one stent was implanted. Exclusion criteria were as follows: (1) severe valvular heart disease (defined as stage C or D of valvular heart disease); (2) malignant tumor; (3) serious dysfunction of the liver (defined as alanine aminotransferase or total bilirubin greater than 3 times the normal upper limit) or kidney (defined as eGFR < 20 mL/min/1.73 m2 or requiring dialysis); (4) severe congenital heart disease; (5) severe infectious disease.
In the study, 3561 CAD patients undergoing PCI were evaluated at first, and 1057 patients were excluded for the age, NT-proBNP or LVEF data none being available or according to the exclusion criteria. Finally, 2504 patients were included, and the flowchart of the inclusion and exclusion criteria of the study are presented as Figure 1.

The flowchart of patients’ enrollment.
Clinical, Demographic and Laboratory Characteristics
After the ethics of this study was passed, we collected the clinical data of all patients by accessing patients’ electronic medical records. The data about clinical and demographic characteristics, such as sex, age, the history of diabetes and hypertension, alcohol abuse and smoking status, were obtained. We also recorded the imaging and laboratory data, including the results of CAG and echocardiography, liver and kidney function, and lipid parameters. The use of drugs, such as β-blockers, clopidogrel, ticagrelor, statins, aspirins, angiotensin-converting enzyme inhibitors (ACEIs), or angiotensin II receptor blockers (ARBs) was noted during the follow-up period. The ABEF score was calculated as follows: age (years)/ejection fraction (%) + NT-proBNP (NT-proBNP < 177pg/mL was 1, 177≤NT-proBNP≥524pg/mL was 2 and NT-proBNP > 524pg/mL is 3).
Definitions
Hypertension was defined as any history of hypertension or blood pressure measuring ≥ 140/90 mm Hg on at least three resting measurements at three different times. 19 Diabetes mellitus was diagnosed when fasting plasma glucose levels were up to 7.1 mmol/L or a 2-h post-load glucose concentration of 11.1 mmol/L on multiple measurements, or any receipt of treatment with glucose-lowering drugs. 20 Smoking was defined as any regular cigarette use 6 months ago, and alcohol use was considered as any intake of alcohol in the past 6 months. 21
Endpoints
The primary endpoint included ACD and CD, defined as death resulting from established heart disease. And the secondary endpoint included MACEs, defined as the combination of cardiac death, recurrent MI, and target vessel reconstruction, and MACCEs that defined as MACEs plus stroke. 22 All the end points have been described carefully in the previous study. 22 All the events were evaluated and determined by the adjudication committee who were trained in advance and blinded to patients
Follow-up
All of the enrolled patients would receive regular clinic visits or telephone interviews. The average follow-up time was 37.59 ± 22.24 months. During this period, all relevant events were carefully assessed and confirmed by trained clinical physicians.
Statistical Analysis
We analyzed all the data by SPSS 23.0 (SPSS Inc, Chicago, Illinois, United States). The ABEF score was calculated as follows: age (years)/ejection fraction (%) + NT-proBNP (NT-proBNP < 177pg/mL was 1, 177≤NT-proBNP≥524pg/mL was 2 and NT-proBNP > 524pg/mL is 3). Patients were classed into three groups based on the tertiles of ABEF sore: first tertile (<5.06, n = 831), second tertile (5.06-6.25, n = 839), and third tertile (≥ 6.25, n = 834). Continuous variables are shown as the mean ± standard deviation (mean ± SD) and compared by one-way ANOVA (for data complying with the normal distribution) or median ± interquartile range (IQR; 25th to 75th centiles) and compared by Mann-Whitney U test or Kruskal-Wallis variance analysis (skewed distribution). Categorical data are here described as frequencies and percentages and compared using the chi-square (χ2) test. The cumulative incidence rates of adverse outcomes are shown using Kaplan–Meier curves and were compared using the log-rank test. Variables that were significantly different (P < .05) in univariate Cox regression analysis were further entered into multivariate Cox regression analyses which were used to evaluate independent parameters for prognosis. HRs and 95% CIs were computed. The P < .05 was considered to be a significant difference.
Results
Baseline Characteristics
A total of 2504 patients who had undergone PCI were enrolled finally in the study, and categorized into three groups based on the tertiles of ABEF sore: first tertile (<5.06, n = 831), second tertile (5.06-6.25, n = 839), and third tertile (≥ 6.25, n = 834). The mean follow-up time was 37.59 ± 22.24 months. As presented in Table 1, the average age was 63.36 ± 10.57 years at enrollment, and 68.1% were men. In the total population, significant differences among these three groups were observed for several variables, including age, diabetes, LVEF, systolic blood pressure (SBP), diastolic blood pressure (DSP), creatinine (Cr), glucose, total cholesterol (TC), and use of aspirin and statins (all P-values < .05). However, the other variables, such as gender, hypertension, smoking, alcohol drinking, family history, blood urea nitrogen (BUN), triglyceride (TG), uric acid (UA), total cholesterol (TC), high-density lipoprotein (HDL) and low-density lipoprotein (LDL) were not significantly different among these groups (P ≥ 0.05).
Baseline Characteristics.
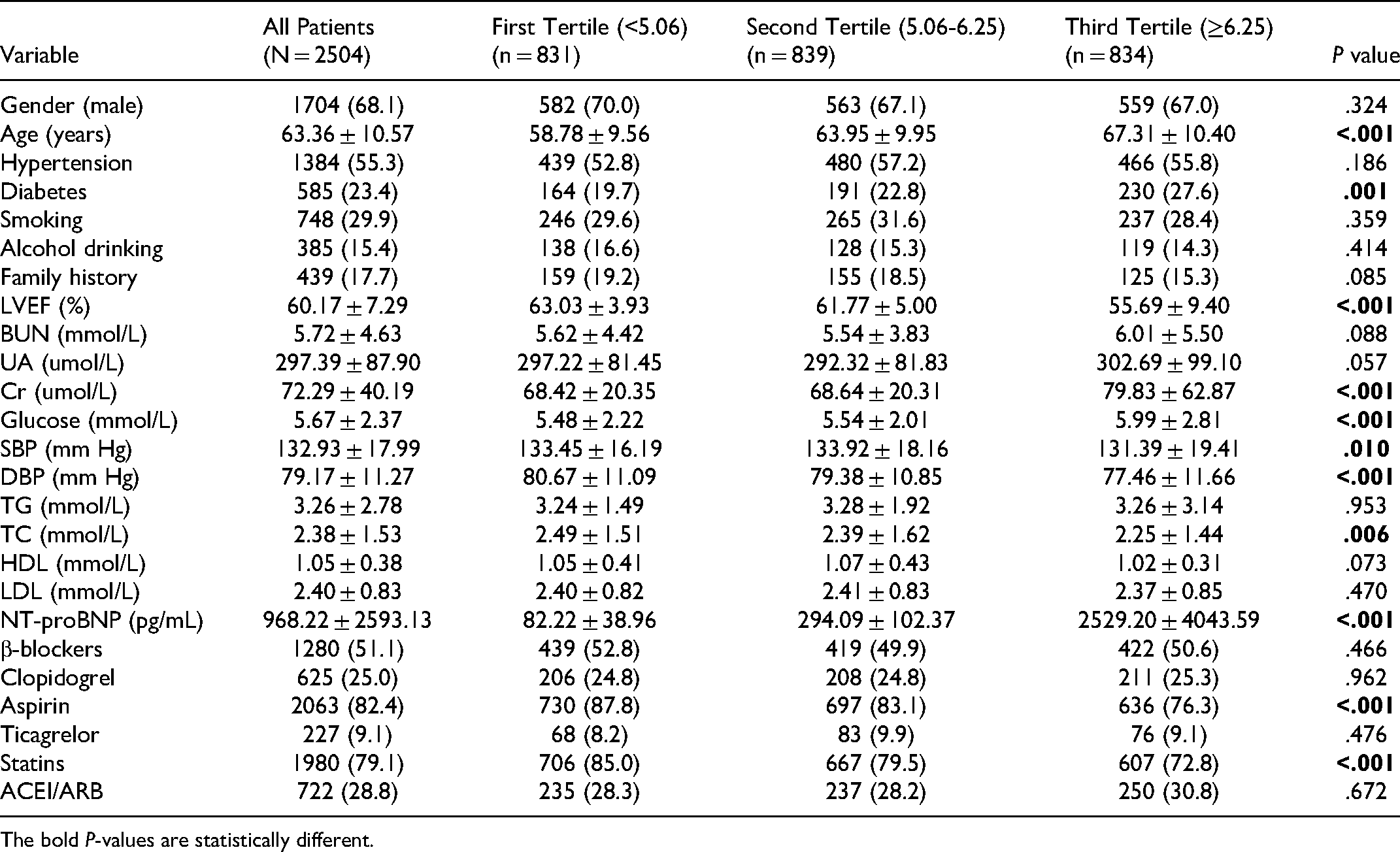
The bold P-values are statistically different.
Clinical Outcomes
As presented in Table 2, 91 cases of ACD were recorded during the duration of follow-up. In total, the morbidity rate of ACD in the first tertile was 9 (1.1%), in the second tertile was 22 (2.6%), and in the third tertile was 60 (7.2%), which was significantly different (P < .001). CD occurred in 59 patients: 5 (0.6%) in the first tertile, 11 (1.3%) in the second tertile, and 43 (5.2%) in the third tertile. The incidence of CD differed significantly among these three groups (P < .001). And 381 patients suffered MACCEs: 105 (12.6%) in the first tertile, 130 (15.5%) in the second tertile, and 146 (17.5%) in the third tertile, which was significantly different (P = .021). While the incidence of MACEs showed no significant differences (P = .186).
Clinical Outcomes Among Three Groups.
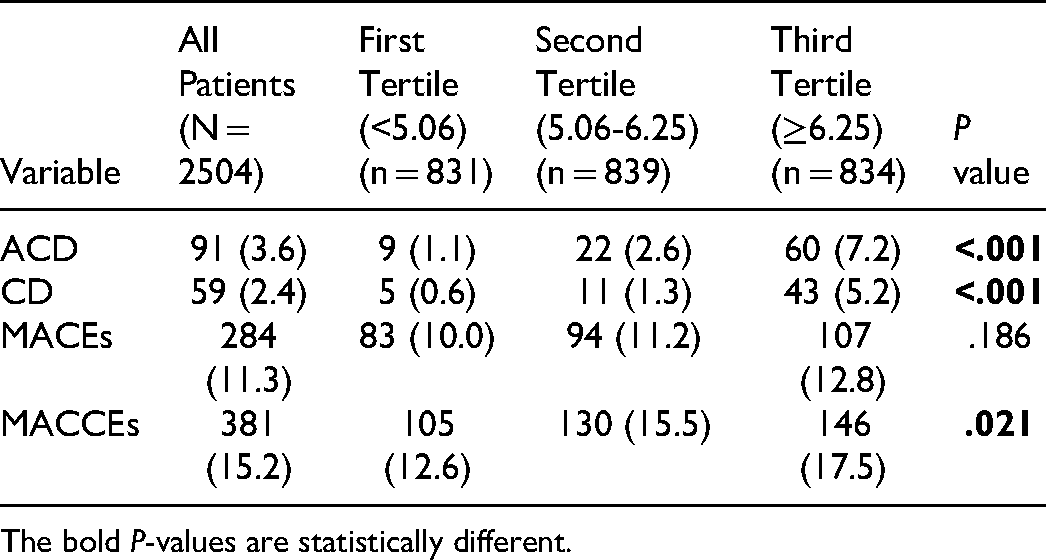
The bold P-values are statistically different.
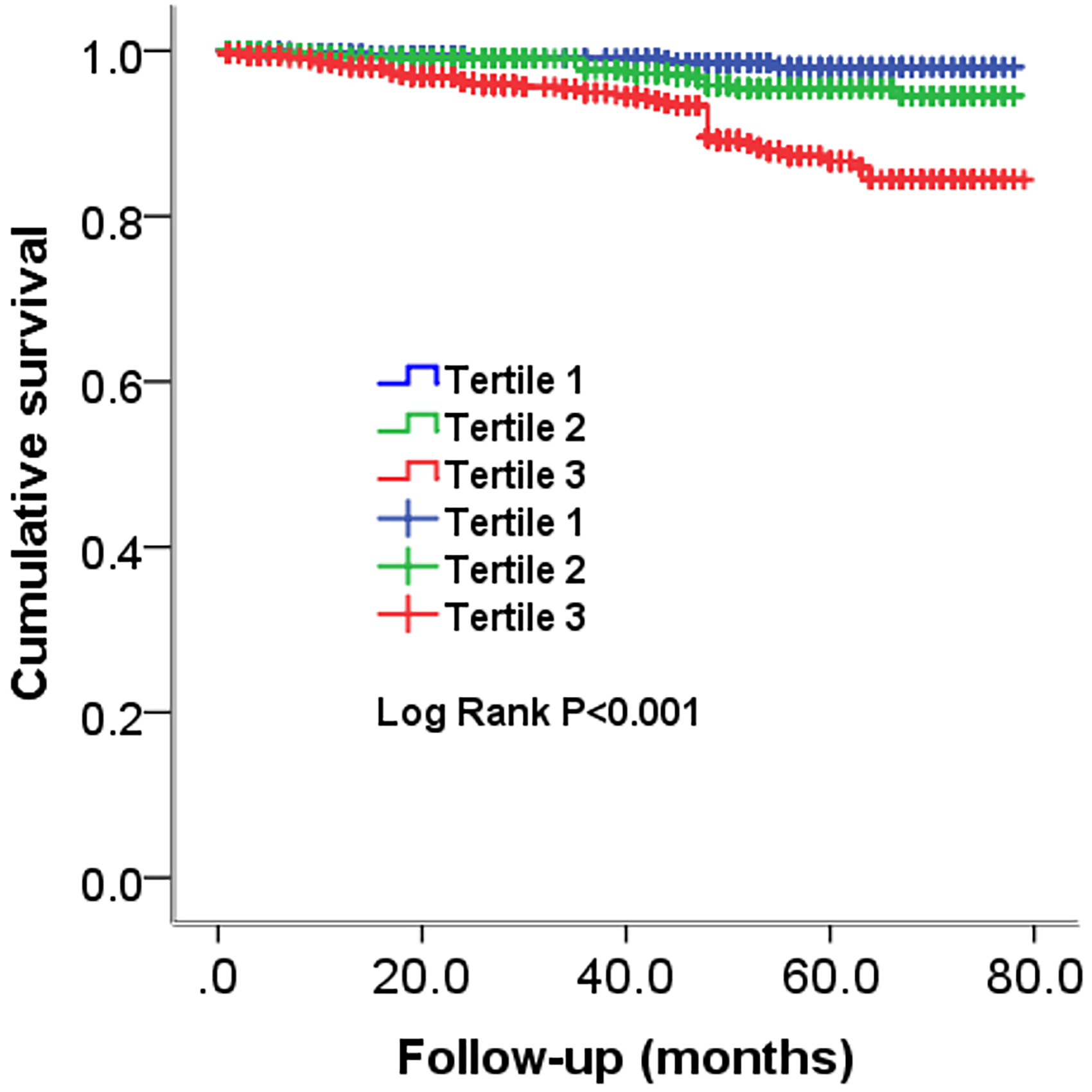
Next, as presented in Figure 2 and 3, Kaplan-Meier curves for ABEF score classified by tertiles and ACD, CD and MACCEs were performed. Patients in the third tertile with ABEF score ≥ 6.25 had a higher risk of ACD, CD MACCEs (Log rank P < .001, P < .001 and P = .027, respectively) compared with patients in the first tertile, as the reference, with ABEF score <5.06 (Figures 4 and 5).
Cumulative Kaplan-Meier estimates of the time to the first adjudicated occurrence of ACD.

Cumulative Kaplan-Meier estimates of the time to the first adjudicated occurrence of CD.

Cumulative Kaplan-Meier estimates of the time to the first adjudicated occurrence of MACEs.

Cumulative Kaplan-Meier estimates of the time to the first adjudicated occurrence of MACCEs.
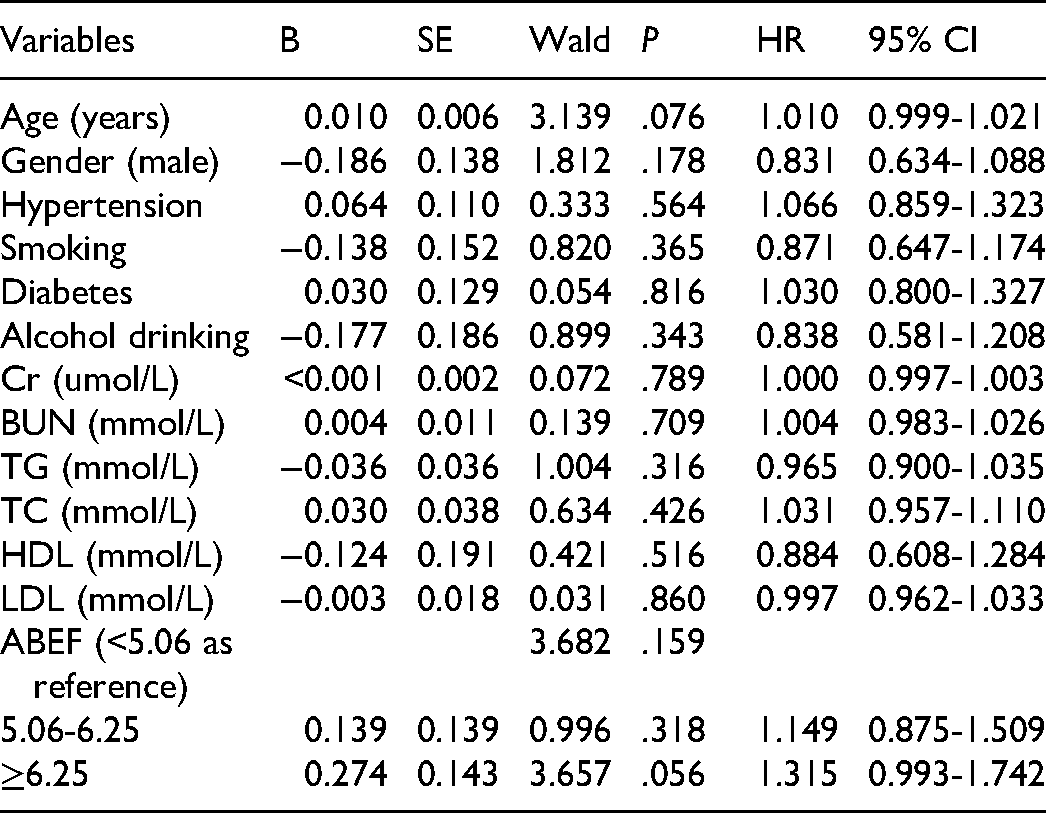
Univariate Cox regression analysis for each of all the related variables were conducted. And variables that showed a significant difference (P < .05) were further entered into multivariate Cox regression analysis, which was performed to evaluate the correlation between ABEF score and adverse outcomes after adjusting for family history, SBP, DSP, LVEF, UA and glucose. According to the results of multivariate Cox regression analyses, the respective risks of ACD and CD were increased 3.013 folds (hazard risk [HR] = 4.013 [95% confidence interval [CI]: 1.922-8.378], P < .001) and 4.922 folds ([HR] = 5.922 [95% [CI]: 2.253-15.566], P < .001) in the third tertile compared with those in the first tertile. (Table 3 and 4). However, no significant differences were observed in multivariate Cox regression analysis results for MACEs and MACCEs Therefore, the higher ABEF score had an independently predictive value for poor prognosis in CAD patients after PCI.
Cox Regression Analysis Results for ACD.

Cox Regression Analysis Results for CD.

Discussion
In the study, we investigated the ability of ABEF score in predicting the long-term adverse prognosis in CAD patients undergoing PCI. To our knowledge, this is the first study that suggested the strong relationship between ABEF score and long-term adverse outcomes in CAD patients treated with PCI. In our study, comparing the ABEF score tertiles, only the patients in the highest tertile (ABEF score ≥ 6.25) were at the increased risk of long-term mortality and MACCEs. To reduce influence of the confounding factors, we adjusted some variables including age, family history, SBP, DSP, LVEF, UA and glucose, the significant differences still remained. The ACD, and CD in the third tertile have 3.013 folds and 4.922 folds increased risks as compared with those in the first tertile (Tables 5 and 6).
Cox Regression Analysis Results for MACEs.

Cox Regression Analysis Results for MACCEs.
The problem of aging is becoming more and more serious in the world, resulting in a continuous rise in mortality of population. With the social and economic development, the process of urbanization and the acceleration of population aging, profound changes have taken place in the life style of Chinese residents. Lifestyle risk factors such as an irrational diet, lack of physical activity and sleep, and alcohol abuse are widely prevalent, and the absolute number of people suffering from hypertension, dyslipidemia, diabetes and obesity in China is still on the rise, which will further increase the morbidity and mortality of cardiovascular disease in our country. In addition, according to the World Health Organization, the number of deaths from CVD worldwide will increase from 18.1 million in 2010 to 24.2 million in 2030. 23 Considering the significant death, severe disability and poor prognosis associated with CAD, it is particularly important to carry out risk stratification and personalized management in the early stage of patients with CAD.
There were various of novel markers, such as microRNAs24‐26 and long chain non-coding RNAs, 27 were used to detect and evaluate the early injuries of cardiomyocytes, which does facilitate the progress of the early identification in patients with CAD to some extent, but there are major difficulties in popular use of clinical practice due to complicated and expensive procedures. Therefore, predictive value of hematological indicators such as high-sensitivity C-reactive protein, 28 hemoglobin, 29 LDL/HDL 30 have gained attentions increasingly. NT-proBNP and BNP, known as the biomarker of heart failure, have been used to evaluate cardiac strain and function, but rarely is considered in predict the adverse outcomes of CAD patients in clinical practice, 31 although many studies suggested that increased NT-proBNP value is associated with high mortality in patients with ACS.15‐17 Age and cardiac function have been demonstrated that they have a tightly relation in the poor prognosis of CAD patients.9,18 So, the ABEF score was reasonable to predict long-term poor prognosis in patients after PCI in the present study.
The CAD patients with higher ABEF score showed higher adverse cardiovascular events in the study, and the reasons may be explained as follows: (1) Ageing affects the occurrence and development of atherosclerosis. Briefly, ageing has a relation with remodeling of the arterial wall, by promoting collagen deposition, fibrosis and functionally stiffer vessels,32‐34 and triggers inflammation response by influence immune cells3,10 and results in dysfunctions in vascular mitochondrial and impaired mitophagy. 11 (2) The increased level NT-proBNP and the decreased LVEF indicate that the cardiac function is impaired. Previous study suggested that a larger ischemic burden, and hence a greater volume of myocardium affected, results in a higher concentration of NT-proBNP. 35 And NT-proBNP showed a satisfactory value in predicting the adverse events in CAD patients.36‐38 Moreover, the end stage of CAD often progresses to varying degrees of heart failure, charactered as decreased LVEF.
Although the ABEF score exhibited an excellent value and may be a promising predictive factor of long-term poor prognosis in CAD patients undergoing PCI, there are still some limitations that need to address in the study: (1) The follow-up time is not long enough and the enrolled patients is small, which may influence the reliability of the results; (2) The study failed to monitor dynamic changes in these parameters (NT-proBNP and LVEF), which is unable to evaluate the effect of the variation of ABEF score on the prognosis of CAD patients; (3) These enrolled patients were from single center, which may make our results unrepresentative. Therefore, the results of this study need to be further confirmed by more large randomized controlled trials.
Conclusion
In conclusion, the study suggested ABEF score is a novel, sensitive, reliable and effective predictor of adverse events in patients who underwent PCI.
Footnotes
Abbreviations
Authors’ Contributions
All of the authors were actively involved in the study. JY Zhang conceived the study and participated in the design. L Fan, ZL Zhang, YY Zheng and JN Tang participated in the design, XT Yue, QQ Guo, JC Zhang, MD Cheng, FH Song, ZY Liu, K Wang, LZ J, Y Bai, XY Dai and RJ Zheng collected the data, YY Zheng performed statistical analyses. L Fan and ZL Zhang drafted the manuscript. JY Zhang critically reviewed the manuscript. All authors read and approved the final manuscript.
Consent for Publication
All authors have viewed the manuscript and written informed consent for publication was obtained from all participants.
Data Availability
The data will not be shared, because the identified participants information is included in the data.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
The present study complies with the Declaration of Helsinki and was approved by the ethics committee of the First Affiliated Hospital of Zhengzhou University.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Natural Science Foundation of Henan Province, National Natural Science Foundation of China, CORFCHDZ- Z, Henan Medical Science and Technique Foundation, (grant number 212300410072, 82000238, ChiCTR1800019699, LHGJ20190119).