
Abstract
In our study of 596 men hospitalized in the last 3 years for deep venous thrombosis-pulmonary emboli (DVT-PE), we determined the prevalence of exogenous testosterone (T) use with subsequent development of DVT-PE. Of the 596 men, 110 were now dead, 97 had cancer thought to cause DVT-PE, 250 could not be contacted, leaving 139, of whom 7 had taken T before and at the time of their admissions, 1.2% of the total cohort, a conservative estimate of the prevalence of T-associated DVT-PE. In all, 5 of the 7 DVT-PE events occurred within 3 months of initiation of T, with mean and median intervals between initiation of T and hospitalization with DVT-PE 6.7 and 2 months. Of the 7 men treated with exogenous T, all 5 men who had evaluation of thrombophilia–hypofibrinolysis were found to have previously undiagnosed familial or acquired thrombophilia or hypofibrinolysis, suggesting a thrombotic interaction between exogenous T and thrombophilia–hypofibrinolysis.
Keywords
Introduction
We initially described deep venous thrombosis (DVT), 1 pulmonary embolism (PE), amaurosis fugax, and osteonecrosis of the hips after exogenous testosterone (T) was given to 6 previously healthy men with no antecedent thrombosis and previously undiagnosed familial thrombophilia–hypofibrinolysis. Osteonecrosis may be caused, in part, by thrombophilia and hypofibrinolysis-induced thrombus of the efferent veins of the head of the femur leading to increased intracortical pressure and reduced arterial inflow, with subsequent bone hypoxia and bone death. 1 –3 After their thrombotic events, 5 of these 6 men were subsequently found to be heterozygous for the previously undiagnosed thrombophilic factor V Leiden mutation, and one had thrombophilic familial high factor VIII. 1 Subsequently, we described DVT-PE (n = 9) and osteonecrosis (n = 5) in 14 previously healthy individuals (13 men, 1 woman) with no antecedent thrombosis and previously undiagnosed thrombophilia–hypofibrinolysis. 4 These thrombotic events developed after a median of 11 months on T. 5 Of these 14 patients, 3 were found to be factor V Leiden heterozygotes, 3 had high factor VIII, 3 had plasminogen activator inhibitor 1 (PAI-1) 4G4G homozygosity, 2 had high factor XI, 2 had high homocysteine, 1 had low antithrombin III, 1 had the lupus anticoagulant, 1 had high anticardiolipin antibody-immunoglobulin (Ig) G, and 1 had no clotting abnormalities. 5 In 4 of these 13 men, DVT-PE recurred when T was continued despite therapeutic international normalized ratio (INR) on warfarin.
Since the major source of estradiol (E2) in men comes from the aromatization of T to E2, 6 we speculated 1 that when exogenous T is aromatized to E2 6 –9 and E2-induced thrombophilia is superimposed on underlying familial thrombophilia, thrombosis occurs. 1 We had previously reported in 60 men on T that 20 (33%) had high estradiol (E2 > 42.6 pg/mL). 5
We have suggested that men or women sustaining thrombotic events on T therapy should be screened for thrombophilia–hypofibrinolysis. 1
Our specific aim in the current study of 596 men hospitalized for DVT-PE was to determine the prevalence of use of exogenous T therapy with subsequent development of DVT-PE requiring hospitalization.
Materials and Methods
Patients
The procedures followed were in accordance with the ethical standards of the institutional review board (IRB) of the Jewish Hospital, Cincinnati, Ohio, which approved the research protocol. The IRB approval was given for our review of electronic medical records of men admitted to the Mercy Hospitals of Cincinnati for the past 3 years because of DVT-PE. Then, we attempted to contact the 596 patients with 1 admission for DVT-PE to review their medical history for use of exogenous T. From the cohort of 596 patients, we invited 7 men with a history of exogenous T use and a control group of 8 men without any exogenous T use for assessment of thrombophilia and hypofibrinolysis, again with signed informed consent.
There was 2-fold documentation of T use before and at the time of the DVT-PE leading to the hospitalization. First, direct interviews of the patients were carried out to identify the type of T, the dose, and whether the T had been used at the time of the thrombotic event. Second, the patients’ history was confirmed by our review of electronic medical records.
In all patients, after overnight fasting, blood was drawn in the seated position for assessment of thrombophilia and hypofibrinolysis. 10
Laboratory Assessment of Thrombophilia and Hypofibrinolysis
Polymerase Chain Reaction Assays
Polymerase chain reaction measures of thrombophilia–hypofibrinolysis (G1691A factor V Leiden, G20210A prothrombin, methylenetetrahydrofolate reductase [MTHFR] C677T-A1298C, and 4G5G plasminogen activator inhibitor activity gene mutations) were performed in all cases using previously published methods by laboratory staff blinded to the patients’ status (diagnosis and severity of disease). 11 –13
Serologic Measures of Thrombophilia
Serologic measures of thrombophilia included anticardiolipin antibodies (IgG and IgM), antigenic protein C, total and free protein S, antithrombin III, resistance to activated-protein C, activated-partial thromboplastin time, dilute Russel’s Viper Venom time, factors VIII and XI, and homocysteine. Established, previously published methods were used. 11,14
Serologic Measures of Hypofibrinolysis
Serologic measures of hypofibrinolysis, lipoprotein(a), and plasminogen activator inhibitor activity were performed using established, previously published methods. 12,15
Results
Prevalence of T use in Men Admitted With DVT-PE Over the Past 3 Years
Of the 596 men, 110 were now dead, 97 had cancer, and 250 could not be contacted, leaving 139 who were contacted, Figure 1. Of these 139 men, 132 had no T use and 7 (1.2% of the total cohort of 596) had been treated with T before and at the time of the thrombotic event, documented both by direct interview and by review of electronic medical records of prescription logs, Figure 1. The prevalence of T use before and at the time of hospitalization for DVT-PE was at least 1.2% (7 of 596).
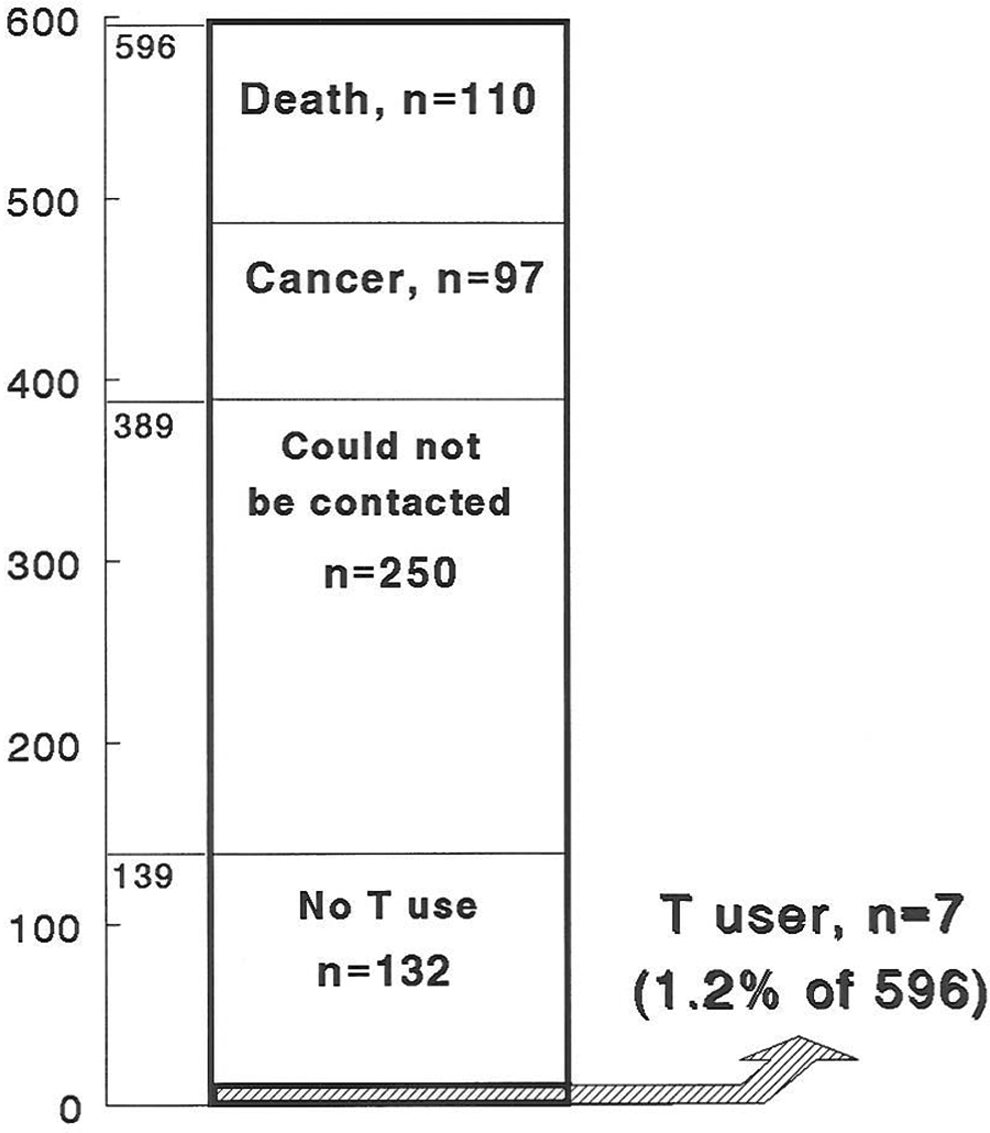
Prevalence of testosterone use before and at the time of deep venous thrombosis-pulmonary embolism requiring hospitalization in 596 men.
In 5 of the 7 cases, thrombotic events occurred ≤3 months after starting T (Table 1). The mean and median intervals between initiation of T and hospitalization with DVT-PE were 6.7 and 2 months with a range of 3 weeks to 27 months (Table 1).
Deep Venous Thrombosis/Pulmonary Embolus and Osteonecrosis Requiring Hospitalization in 7 Men After Starting Testosterone Therapy.
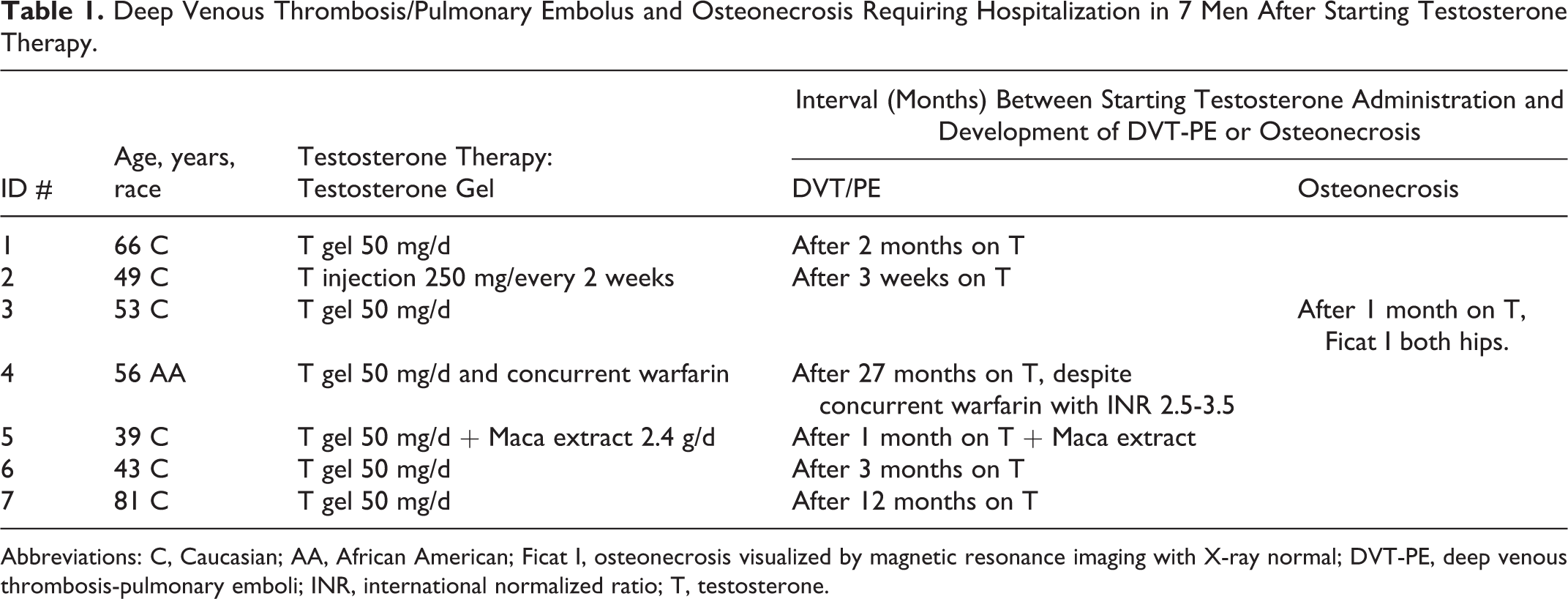
Abbreviations: C, Caucasian; AA, African American; Ficat I, osteonecrosis visualized by magnetic resonance imaging with X-ray normal; DVT-PE, deep venous thrombosis-pulmonary emboli; INR, international normalized ratio; T, testosterone.
None of these 7 previously healthy men had sustained DVT, PE, or any other thrombotic events before taking exogenous T. None of these 7 men had risk factors for thrombosis including hip-knee or superficial leg vein surgery, leg fracture or dislocation, immobilization, or trauma. Of the 7 men, 1 (#3, Tables 1 and 2) smoked cigarettes (1 pack/d).
Previously Undiagnosed Thrombophilia and Hypofibrinolysis in 15 Men Hospitalized Because of DVT-PE and Osteonecrosis, 7 of Whom had Taken Exogenous Testosterone Before and at the Time of their DVT-PE.
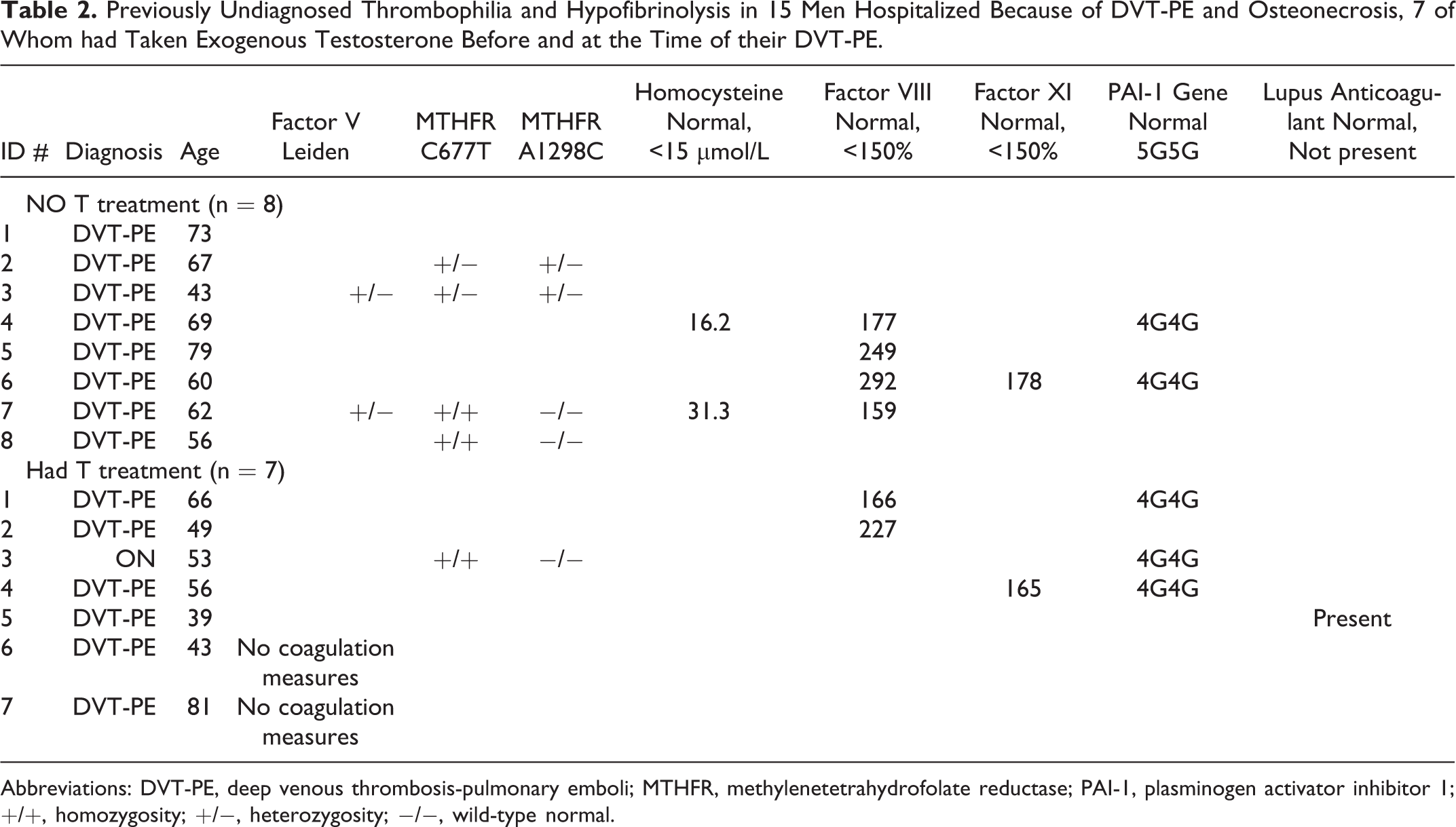
Abbreviations: DVT-PE, deep venous thrombosis-pulmonary emboli; MTHFR, methylenetetrahydrofolate reductase; PAI-1, plasminogen activator inhibitor 1; +/+, homozygosity; +/−, heterozygosity; −/−, wild-type normal.
Case #3 was admitted with a diagnosis of DVT-possible PE but was then also found to have bilateral hip osteonecrosis (Table 1). Case #4 developed DVT-PE on T therapy despite anticoagulation with coumadin with INR levels ranging from 2.5 to 3.5 before T and while T was taken (Table 1).
As displayed in Table 1, of the 7 men with DVT-PE and osteonecrosis after starting T therapy, most were middle aged (range 39-64 years), and 1 was aged 81years. Of the 7 men sustaining thrombotic events after starting T, 6 were using T gel, 50 mg/d, and 1 was using T by injection 250 mg every 2 weeks (Table 1). One patient, #5, was also using Maca extract as an aphrodisiac ( Table 1). 16,17
Thrombophilia–hypofibrinolysis in Men With DVT-PE Taking and not Taking T
None of the 7 men who had taken T before and at the time of their DVT-PE had previous thrombotic episodes, and none had previous evaluation of thrombophilia–hypofibrinolysis. Of the 7 men treated with exogenous T, 5 had measures of thrombophilia–hypofibrinolysis and all 5 had ≥1 procoagulant (Table 2). None of the men had any previous studies of thrombophilia–hypofibrinolysis. Of these 5 men, 1 had the lupus anticoagulant, 3 had the hypofibrinolytic 4G4G mutation of the PAI gene, 2 had high factor VIII, 1 had high factor XI, and 1 had MTHFR C677T homozygosity (Table 2).
None of the 8 control men without prior T use had previous thrombotic episodes, and none had previous evaluation of thrombophilia–hypofibrinolysis. Of the 8 controls without exogenous T treatment, 7 had ≥1 procoagulant (Table 2). Of these 8 men, 2 were heterozygous for the factor V Leiden mutation, 2 were MTHFR C677T homozygotes, 2 were MTHFR C677T/A1298C compound heterozygotes (1 of whom had high homocysteine [31.3 µmol/L], 4 had high factor VIII, 1 had high factor XI, and 2 had 4G4G homozygosity (Table 2).
The prevalence of procoagulants in men taking T (5 of 5) was comparable to those not taking T (7 of 8; Table 2).
Discussion
Given the small size of the current study, this should be considered as an exploratory, hypothesis-generating study, recognizing that a multicenter study with many more patients would be more convincing.
In the current study, of the 596 men admitted to the Mercy Hospitals over the past 3 years because of DVT-PE, 110 were now dead, 97 had cancer thought to be a cause of DVT-PE, 250 could not be contacted, leaving 139 men, 7 of whom (1.2% of the total cohort) had taken T prior and at the time of their admissions. The conservative estimate of the prevalence of T use before and at the time of hospitalization for DVT-PE was 1.2% (7 of 596). To the best of our knowledge, this is the first report on the prevalence of DVT-PE requiring hospitalization associated with T therapy in men without previous thrombotic episodes and without any previous diagnosis of thrombophilia–hypofibrinolysis.
In 5 of the 7 men whose DVT-PE necessitated hospitalization, DVT-PE occurred ≤3 months after starting T. The mean and median intervals between initiation of T and hospitalization with DVT-PE were 6.7 and 2 months with a range of 3 weeks to 27 months.
Congruent with our previous reports, where 19 of the 20 patients sustaining DVT-PE or osteonecrosis had familial thrombophilia–hypofibrinolysis, 1,5 all 5 T-taking men with thrombotic events having coagulation measures in the current study were found to have previously undiagnosed thrombophilic-hypofibrinolytic abnormalities, 2 with high factor VIII, 1 with high factor XI, 3 with 4G4G homozygosity of the PAI-1 gene, and 1 with the lupus anticoagulant. The prevalence of procoagulants in the 5 men having DVT-PE on T (5 of 5) was comparable to that (7 of 8) of the 8 controls whose DVT-PE occurred without antecedent T.
Of the many thrombophilias associated with DVT-PE, 18,19 exogenous T use does not appear to “select out” 1 or more unique thrombophilias as shown in the current study, where the pattern of thrombophilias was comparable in cases receiving T and controls not on T. However, we speculate that as exogenous T is aromatized to thrombophilic estradiol, the superimposition of pharmacologic thrombophilia on top of heritable-acquired thrombophilia–hypofibrinolysis facilitates development of DVT-PE and osteonecrosis as in our current and previous reports. 1,5 Congruent with our first 2 reports, 1,5 1 of our 7 patients developed DVT-PE despite warfarin treatment, with an INR maintained in the 2.5 to 3.5 range which preceded and then was concurrent with T before development of DVT-PE.
Endogenous sex hormone levels in men are not associated with risk of venous thromboembolism. 5,20 There are case reports of DVT-PE in men after exogenous T-nandrolone 21 and cerebral sinus thrombosis 22 after exogenous nandrolone.
Given an estimated population prevalence of heterozygosity for the factor V Leiden mutation of 5%, 23 and prevalence of thrombophilias of 18% to 28%, 24 –26,27 there is considerable opportunity for men given T therapy to also have familial and acquired thrombophilias, with resultant DVT-PE and osteonecrosis (ON), as in our current and previous 1,5 reports. Anawalt 28 has noted that “… despite the lessons learned about sex-steroid hormone therapy in postmenopausal women from the Women’s Health Initiative, we are threatened with a reprise of promiscuous prescription of sex-steroid hormone therapy in aging men, obese men, diabetic men, and other groups of men with a high prevalence of low-serum androgen levels,” and has concluded that “… we could scarcely know less about the long-term effects of T therapy on clinically meaningful outcomes in men.” Vitry and Mintzes 29 have expressed similar cautions on wide use of testosterone supplementation in men. In addition to an increase in cardiovascular-related adverse events in elderly men given T supplementation, 30 our initial 1,5 reports and our current study emphasize that DVT-PE and osteonecrosis occur after T therapy in men and women later found to have previously undiagnosed familial thrombophilia–hypofibrinolysis. We recommend that the Food and Drug Administration MedWatch 31 process should be followed in the future for adverse thrombotic events associated with exogenous T to facilitate impact on a national–international level.
The current study has several serious limitations. Because we were able to interview only 25% of the original cohort, our estimate of prevalence of T-associated DVT-PE is very conservative. Sampling far less than the total cohort would have biased our results toward the null, rather than overstated the true prevalence. We included all 597 men admitted over a 3-year period in the denominator in our calculation of prevalence, providing the most conservative estimate of prevalence. This is, to our knowledge, a new finding that could be used in designing a definitive large multicenter study. In fact, the “could not be contacted” and died patient groups may have contained patients who were taking T and experienced morbid or fatal DVT-PE. Thus, some patients having DVT-PE associated with T use might have been missed. Although unlikely, some patients who sustained DVT on T therapy might have been treated in the emergency department without documentation of PE and sent home on anticoagulation.
Previously, we suggested that before exogenous T is given to men 4 or women 32 screening should be carried out for familial and acquired thrombophilia–hypofibrinolysis to avoid the severe thrombotic interactions requiring hospitalization as observed in our current study. Moreover, development of DVT-PE on other drugs that elevate T and estradiol in men might usefully be studied in the future, including Finasteride-Dutasteride, 33,34 human chorion gonadotrophin, 35 and clomiphene citrate. 36,37
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.