
Abstract
The X Kell blood group complex subunit-related family member 6 (XKR6) gene single-nucleotide polymorphisms (SNPs) have been associated with serum lipid profiles and the risk of coronary heart disease (CHD) and ischemic stroke (IS) in several previous studies, but the association between the XKR6 rs7014968 SNP and serum lipid levels and the risk of CHD and IS has not been detected previously. This study aims to explore the association between the XKR6 rs7014968 SNP and serum lipid traits and the susceptibility to CHD and IS in the Guangxi Han Chinese population. Snapshot technology was used to determine the genotypes of the XKR6 rs7014968 SNP in 624 controls, 588 patients with CHD, and 544 patients with IS. The XKR6 rs7014968C allele carriers in the control group had higher serum total cholesterol (TC) levels than the C allele noncarriers (P = .025). The XKR6 rs7014968C allele carriers also had an increased risk of CHD and IS (P < .05-.01). Stratified analysis showed that the patients with the rs7014968C allele in the female, age >60 years, body mass index (BMI) >24 kg/m2, and hypertension subgroups had a higher risk of CHD than those in the subgroup counterparts. The patients with the rs7014968C allele in the male, BMI > 24 kg/m2, smoker, and hypertension subgroups also had a higher risk of IS than those in the subgroup counterparts. These results suggest that the XKR6 rs7014968 SNP is likely to increase the risk of CHD and IS by increasing serum TC levels in our study populations.
Keywords
Introduction
Coronary heart disease (CHD) and ischemic stroke (IS) remain the leading causes of disability, mortality, morbidity, functional deterioration, and health-care expenditure worldwide. 1 –3 More than 2.5 and 1 million people in China are affected by stroke and heart attack, respectively, leading to more than 2 million deaths each year. 4 The pathological basis of both diseases is atherosclerosis, which is caused by the accumulation of cholesterol in arterial wall macrophages and the dysregulation of lipid metabolic rate. Unfavorable serum lipid levels, such as increased levels of total cholesterol (TC), triglycerides (TGs), low-density lipoprotein cholesterol (LDL-C), and apolipoprotein B (Apo B) and reduced levels of high-density lipoprotein cholesterol (HDL-C), ApoA1, and the ratio of ApoA1 to ApoB, are well-established risk factors for CHD and IS. 5 –10 In addition, twin and family studies have indicated that heritable factors account for 30% to 60% of the interindividual variation in the risk of CHD and IS. 11 –14
The X Kell blood group complex subunit-related family member 6 (XKR6) gene (also known as XRG6, hCG_1991046, FLJ31557, C8orf5, C8orf7, or C8orf21; GeneID: 286046; HGNC: 27806; locus type: gene with protein product) is located on chromosome 8p23.1. 15 The 8p23.1 deletion syndrome is a rare multisystem disorder with high penetrance and a variable phenotypic spectrum that includes congenital heart disease, intellectual disability, behavioral problems, microcephalia, and sometimes epilepsy. 16,17 Akcakaya et al 17 reported that a patient with epilepsy who was affected by developmental delay, microcephalia, behavioral problems, congenital heart disease, and childhood-onset absence seizures had a 4-Mb de novo microdeletion at 8p23.1. Some of the genes in this region, particularly XKR6, may be involved in the pathogenesis of absence seizures. Barber et al 18 also described another prenatal and 5 postnatal patients with de novo 8p23.1 duplications that were analyzed by oligonucleotide array comparative genomic hybridization and found that the core duplication of 3.68 Mb contains 31 genes and microRNAs, of which only GATA-binding protein 4 (GATA4), TNKS, SOX7, and XKR6 are likely to be dosage-sensitive genes. Recent genome-wide or follow-up studies showed that 2 single-nucleotide polymorphisms (SNPs), XKR6 rs7460469 and XKR6 rs4240671, were significantly associated with systemic lupus erythematosus (SLE) or childhood-onset SLE in European or Korean populations 19 –21 but not in the Chinese population (XKR6 rs4240671 SNP). 22 In a recent study, we showed that the XKR6 rs7819412 A allele was correlated with increased serum TG levels in patients with CHD and TC levels in patients with IS and a high risk of CHD and IS. 23 To the best of our knowledge, however, the association between the XKR6 rs7014968 SNP and serum lipid levels and the susceptibility to CHD and IS has not been explored previously. Therefore, the present study was undertaken to detect the association between the XKR6 rs7014968 SNP and 7 serum lipid traits and the risk of CHD and IS in the Southern Han Chinese population.
Methods
Control Group
A group of 624 healthy participants matched with the patient group for age, sex, and nationality (Han Chinese) were consecutively recruited as controls. There were 447 (71.6%) males and 177 (28.4%) females. The mean age of the controls was 61.95 ± 9.81 years. All of them were healthy adults who underwent a periodical medical checkup at the Physical Examination Center of The First Affiliated Hospital, Guangxi Medical University, during the same period when patients with CHD and IS were recruited. All of these individuals were free of CHD and IS at the time of medical history, clinical, biochemical, and imaging examinations, such as 64-slice computed tomography coronary angiography. The controls had no known medical problems and did not take medications known to affect serum lipid levels, such as β-adrenergic-blocking agents, thiazide diuretics, lipid-lowering agents, hypoglycemic agents, or hormones.
Coronary Heart Disease Group
A total of 588 patients with CHD were recruited from the patients hospitalized at The First Affiliated Hospital, Guangxi Medical University. There were 431 (73.3%) men and 157 (26.7%) women. The average age of the patients with CHD was 62.29 ± 10.56 years. The diagnosis of CHD was based on the findings of clinical manifestation, electrocardiography, cardiac biomarkers, and coronary angiography. Significant coronary stenosis (≥50%) in at least 1 of the 3 main coronary arteries or their major branches (branch diameter ≥2 mm) was defined as CHD by coronary angiography. 23,24 Patients who had congenital heart disease, cardiomyopathy, or valvular disease were excluded.
Ischemic Stroke Group
A total of 544 IS cases were also recruited from hospitalized patients in our First Affiliated Hospital. There were 393 (72.2%) males and 151 (27.8%) females. The average age of the IS cases was 62.83 ± 12.35 years. The diagnosis and classification of IS were ascertained in accordance with the Trial of Org 10172 in Acute Stroke Treatment criteria 25 after strict neurological examination, computed tomography, or magnetic resonance imaging (MRI). Patients with a history of hematologic or brain MRI revealing cerebral hemorrhage; cardioembolic or unspecified stroke; neoplastic or intracranial space-occupying lesion; infection; other types of intracranial lesions; renal, liver, thyroid, or autoimmune diseases; or type 1 diabetes were excluded. The study protocol was approved by the ethics committee of The First Affiliated Hospital, Guangxi Medical University (No. Lunshen 2009-Guike-018; January 7, 2009) and was conducted according to the Declaration of Helsinki. Informed consent was obtained from all subjects before the study.
Biochemical Assays and Genotyping
A 5-mL venous blood sample was collected from each participant after at least 12 hours of fasting. Part of the sample (2 mL) was placed in a glass tube and used to perform biochemical assays. Another part of the sample (3 mL) was collected in tubes containing anticoagulants (4.80 g/L citric acid, 14.70 g/L glucose, 13.20 g/L trisodium citrate) and was utilized to extract DNA. Genotyping of the XKR6 rs7014968 SNP was performed by Snapshot technology in the Center for Human Genetics Research, Shanghai Genesky Bio-Tech Co Ltd, China. 23,26 –38 The sequences of the forward and backward primers used were 5′-TGGAACTAATCGTTGTTGCCAGTC-3′ and 5′-TCCCAGTGAAAAGCAAACCAGAA-3′, respectively. Seven serum lipid traits (TC, TGs, HDL-C, LDL-C, ApoA1, ApoB, and ApoA1/ApoB) were determined as described in our previous reports. 23,26 –38 All determinations were completed with an autoanalyzer (Type 7170A; Hitachi Ltd, Tokyo, Japan) in the Clinical Science Experiment Center of The First Affiliated Hospital, Guangxi Medical University.
Diagnostic Criteria
The normal ranges of serum TC, TG, HDL-C, LDL-C, ApoA1, and ApoB levels and the ApoA1/ApoB ratio in our Clinical Science Experiment Center were 3.10 to 5.17, 0.56 to 1.70, 1.16 to 1.42, and 2.70 to 3.10 mmol/L; 1.20 to 1.60 and 0.80 to 1.05 g/L; and 1.00 to 2.50, respectively. The patients with TC >5.17 mmol/L and/or TGs >1.70 mmol/L were defined as hyperlipidemic. 23,26 –38 Hypertension was diagnosed according to the criteria of the 1999 World Health Organization-International Society of Hypertension Guidelines for the management of hypertension. 23,26 –38 Normal weight, overweight, and obesity were defined as a body mass index (BMI) <24, 24 to 28, and > 28kg/m2, respectively. 23,26 –38
Statistical Analyses
The statistical analyses were performed using SPSS (version 22.0). Continuous variables are presented as the mean ± standard deviation. Serum TG levels are presented as the medians and interquartile ranges because they were not normally distributed. Categorical variables are presented as numbers or percentages. The Hardy-Weinberg equilibrium (HWE) was verified by a standard goodness-of-fit test. The χ2 test was used to calculate the genotype distribution between cases and controls. The differences in the continuous variables between the patients and controls were tested by Student unpaired t test. The association between the XKR6 rs7014968 genotypes and serum lipid traits was tested by covariance analysis. Sex, age, blood pressure, cigarette smoking, BMI, and alcohol consumption were adjusted for the statistical analysis. The difference in serum TG levels was determined by the Wilcoxon-Mann-Whitney test. Unconditional logistic regression analysis was used to detect the odds ratio (OR) and 95% confidence interval (CI). A P value <.05 was considered statistically significant.
Results
Clinical Characteristics and Serum Lipid Levels
As described in Table 1, the mean values of height, weight, BMI, systolic blood pressure, pulse pressure, and TGs; the percentages of patients who smoked cigarettes and consumed alcohol; and the prevalence of hypertension were higher in the patients with CHD or IS than in controls, whereas the levels of TC, HDL-C, and ApoA1 and the ratio of ApoA1 to ApoB were lower in patients with CHD or IS than in controls (P < .05-.001). In addition, the levels of diastolic blood pressure were lower in patients with CHD and higher in patients with IS than in controls (P < .05 and < .001, respectively).
General Characteristics and Serum Lipid Levels of the Patients.a

Abbreviations: Apo, apolipoprotein; CHD, coronary heart disease; HDL-C, high-density lipoprotein cholesterol; IS, ischemic stroke; LDL-C, low-density lipoprotein cholesterol.
a Quantitative variables are presented as the mean ± standard deviation, and the difference was compared by Student unpaired t test. Serum triglyceride levels are presented as the median (interquartile range), and the difference was determined by the Wilcoxon Mann-Whitney test. Qualitative variables are expressed as percentages. A χ2 analysis was used to evaluate the differences.
Genotypic and Allelic Frequencies of the Patients
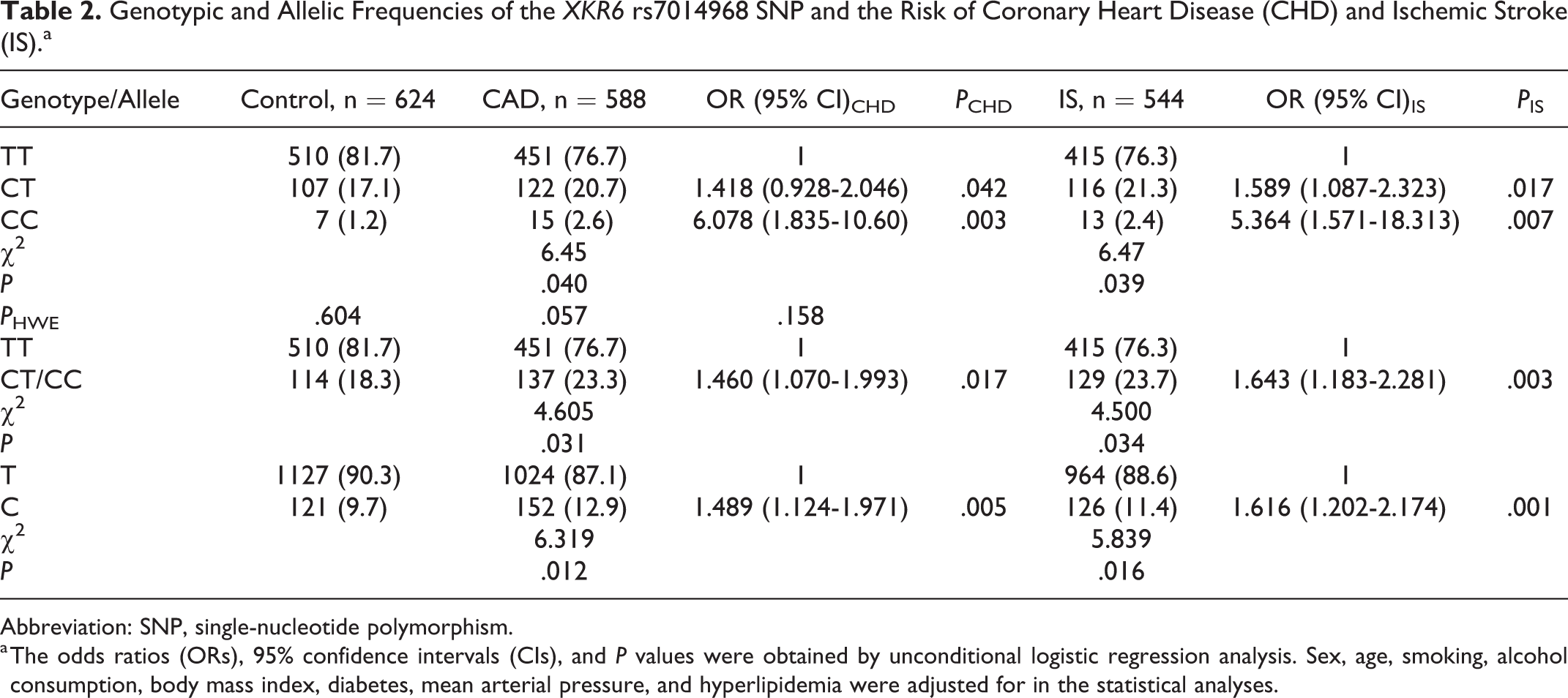
The genotypic and allelic frequencies of the patients are shown in Figure 1. The genotypic distribution in both patients with CHD and IS and controls conformed to the HWE (P HWE > .05; Table 2). The CT and CC genotype and C allele frequencies were higher in the patients with CHD (20.7%, 2.6%, and 12.9%) or IS (21.3%, 2.4%, and 11.4%) than in controls (17.1%, 1.2%, and 9.7%), respectively (P < .05).

Genotypic and allelic distribution of the XKR6 rs7014968 single-nucleotide polymorphism (SNP) in the controls and the coronary heart disease (CHD) and ischemic stroke (IS) patients. The differences in the genotypic and allelic frequencies between controls and patients were determined by the χ2 test.
Genotypic and Allelic Frequencies of the XKR6 rs7014968 SNP and the Risk of Coronary Heart Disease (CHD) and Ischemic Stroke (IS).a
Abbreviation: SNP, single-nucleotide polymorphism.
a The odds ratios (ORs), 95% confidence intervals (CIs), and P values were obtained by unconditional logistic regression analysis. Sex, age, smoking, alcohol consumption, body mass index, diabetes, mean arterial pressure, and hyperlipidemia were adjusted for in the statistical analyses.
Genotypes and Serum Lipid Levels in Controls
The association between the genotypes of the XKR6 rs7014968 SNP and serum lipid parameters in controls is presented in Figure 2. Serum TC levels in controls were different between the TT and CT/CC genotypes (P < .05). The C allele carriers had higher serum TC levels than the C allele noncarriers.

Association between the XKR6 rs7014968 single-nucleotide polymorphism (SNP) and serum lipid parameters in the controls. The values are presented as the mean ± standard deviation, and the difference was tested by analysis of covariance. Serum triglyceride levels are presented as the median (interquartile range), and the difference was determined by the Wilcoxon Mann-Whitney U test. HDL-C indicates high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol.
Genotypic Frequencies and the Risk of CHD and IS
As shown in Table 2, the XKR6 rs7014968C allele carriers had a higher risk of CHD (CT genotype: OR = 1.418, 95% CI: 0.928-2.046, P = .042; CC genotype: OR = 6.087, 95% CI: 1.835-10.600, P = .003) and IS (CT genotype: OR = 1.589; 95% CI: 1.087-2.323, P = .017; CC genotype: OR = 5.364, 95% CI: 1.571-18.313, P = .007).
Possible Interaction of the SNP With Various Factors
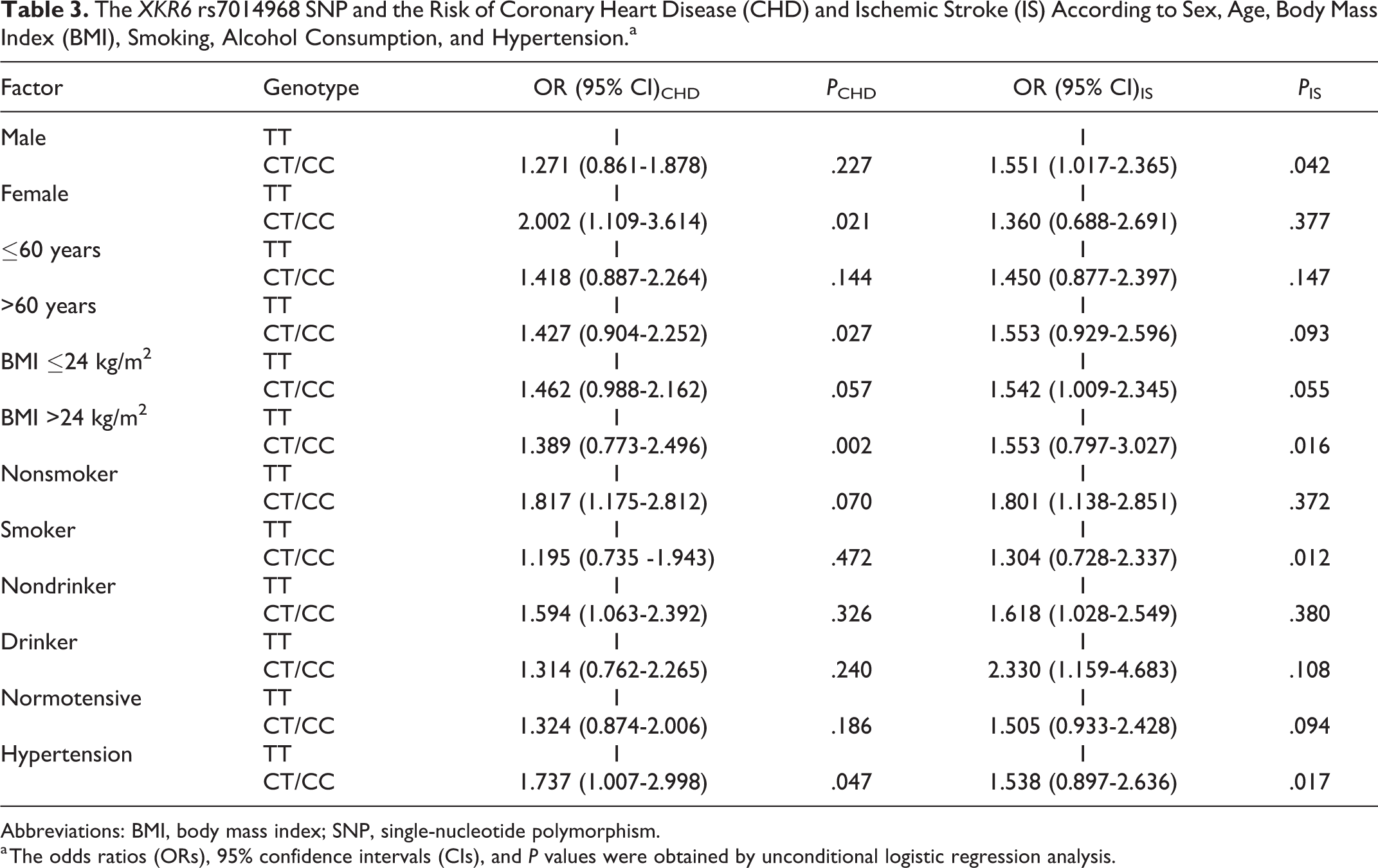
The possible effects of the interaction of the XKR6 rs7014968 SNP with various factors on the risk of CHD and IS are listed in Table 3. Unconditional logistic regression analysis showed that the patients with CT/CC genotypes had a higher risk of CHD in the female, age >60 years, BMI >24 kg/m2, and hypertension subgroups, and a higher risk of IS was observed in the male, BMI >24 kg/m2, smoker, and hypertension subgroups than in the subgroup counterparts.
The XKR6 rs7014968 SNP and the Risk of Coronary Heart Disease (CHD) and Ischemic Stroke (IS) According to Sex, Age, Body Mass Index (BMI), Smoking, Alcohol Consumption, and Hypertension.a
Abbreviations: BMI, body mass index; SNP, single-nucleotide polymorphism.
a The odds ratios (ORs), 95% confidence intervals (CIs), and P values were obtained by unconditional logistic regression analysis.
Related Risk Factors for CHD and IS
Unconditional logistic regression analysis also revealed that the incidence of both CHD and IS was positively correlated with smoking, BMI >24 kg/m2, rs7014968 CT/CC genotypes, and hyperlipidemia and negatively associated with alcohol consumption in our study populations (Table 4).
Correlative Risk Factors for Coronary Heart Disease (CHD) and Ischemic Stroke (IS).a

Abbreviation: BMI, body mass index.
a The odds ratios (ORs), 95% confidence intervals (CIs), and P values were obtained by unconditional logistic regression analysis.
Discussion
The major new findings in this descriptive association study were (1) the genotypic and allelic frequencies of the XKR6 rs7014968 SNP were different between patients with CHD and IS and controls. The CT and CC genotype and C allele frequencies were higher in patients with CHD and IS, respectively, than in controls. (2) Serum TC levels in the control group were different between TT and CT/CC genotypes, and the C allele carriers had higher serum TC levels than the C allele noncarriers. (3) The XKR6 rs7014968 SNP was associated with susceptibility to CHD and IS in our study populations, and the XKR6 rs7014968C allele carriers had a higher risk of CHD and IS. (4) There was a possible interaction between the XKR6 rs7014968 SNP and some risk factors in this study. The patients with CT/CC genotypes had a higher risk of CHD in the female, age >60 years, BMI >24 kg/m2, and hypertension subgroups, and a higher risk of IS was observed in the male, BMI >24 kg/m2, smoker, and hypertension subgroups than in the subgroup counterparts.
The genotypic and allelic frequencies of the XKR6 rs7014968 SNP in different racial/ethnic groups are not well known. According to the International 1000 Genomes database (https://www.ncbi.nlm.nih.gov/variation/tools/1000genomes/), the minor C allele frequency of the XKR6 rs7014968 SNP was 1.52% in Utah residents (CEPA) with Northern and Western European Ancestry (CEU); 2.33% in Bengalis from Bangladesh (BEB); 4.10% in Americans of African Ancestry in the Southwestern USA (ASW); 4.26% in Colombians from Medellin, Colombia (CLM); 6.77% in African Caribbean individuals in Barbados (ACB); 9.52% in Southern Han Chinese; 11.17% in Han Chinese in Beijing, China (CHB); and 12.37% in Chinese Dai in Xishuangbanna, China (CDX). In the present study, we showed that the C allele frequency in the Southern Han Chinese population was 9.7% in controls, 12.9% in with patients CHD (P = .012 vs controls), and 11.4% in patients with IS (P = .016 vs controls). These findings suggest that the XKR6 rs7014968 SNP may have racial/ethnic and population specificity. However, these findings need to be confirmed in the other ethnic groups or populations with larger sample sizes.
The potential association between the XKR6 rs7014968 SNP and plasma or serum lipid levels in humans has not been evaluated previously. In 2 previous genome-wide association and Mendelian randomization studies, the XKR6 rs7819412 SNP has been associated with increased blood TG levels and type 2 diabetes mellitus in Europeans. 39,40 More recently, we also showed that the XKR6 rs7819412 SNP was associated with serum TC levels in patients with IS and serum TG levels in patients with CHD. The XKR6 rs7819412A allele carriers had higher serum TC levels in patients with IS and higher TG levels in patients with CHD than the rs7819412A allele noncarriers. 23 In the current study, we revealed that serum TC levels in the controls were significantly different between TT and CT/CC genotype carriers, and the patients with CT/CC genotypes had higher serum TC levels than those with the TT genotype. A number of literatures have showed that dyslipidemia is closely related to the occurrence and development of atherosclerosis and cardiovascular disease. Thus, these results suggest that the XKR6 SNPs may affect the risk of ischemic cardiovascular disease by affecting certain serum lipid components. But this association between the XKR6 rs7014968 SNP and serum TC levels needs to be confirmed by proteomics study in further research.
The association between the XKR6 rs7014968 SNP and ischemic cardiovascular disease is not well known. Our previous study showed that the rs7819412A allele was associated with a high risk of CHD (adjusted OR = 1.38, 95% CI: 1.042-1.827) and IS (adjusted OR = 1.365, 95% CI: 1.019-1.805). 23 In the present study, we found that the XKR6 rs7014968C allele carriers had a higher risk of CHD (CT genotype: OR = 1.418, 95% CI: 0.928-2.046, P = .042; CC genotype: OR = 6.087, 95% CI: 1.835-10.600, P = .003) and IS (CT genotype: OR = 1.589; 95% CI: 1.087-2.323, P = .017; CC genotype: OR = 5.364, 95% CI: 1.571-18.313, P = .007). These results suggest that the XKR6 rs7014968 SNP may be a genetic risk factor for ischemic cardiovascular disease.
Although the effect of the interaction between genes and the environment on the risk of ischemic cardiovascular disease is not fully understood, the potential interaction between the XKR6 rs7014968 SNP and some risk factors was also observed in this study. The patient with CT/CC genotypes were associated with an increased risk of CHD in the female, age >60 years, BMI >24 kg/m2, and hypertension subgroups and an increased risk of IS in the male, BMI >24 kg/m2, smoker, and hypertension subgroups. However, these findings have yet to be confirmed by further research.
Limitations
The present study may have several limitations. First, the number of controls and patients was relatively small compared with previous studies. Second, many patients with CHD and IS were taking some drugs that may affect serum lipid levels. Therefore, we could not detect an association between the XKR6 rs7014968 SNP and serum lipid levels in the CHD and IS groups. Third, although several environmental factors, such as sex, age, blood pressure, cigarette smoking, BMI, and alcohol consumption, were adjusted for in the statistical analysis, some general characteristics were different between the patient and control groups. Finally, although we observed that the XKR6 rs7014968 SNP was associated with serum TC levels in controls and the risk of CHD and IS, other studies should be carried out to further clarify the mechanism.
Conclusions
This study showed that the genotypic and allelic frequencies of the XKR6 rs7014968 SNP were significantly different between the patients with CHD and IS and controls. The XKR6 rs7014968C allele frequency was higher in the patients with CHD and IS than in the controls (P < .05 for each). The C allele carriers in the control group had higher serum TC levels than the C allele noncarriers. The C allele carriers were associated with an increased risk of CHD and IS. There may be an interaction between the XKR6 rs7014968 SNP and some risk factors. These results suggest that the XKR6 rs7014968 SNP may be a new genetic marker for CHD and IS in our study populations. The association between the XKR6 rs7014968 SNP and ischemic cardiovascular disease may be partly explained by increasing serum TC levels in our study populations.
Footnotes
Authors’ Note
K.-G.L. conceived the study, participated in the design, undertook genotyping, performed the statistical analyses, and drafted the manuscript. R.-X.Y. conceived the study, participated in the design, carried out the epidemiological survey, collected the samples, and helped to draft the manuscript. F.H., W.-X.C., J.-Z.W., and X.-L.C. carried out the epidemiological survey and collected the samples. All authors read and approved the final manuscript.
Acknowledgments
The authors would like to acknowledge all the participants in this study and the staff from the Guangxi Key Laboratory Base of Precision Medicine in Cardio-cerebrovascular Disease Control and Prevention.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Natural Science Foundation of China (No: 81460169). The funding body played no role in the design of the study; the collection, analysis, or interpretation of data; or in the writing of the manuscript.