
Abstract
Pregnancy is a hypercoagulable state associated with an increased risk of venous thrombosis. Calibrated automated thrombogram (CAT) is a test to monitor the thrombin generation (TG), a laboratory marker of thrombosis risk, and increases during normal pregnancy, but it is still unclear whether TG is related to the use of insulin in pregnant women with gestational diabetes mellitus (GDM). We performed thrombin generation by CAT on 135 normal pregnant women, including 43 in first trimester, 32 in second trimester, 60 in third trimester, respectively; 68 pregnant women with GDM were also enrolled, 19 patients with GDM using insulin to control blood glucose and 49 patients control their blood glucose through diet and exercise with noninsulin treatment. The overall CAT parameters were calculated using descriptive statistics method with mean ± standard deviation. Mean endogenous thrombin potential, peak thrombin generation, and StartTail time increased significantly with the pregnancy. There was no significant difference in TG test parameters except StartTail time(P = .003) in insulin-treated GDM group when compared to those without insulin in the GDM group. The normal ranges for CAT parameters in pregnant women were determined. Thrombin generation increased significantly in first trimester and remains stable in second and third trimester. The use of insulin in patient with GDM did not affect thrombin generation test. Our study helps to establish the reference range of thrombin generation in Chinese normal pregnant population and provide more basis to predict the risk of thrombus complicating during pregnancy.
Introduction
Pregnancy is a risk factor for venous embolism and is associated with hypercoagulability. 1 Most of the pregnancy complications and adverse pregnancy outcomes are related to maternal thromboembolic disease. The most common abnormality is the prethrombotic state, which is mainly related to the endothelial function injury or the change in the anticoagulation protein C system, resulting in an increase in the formation of the thrombin, which further increases the hypercoagulability and increases the tendency to be embolized. 2
The traditional coagulation test, represented by Prothrombin Time/Activated Partial Thromboplastin Time (PT/APTT), is not sensitive to hypercoagulability and is not suitable for evaluating thrombus risk. The global coagulation assay such as calibrated automated thrombogram (CAT) and thromboelastogram have been demonstrated to more accurately reflect the thrombotic phenotype than measuring individual parameters of the coagulation cascade. 3 –5 Many diseases have been studied related to higher level of thrombin generation such as malignant tumors. 6,7 There are few reports of thrombin generation in pregnant women, and studies have shown racial differences between caucasian and African women. 1,8 –10 But thrombin generation in Chinese pregnant women has not been studied. Therefore, the purpose of this study was to study the level of thrombin generation in Chinese normal pregnant women through the global coagulation assay, thrombin generation test (TGT).
Gestational diabetes mellitus (GDM) is a common complication during pregnancy. The average incidence of GDM in pregnant women was 6.6%. Gestational diabetes mellitus can lead to vascular endothelial injury and changes in coagulation system, resulting in hypercoagulability and prethrombotic state. 11 It has been reported that GDM is a risk factor for venous thromboembolism (VTE), which is a serious threat to maternal and fetus health, 4,12 –14 and hyperinsulinemia affects coagulation activation and causes impairment of fibrinolysis. 15 Therefore, another aim of this study was to study the changes in thrombin generation and the effect of insulin use on the level of thrombin generation in patients with GDM and to provide evidence for the study of hypercoagulability of GDM.
Materials and Methods
Participants
From January 2017 to December 2017, a total of 135 normal pregnant women, including 43 in first trimester, 32 in second trimester, and 60 in third trimester, were recruited consecutively from the Beijing Civil Aviation General Hospital. At the same time, 68 pregnant women with GDM were enrolled in this study, 19 patients with GDM using insulin to control blood glucose, and 49 patients control their blood glucose through diet and exercise with noninsulin treatment. The specific ages of our study participants and gestational weeks data are shown in Table 1. Diagnose of GDM were based on the GDM guidelines issued by the American Diabetes Association (ADA) in January 2011 16 ; all undiagnosed pregnant women are given 75 g of oral glucose tolerance test (OGTT) between 24 and 28 weeks of gestation, with a threshold of 5.1 mmol/L of fasting blood glucose, 10.1 mmol/L of 1 hour blood glucose, and 8.5 mmol/L of 2 hour blood glucose.
The Age and Pregnant Weeks Distribution of Enrolled Volunteers.

Abbreviation: GDM, gestational diabetes mellitus.
Exclusion Criteria
History of DM or GDM during former pregnancies, liver dysfunction, renal dysfunction, preeclampsia/eclampsia, endocrine disorders, use of medications with known effects on glucose metabolism, and hemostatic system such as antidiabetic medications, aspirin, heparin, and enoxaparin. The use of human blood samples in this study were approved by the Ethical Committee of Civil Aviation General Hospital. Data on clinical and biological characteristics were also from hospital medical records. Written informed consent was obtained for every participant.
Collection of Blood Samples
Vacutainer method was used to collect the blood sample. Blood samples were collected on 3.2% (0.109 M) sodium citrate into Vacutainer tubes (363083, BD, roborough plymouth, United Kingdom) at the anticoagulant to blood ratio of 1:9. The needle used for collection was 20-Gauge wide in order to prevent cell damage/hemolysis. While collecting the blood sample, the initial 2 mL of blood sample was discarded using a discard tube for fear of contamination of tissue factor and then collected into Vacutainer tubes (BD Biosciences, New Jersey, USA). A total of 2.7 mL of blood sample was collected into standard tubes containing 0.3 mL of 0.109 M trisodium citrate. Platelet-poor plasma (PPP) was obtained by centrifugation at 2500 g for 20 minutes at 4°C. The plasma sample was stored at −80°C until it was analyzed.
Thrombin Generation Test
Thrombin generation was measured by CAT and Fluoroscan Ascent fluorometer (Thermoscientific Labsystems OY, Helsinki, Finland), as previously described,. 3,17,18 using PPP reagent containing final concentrations of 5 pM tissue factor and 4 M phospholipids (normal PPP reagent, Diagnostica Stago, Asnieres, France). Assay were performed by means of Fuoroskan Ascent plate reader (Thermoscientific Labsystems) and Thrombinoscope software (Thrombinoscope BV, Maastricht, the Netherlands) as described by the manufacturer. All samples were assessed concurrently, alongside a standardized plasma (TGT-RP), to minimize the effect of interassay variability. The most important parameters of TG test were the following: endogenous thrombin potential (ETP; nM × min, the area under the curve) representing overall coagulating capacity, lag time (minutes, time to first thrombin production), peak thrombin concentration (nM thrombin), time to peak (minutes), velocity, and so on. The fluorescent signal was also measured in time at excitation and emission wavelengths of 390 nm and 460 nm, respectively. The intensities of fluorescence were read, and the thrombin generation curves were produced by thrombinscope software (version 5.0.029; Thrombinoscope BV).
Statistical Analysis
All parameters from thrombin generation test were collected for statistical analysis. Statistics were computed using SPSS 19.0 (SPSS, Inc, Chicago, Illinois). The ranges of CAT parameters were expressed as mean ± standard deviation. Tests such as t-test, 1-way analysis of variance, Wilcoxon W, and Kruskal-Wallis test were performed to analyze the parameter differences in thrombin generation. Any statistically significant differences (P < .05) were further analyzed by pairwise Mann-Whitney U test and Dunn test. Correlations between pregnant women and thrombin generation values were calculated using Pearson correlation, and P value was corrected with Bonferroni method. A 2-tailed P value of <.05 was considered statistically significant. Correlations were computed using R language (R Core Team; R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria).
Result
One hundred thirty-five women with normal pregnancies were enrolled in this study in 2017. Women were classified by trimester of pregnancy, 68 women with GDM pregnancies. Clinical data of the entire population and the study group are reported in Table 1.
The Normal Range of CAT Parameters in Chinese Pregnancies
The specimens were divided into 3 subgroups. On analysis of the mean data, there was significant increase from baseline in peak thrombin, ETP, and Velocity Index (VI), and there was no significant difference in lag time, time to peak, velocity, and α2-Macroglobulin (α2M) level during different pregnancy trimesters (Figure 1). The ETP began to increase during the first trimester of pregnancy (2007.67 ± 345.24 nM/min), then decrease in the second trimester of pregnancy (1809.81 ± 220.9), and remained unchanged in the third trimester of pregnancy (1859.74 ± 312.40); no statistically significant difference was found between the second and third trimester. Levels of peak height significantly increased from the first and second trimester (342.58 ± 53.64, 353.62 ± 43.65) and then decreased in the third trimester (323.86 ± 60.76); no statistically significant difference was observed between the first and second trimester, while there was statistically significant difference between the second and the third trimester. There was a shorter StartTail time in the second trimester (20.4 ± 2.27) than the first (22.63 ± 3.35) and third trimester (22.26 ± 2.45); there was statistically significant difference between the first and second trimesters. These values were different from those of caucasian and African population, suggesting the difference in genetic background has effect on the values of CAT parameters. Detailed results of unpaired t test are shown in Table 2.
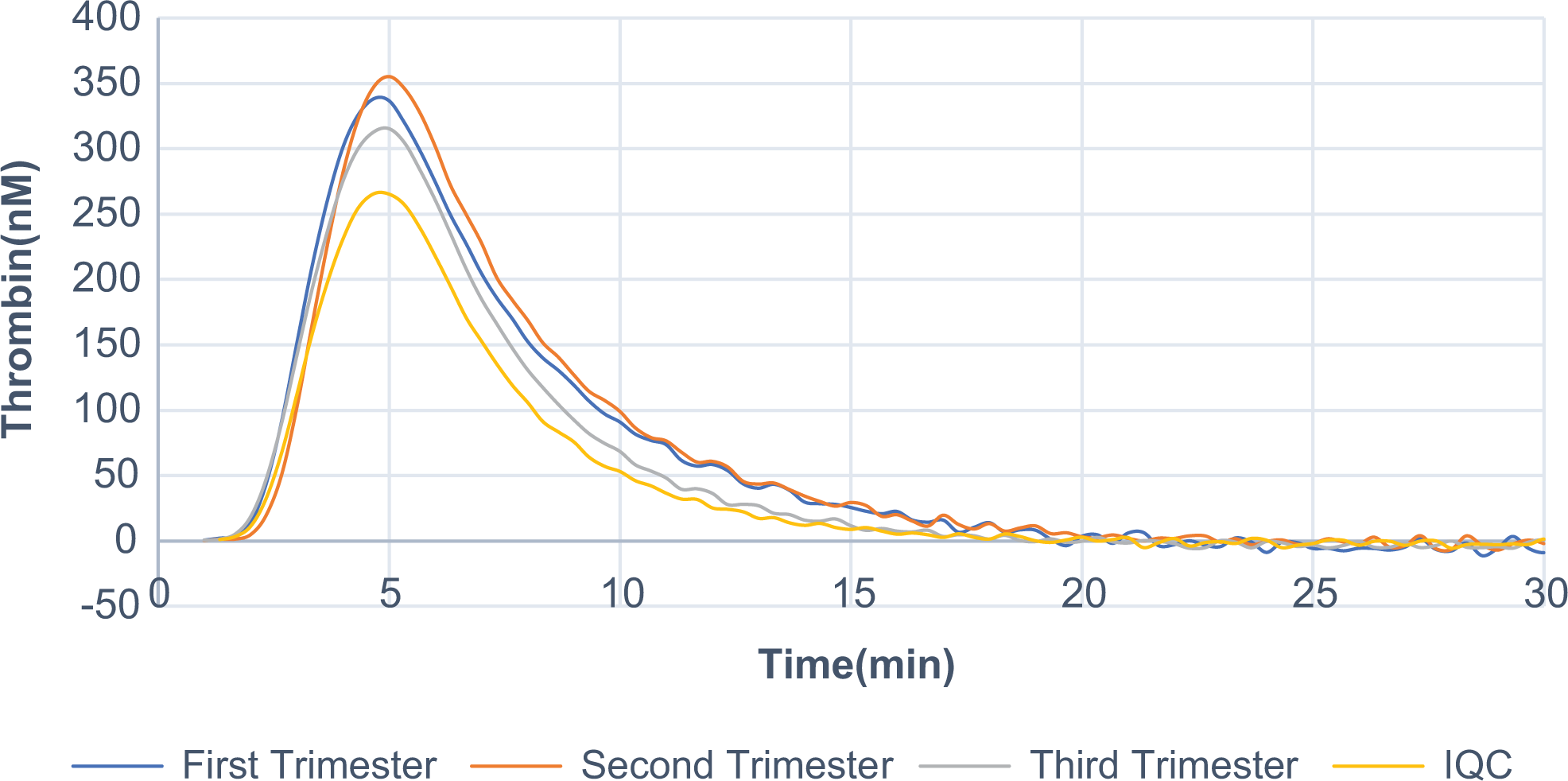
Thrombin generation curves in normal pregnancy. Curves illustrate thrombin generation during first (black curve), second (silver curve), and third (dark silver curve) trimester of pregnancy, and thrombin generation profile of our Internal Quality Control (IQC) (curve in dotted lines).
The Normal Ranges of Thrombin Generation Test Parameters in Chinese Pregnancies.

Abbreviations: ETP, endogenous thrombin potential; KW, Kruskal-Wallis test.
Correlation Between GDM and CAT Parameters
Participants were divided into 3 groups: control group, GDM treated without insulin group, and GDM treated with insulin group; all participants in control group were normal pregnant women in third trimester. There was no significant difference between control group and patients with GDM treated without insulin group in all CAT parameters, indicating the changes in coagulation factor activation and fibrinolytic system inhibitors were not significant in patients with GDM, which was consistent with the thrombin generation curve in this study, as shown in Figures 2 and 3. However, startTail time in patients with GDM treated with insulin decreased when compared to control group and patients with GDM treated without insulin; there were significant differences in StartTail time (P < .005) between the groups, while there was no significant difference in startTail time between control group and patients treated without insulin, which may suggest the effect of insulin on the anticoagulant system shortened the time of thrombin inhibition.
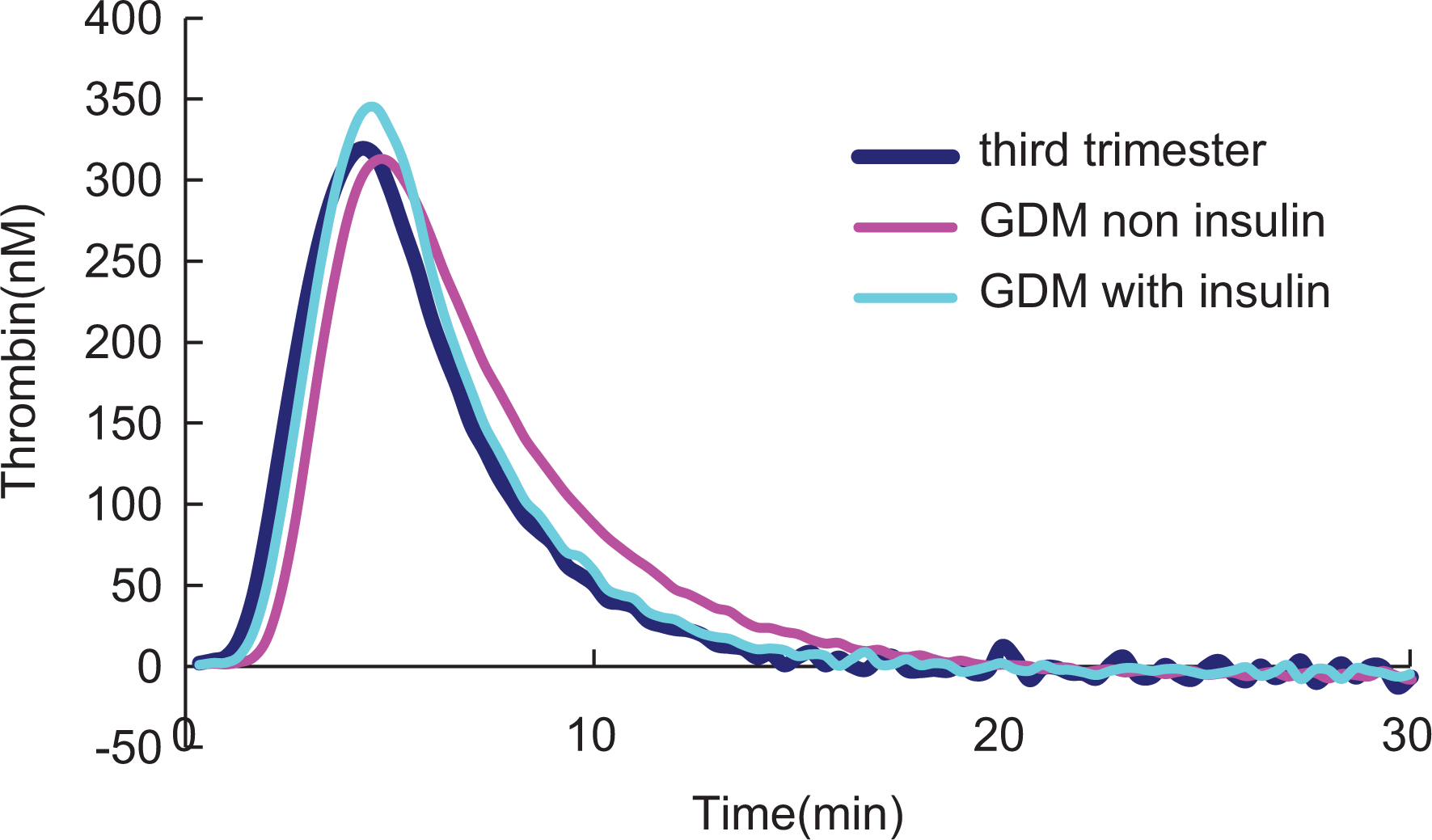
Thrombin generation curves in GDM women and controls. GDM indicates gestational diabetes mellitus.
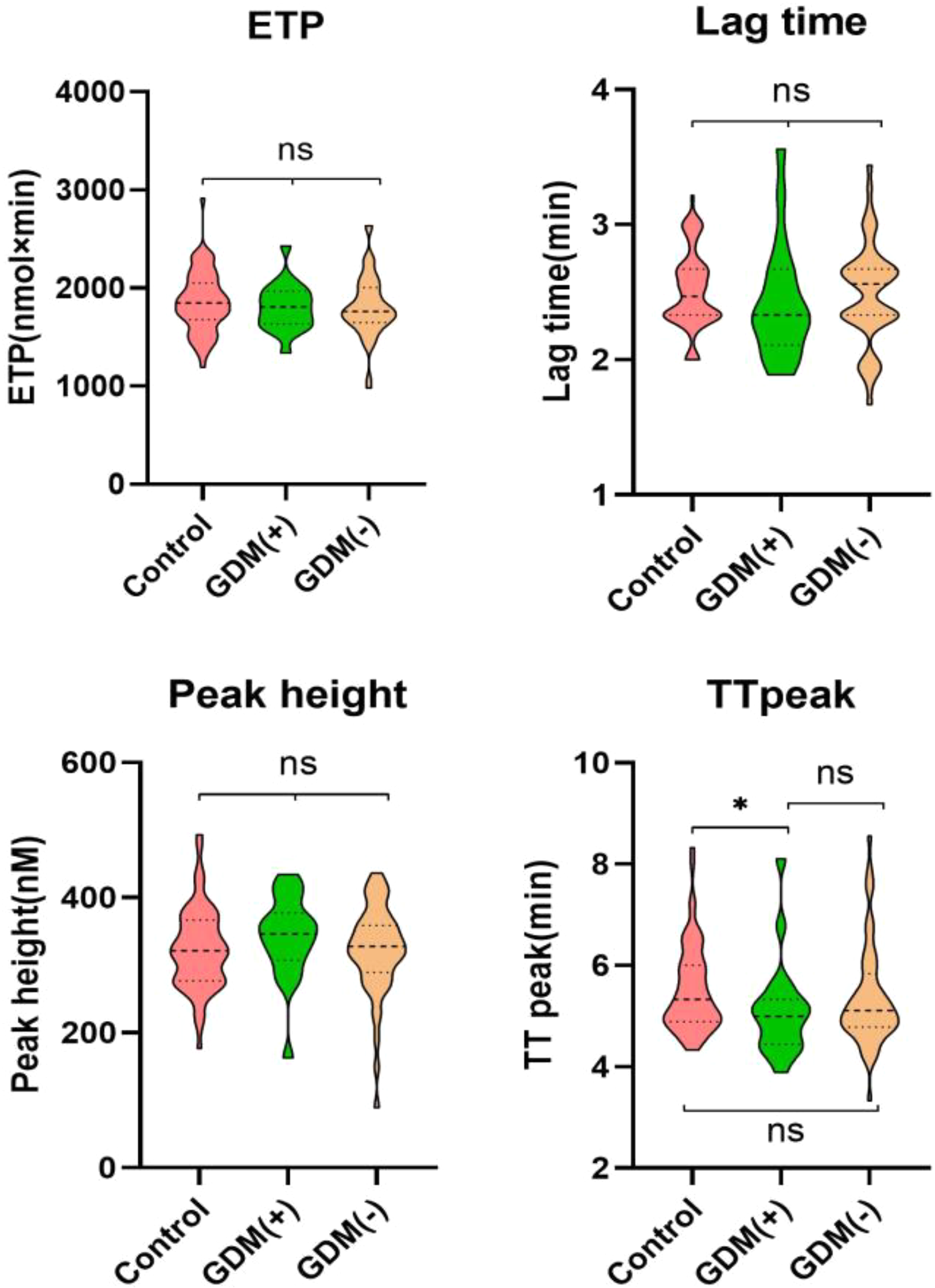
Parameters of thrombin generation test in GDM women and controls, GDM(+): GDM treated with insulin, GDM(−): GDM treated with noninsulin. GDM indicates gestational diabetes mellitus.
Discussion
The risk of VTE in pregnant women is 50 times higher than that in nonpregnant women, which is associated with hypercoagulability.
2
Physiological hypercoagulability during pregnancy is closely related to the increase in coagulation factor, the decrease in inhibitor level, and the change in fibrinolytic activity. The level of fibrinogen and
Thrombin generation test is a classical global assay. The CAT is the most sensitive and specific method to detect thrombin generation and one of the best methods to correlate with clinical bleeding or thrombotic events. 3,5,17 The main difference between TG and other conventional clotting tests is that other experiments simply describe the beginning and end of fibrin clot formation (about 5% of thrombin consumption); TG can provide more information, that is, the overall clotting potential, because thrombin generation does not stop detection when fibrin clots are produced, indicating that it has an advantage in monitoring arteriovenous thrombus.
There are few reports of thrombin generation in pregnant women, and studies have shown that there are racial differences in thrombin between caucasian and African women. 8 –10 At present, there is no report of thrombin generation in pregnant women in China. It had been reported that there is no difference in ETP levels between males and females aged between 18 and 35 years, and the ETP levels over 35 years old vary with the increase in age, 19 suggesting that a reference range for normal women should be established according to their age. Therefore, we selected Chinese women who were pregnant before the age of 35 as the study participants and reported for the first time in Chinese population that the level of ETP, the main parameter of thrombin TGT, was significantly higher than that of Internal Quality Control (IQC) (mixed plasma from normal people) in early pregnancy. However, the level of ETP decreased slightly in the second trimester and continued steadily until the third trimester, and the ETP level was higher than that of the control, as shown in Figure 1, which indicated that the body was in a hypercoagulable state. The variation trend of TGT in 3 different pregnancy periods was basically consistent with that reported by Joly et al. 10
There were few reports of thrombin generation about pregnant women, and the condition of the participants in the literature were different, such as age, race, and so on. On the other hand, the differences in experimental conditions such as the type of reagent, the concentration of activator, and the process of experiment were also different; these may result in variation of thrombin generation levels during 3 pregnancy periods. It is worth noting that compared to caucasian population, the mean ETP and peak parameters in the first and second trimesters of pregnancy of African population are higher than those of caucasian population. In our study, the mean ETP parameter was 2007.67 nM × min, close to 2126 nM × min in African population, and was higher than that in Caucasian population (1296 nM × min). However, the Mean ETP 1809.81 nM × min in the second trimester of pregnancy was similar to that in the caucasian population and was lower than that in Africa, and there was no significant difference among the 3 groups in the third trimester. The determination of the normal range of CAT parameters in Chinese pregnant women make it possible to use CAT in abnormal hypercoagulability in clinical pregnant women. But our study only provides data on pregnant women of Han nationality in China, and more differences among different ethnic groups in China need to be explored in the next step.
During the whole normal pregnancy period, the main coagulation activation indexes such as fibrinogen,
The screening standard of GDM is to perform OGTT test at 24 to 28 weeks of gestation according to GDM guidelines issued by the ADA in January 2011. Gestational diabetes mellitus usually happened in late pregnancy. Therefore, in this study, the normal late pregnancy population was selected as the control group of GDM. The changes of thrombin generation in patients with GDM were reported for the first time in our study. As shown in Table 3, there was no significant difference in the main parameter of thrombin generation level between patients with GDM and control group, but the increase in the main parameter of ETP showed that the body was also in hypercoagulable state when compared to the former IQC (normal mixed plasma).
Different Parameters of Coagulation Activation and Thrombin Generation Test Measured in GDM and Pregnancies.

Abbreviations: GDM, gestational diabetes mellitus; ETP, endogenous thrombin potential.
a GDM (+): GDM treated with insulin, GDM (−): GDM treated with noninsulin.
As reported, the prethrombotic state of GDM is mainly due to the activation of platelets and coagulation factors and the decrease in anticoagulant/fibrinolytic function. 21 Pregnancy is a physiological hypercoagulability, which can be transformed into pathological hypercoagulability due to the presence of GDM and/or eclampsia/preeclampsia. Because coagulation and fibrinolysis systems contain many factors that interact through complex pathways, it is difficult to reveal and understand the changes in coagulation function in cases of impaired glucose metabolism. In this study, a global evaluation test of coagulation function, CAT, was used. As a new research tool, there was no significant difference in the main parameters between GDM and the control group of late pregnancy, suggested that the main procoagulant factor activity or activated protein C (APC) system and thrombin inhibition factors did not affect the potential of thrombin generation. Previous studies had reported there was no significant difference between thrombin activatable fibrinolysis inhibitor (TAFI)/tissue factor pathway inhibitor (TFPI)/plasminogenactivator inhibitor type 1 (PAI-1)/tissue plasminogen activator (t-PA) and routine items (PT/APTT), only fibrinogen and PLG had difference (increased) in patients with GDM compared to the control group in the third trimester of pregnancy. 2,15 The results showed that the changes in coagulation factor activation and fibrinolytic system inhibitors were not significant in patients with GDM, which was consistent with the thrombin generation curve in this study, as shown in Figure 2. In addition, attention should be paid to the fact that although GDM is generally regarded as a high-risk factor for pregnancy VTE, whether GDM is a high-risk factor for VTE has always been reported by the Won and team. 22 The evidence for GDM as a risk factor for pregnancy VTE is inadequate, and our findings support this conclusion. Therefore, the correlation between GDM and VTE remain to be further studied.
The standard therapy of GDM is diet and exercise control. Insulin should be used when diet and exercise control is not ideal to avoid adverse maternal and child outcomes. 16 With regard to the effects of insulin use on hypercoagulability, it was reported that there was no difference on fibrinogen levels between insulin-treated GDM and noninsulin-treated GDM groups; it has also been reported that the use of insulin can reduce the body high glucose environment, but it can also cause the increase in PAI-1 and fibrinogen, which may lead to persistent hypercoagulability. In terms of clinical events, several meta-analyses suggest that the use of insulin increases the risk of cardiovascular events in patients with diabetes. 15 In this study, we found that there was no significant difference in TGT parameters except StartTail in insulin-treated GDM group compared to those without insulin in GDM group. StartTail was mainly affected by the level or function of antithrombin (AT) and α2M. 17 The results indicated that the effect of insulin on the anticoagulant system shortened the time of thrombin inhibition. Although there was no significance difference in peak height and VI between groups, the mean level of peak height and VI increased in insulin use pregnant women. It suggests that insulin use may further exacerbate the hypercoagulability. This also has a further understanding of the changes of hypercoagulability in patients with GDM having high glucose environment.
It should be pointed out that our study has some limitations. First, the sample size of this study is small. Second, as mentioned above, it is possible to detect more sensitive changes in prethrombotic state in patients with GDM through CAT, but there are no data indicating the exact time when abnormal coagulation began to change in patients with GDM. Are the results of early screening valuable for improving outcomes? What is the significance of CAT monitoring after delivery? Whether the time-advancing dynamic monitoring of CAT can better predict the events of thrombosis or hemorrhage in patients with GDM can provide the basis for timely clinical intervention and enable more patients to benefit from this test.
Conclusion
This study revealed the changes in thrombin generation in Chinese pregnant women and evaluated the effect of insulin use on coagulation status in patients with GDM. It helps to establish the reference range of thrombin generation in Chinese normal pregnancy population and provide more basis to predict the risk of thrombus complicating during pregnancy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.