
Abstract
People with HIV (PWH) have an increased prevalence of cardiovascular disease (CVD) compared to uninfected patients. Lipoprotein-associated phospholipase A2 (Lp-PLA2) catalyzes the synthesis of pro-inflammatory lipids that recruit monocytes. Current guidelines for assessing cardiovascular risk in HIV-infected patients suggest that Lp-PLA2 may be a useful surrogate marker for CVD health in this patient population. Lipoprotein-associated phospholipase A2, lipids, glucose, physical parameters, and carotid intimal–medial thickness (CIMT) were measured in 98 participants (49 HIV-uninfected, 27 antiretroviral therapy [ART]-naive PWH, and 22 ART-treated PWH). HIV viral load (VL) and CD4+ T-cell count were measured in HIV-infected participants. Lipoprotein-associated phospholipase A2 was increased in participants on protease inhibitor (PI) ART (median 50.5 vs 127.0 nmol/mL, P = .05) and correlated with age, body mass index, and cholesterol. Lipoprotein-associated phospholipase A2 was not related to Framingham risk score or CIMT but correlated directly with VL (r = .323, P = .025) and inversely with CD4+ T-cell count (r = −.727, P < .001). Lipoprotein-associated phospholipase A2 was increased in HIV-infected participants on PIs and correlated strongly with VL and CD4+ T-cell count suggesting that HIV-associated inflammation is linked to increased Lp-PLA2, providing a mechanistic link between HIV and CVD.
Introduction
Access to antiretroviral therapy (ART) has increased the life expectancy of people with HIV (PWH). 1 Although there has been a decrease in the prevalence of opportunistic infections, PWH are more likely to develop noncommunicable diseases including cardiovascular disease (CVD). The risk of CVD is estimated to be 60% higher in patients with HIV infection, and the relative risk is increased 2-fold even in patients on ART. 2 Cardiovascular disease was the cause of mortality in patients undergoing planned interruption of ART, focusing research interest on validation of biomarkers to assess CVD risk in these patients. 3 The pathogenesis of CVD in PWH is multifactorial. Immune activation and chronic inflammation, associated with low-grade viral replication, microbial translocation, and opportunistic diseases, directly impacts the endothelial surface and activates leukocytes, specifically monocytes, which are implicated in plaque formation. 4 People with HIV may have underlying traditional risk factors and are more likely to use tobacco. 5 Although suppression of viral replication generally protects against CVD, certain ART drugs including the protease inhibitors (PIs) cause disorders in lipid metabolism.
Cardiovascular disease risk assessment tools, validated in the general population, such as the Framingham risk score (FRS), convert clinical risk factors into a summary estimate of the likelihood of a CVD event over a specified period. The scores can underestimate the individual patient risk 6 and may have limited utility in PWH, as HIV-specific risk factors including the use of PI and viral burden are not always included. 7
Various biomarkers have been assessed in CVD risk evaluation. In PWH, inflammatory changes (cytokines and leukocyte activation), changes in coagulation proteins, presence of oxidized lipids, and adhesion markers have been measured to identify a robust predictive model. 8 Lipoprotein-associated phospholipase A2 (Lp-PLA2), an enzyme secreted by leukocytes and liver cells, circulates primarily complexed to low-density lipoprotein (LDL). 9 Lipoprotein-associated phospholipase A2 hydrolyzes phospholipids to produce metabolically active lipid mediators including pro-inflammatory free fatty acids. These products recruit T-cells and monocytes, key effectors of atherosclerotic plaque formation. Lipoprotein-associated phospholipase A2 is overexpressed in macrophages in the fibrous cap of unstable atherosclerotic coronary lesions. 10 The relationship between Lp-PLA2 and HIV has been extensively studied with early reports in both simian and human leukocyte models suggesting that Lp-PLA2 synthesis, promoted by CD4–HIV envelope interactions, could facilitate viral integration into host cells by destabilizing the cell membrane. This permissive effect could be further enhanced by the T-cell proliferation and activation in response to pro-inflammatory lipid mediators. 11
Lipoprotein-associated phospholipase A2 has been extensively evaluated in clinical cohorts. It correlates with plaque formation and CVD risk and identifies patients at risk of recurrent cardiovascular events. 10 Lipoprotein-associated phospholipase A2 was incorporated into the American Association of Clinical Endocrinologists/American College of Endocrinology Guidelines for management of dyslipidemia and prevention of CVD as a nontraditional risk factor. Cardiovascular disease risk is elevated in patients with raised Lp-PLA2 (generally considered as >30 nmol/mL) 12 and C-reactive protein levels, even in the presence of a moderately increased LDL. 13 Studies suggest PWH have higher Lp-PLA2 levels than uninfected patients, independent of triglyceride and LDL levels. 14 The elevated levels persist with viral suppression. Levels of Lp-PLA2 may also guide both ART regimen choice (tenofovir may reduce Lp-PLA2 levels) and use of ancillary risk modifiers such as statins. Most studies measured Lp-PLA2 levels in patients with controlled HIV viraemia. 15
The aim of this study was to investigate Lp-PLA2 levels of HIV-infected patients (ART-naive and treated) enrolled in large cross-sectional study in South Africa and to investigate relationships between this marker, other measures of CVD risk, and markers of viral control.
Methodology
Patient Recruitment
The study was approved by the Human Research Ethics Committee (Medical) of the University of the Witwatersrand (Protocol number M160131). Ninety-eight patients, enrolled in a larger study to evaluate CVD risk in PWH in Johannesburg, South Africa, from 2016 to 2017, were included. Twenty-seven HIV-infected, ART-naive participants and 22 HIV-infected participants on stable PI-containing ART regimen were compared with 49 age- and sex-matched uninfected controls. Participants were considered ART naive if they had received no ART or ART for less than 6 weeks. The ART-treated participants, treated with a PI-containing regimen for at least 48 weeks, showed viral suppression. Demographic and cardiovascular risk factors were collected using a modified version of the World Health Organization STEPwise approach to Surveillance (WHO STEPS) instrument. 16 Blood was collected for measurement of fasting glucose and lipid levels and Lp-PLA2. Physical examination included measurement of height, weight, waist and hip circumference, and blood pressure. The FRS was computed to estimate a cumulative 10-year CVD risk. Left and right carotid intima–media thickness (CIMT) was measured sonographically at 3 standardized angles using the Meijer Arc. Measurements were semiautomated but manually corrected if required. Plasma Lp-PLA2 levels were measured on the Roche Cobas analyzer using an enzymatic assay (Diazyme Laboratories, Poway, California).
Statistical Analysis
Because of the small number of participants per group, continuous variables were expressed using median with minimum and maximum values or count with percentage. Baseline variables across the 3 groups were compared using a Kruskal-Wallis test for continuous outcomes and a χ2 test for categorical outcomes. The LP-PLA2 was correlated with age, body mass index (BMI), waist-to-hip circumference, lipid subcomponents, and glucose using a Pearson correlation coefficient.
In a multivariable regression, the LP-PLA2 levels in the 3 groups were adjusted for age, gender, LDL levels, BMI, and smoking. The relationship between Lp-PLA2 levels and FRS or CIMT was examined in a multivariable regression considering HIV and ART status. Finally, the relationship between LP-PLA2 levels of all viremic participants and log-viral load and CD4-cell count were analyzed using a Pearsons correlation coefficient. A P value of ≤.05 was considered significant. Statistical analyses were performed using IBM SPSS Statistics version 25 (SPSS, Chicago, Illinois).
Results
The baseline characteristics for the 3 participant groups are included in Table 1. With the exception of viral load and CD4+ T-cell count, no significant differences were noted between the populations.
Characteristics of the Patient Population at the Time of Analysis (All Values Expressed as a Median and Range Unless Otherwise Specified).
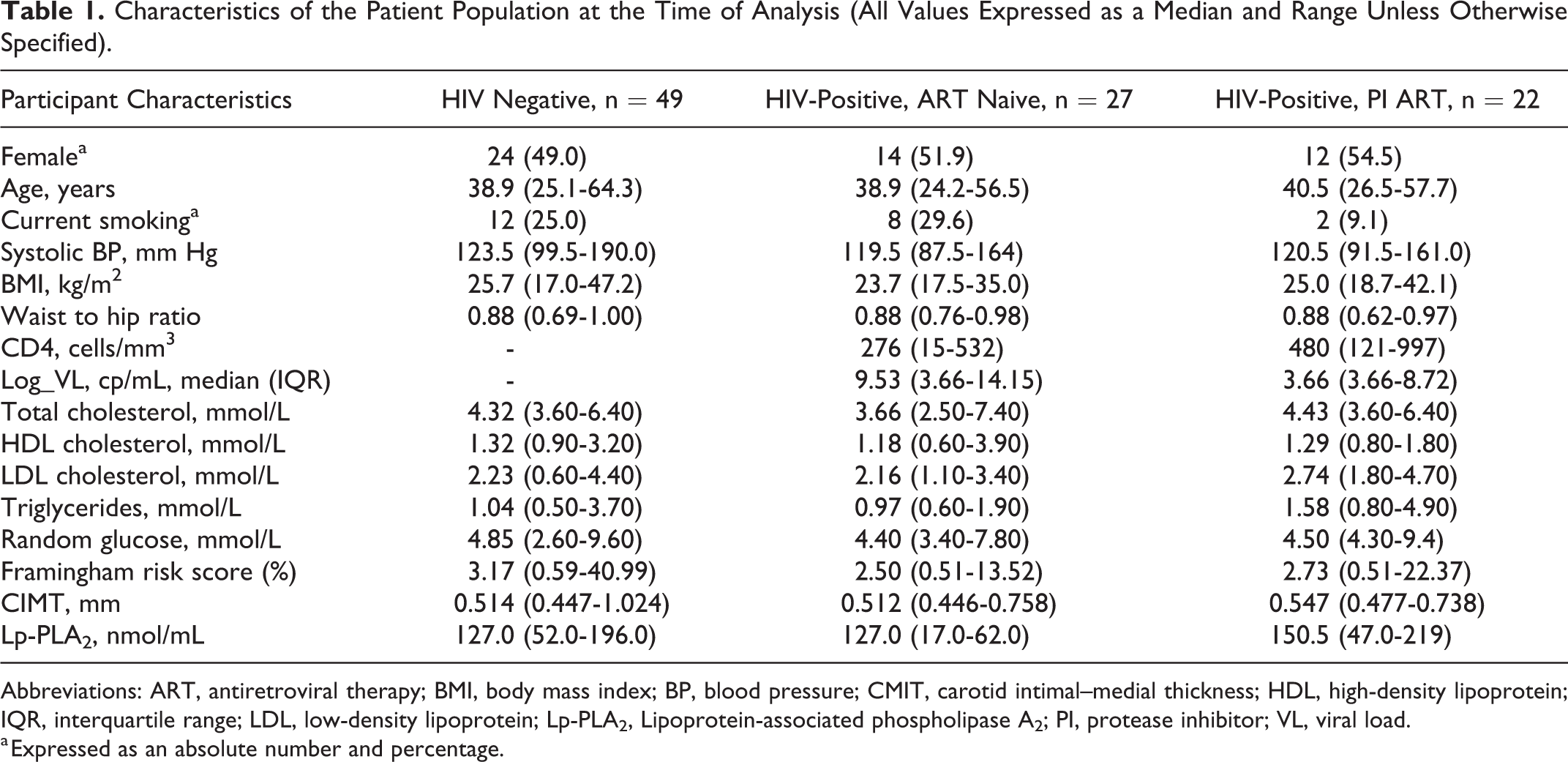
Abbreviations: ART, antiretroviral therapy; BMI, body mass index; BP, blood pressure; CMIT, carotid intimal–medial thickness; HDL, high-density lipoprotein; IQR, interquartile range; LDL, low-density lipoprotein; Lp-PLA2, Lipoprotein-associated phospholipase A2; PI, protease inhibitor; VL, viral load.
a Expressed as an absolute number and percentage.
We correlated Lp-PLA2 with traditional cardiovascular risk factors, with carotid artery intimal thickness and with the FRS in all 3 population groups. The Lp-PLA2 did not show a significant relationship with either CIMT or FRS in HIV-uninfected (median = 0.514 nmol/mL, P = .44 and median = 3.17 nmol/mL, P = .92, respectively), ART-naive HIV-infected participants (median = 0.512 nmol/mL, P = .52 and median = 2.50 nmol/mL, P = .92, respectively) or HIV-infected participants on second-line ART (median = 0.547 nmol/mL, P = .48 and median = 2.73 nmol/mL, P = .94).
As expected, patients on PI treatment had significantly higher LDL (median = 2.74 mmol/L, P < .001), triglycerides (median = 1.58 mmol/L, P < .006), and total cholesterol levels (median = 4.43 mmol/L, P = .02) than either uninfected patients or patients who were ART naive. Levels of Lp-PLA2 were increased in patients on PI-containing ART regimens (median = 150.5 nmol/mL vs 127.0 nmol/mL, P = .05) and correlated with age (r = .25, P < .001), BMI (r = .73, P = .04), total cholesterol (r = .21, P = .04), and LDL-cholesterol (r = .40, P < .001) in this population. The significant higher levels of Lp-PLA2 for participants on ART did not persist when LDL levels were considered.
Of interest, Lp-PLA2 correlated with viral load (r = .323, P = .025). When patients with undetectable viremia were excluded, the correlation became more pronounced (r = .653, P < .001). There was an inverse relationship with CD4+ T-cell count, but this reached only significance in the virally unsuppressed ART-naive participants (r = .727, P < .001).
Conclusion
Lipoprotein-associated phospholipase A2 is a phospholipase that complexes with LDL and catalyzes the release of pro-inflammatory lipid mediators. It has been linked to CVD risk (plaque formation and instability) specifically in patients with underlying inflammatory disease. Studies, generally performed on patients with controlled viremia, have demonstrated elevated levels of Lp-PLA2. 14 In this study, we assessed Lp-PLA2 utility when compared to traditional CVD risk factors and also in ART-naive, HIV-infected participants and participants on a PI-containing ART regimens.
Lipoprotein-associated phospholipase A2 levels were only significantly increased in HIV-infected participants in this cross-sectional study on a PI-containing ART regimen. This increase reflected LDL levels and may indicate the general dyslipidemia associated with PI-containing drug regimens. 17 Studies suggest that the benefits of ART initiation outweigh the risks of initiating a PI for CVD outcomes. 18 Lipoprotein-associated phospholipase A2 correlated with LDL and total cholesterol that are risk factors for atherosclerosis, although there was no convincing relationship with the FRS or the CIMT. The FRS has been criticized for both under- and overestimating cardiovascular risk in the HIV-infected population. 19
More importantly, Lp-PLA2 correlated strongly with viral load and CD4+ cell count, specifically in those patients with detectable viremia. Persistent chronic inflammation secondary to viral factors including low-grade viral replication, opportunistic infections, and bacterial translocation is associated with endothelial dysfunction and coagulation abnormalities. 20 –22 Lipoprotein-associated phospholipase A2 is a lipid regulator of inflammatory pathways and is a biomarker of inflammation-induced endothelial dysfunction. The significant relationship with virological status in this population provides a link between active viremia and the mechanistic development of CVD in these patients.
This study has a number of limitations. We did not access patients who were not on a PI-containing regimen which may explain the discrepancies of our findings and other studies looking at Lp-PLA2 in HIV-infected patients. In addition, this study was cross-sectional, and it would be useful to examine the patients with increased Lp-PLA2 levels longitudinally to assess the contribution to CVD risk. Finally, we did not include measurement of Highly sensitive C-reactive protein (hs-CRP) which would have been an important indicator of inflammation. Despite these limitations, we are of the opinion that this enzyme may drive atherosclerosis in HIV-infected patients, and its utility in clinical care should be investigated in prospective studies.
Footnotes
Authors’ Note
Elizabeth S. Mayne and Susan Louw contributed equally to this article.
Acknowledgments
Technical support was provided by Kat Medical (Mr Keith Dodkins), Ms Nomampondo Camane (Roche), and Dr Agnes Magwete.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Discovery Foundation Academic Excellence award (Dr Elizabeth S. Mayne) and a Thuthuka Grant from the South African National Research Foundation (TTK20110801000022866) awarded to Dr Elizabeth S. Mayne.