
Abstract
Multiple myeloma (MM) is a neoplastic plasma cell disorder characterized by the clonal proliferation of plasma cells in the bone marrow and presence of monoclonal protein in the blood or urine. Diverse hemostatic abnormalities have been reported in patients with myeloma which predispose the patient to bleeding and also thrombosis. The aim of this study was to measure the concentrations of serum levels of vascular endothelial growth factor, D-dimer, and von Willebrand factor in patients with newly diagnosed or relapsed multiple myeloma before treatment, during therapy, and after successful therapy. The working hypothesis was that all of these factors reflect the total body burden of tumor. Angiogenic and coagulation activity should therefore decrease after successful therapy. Our study indicates that selected prothrombotic abnormalities occur in patients with MM, which may contribute to the increased risk of venous thromboembolism observed in these patients. The levels of our 3 parameters were strongly elevated in patient with newly diagnosed MM and also in patients with clinical stage III based on International Staging System criteria. Furthermore, there was a correlation between prognostic disease stages in all study population. It would be appropriate to include angiogenic and coagulation parameters into prognostic parameters.
Introduction
Multiple myeloma (MM) is a plasma cell neoplasm that accounts for 0.8% of cancer cases worldwide and comprises 13% of hematological malignancies. 1 Multiple myeloma is associated with an increased risk of venous thromboembolism (VTE). The cumulative incidence of VTE during the first 6 months from diagnosis of MM has been estimated as 11.1 (95% confidence interval [CI]: 6.0-20.5) per 1000 patients. 2 The risk factors can be patient related (advanced age, history of thrombosis, obesity, immobility, concomitant infections, major illnesses, surgery, and hormone therapy), 3 –6 disease related, and treatment related. Disease-related risk factors can derive from the monoclonal component (rarely hyperviscosity or inhibition of natural anticoagulants) or hypercoagulability sustained by inflammatory cytokines (increased von Willebrand factor [vWf], factor VIII (FVIII), fibrinogen levels, decreased protein S levels, acquired activated protein C resistance). 7 The 1% to 2% baseline of incident VTE associated with conventional therapies as melphalan and prednisone is at least doubled by the use of doxorubicin or other chemotherapeutic agents. Furthermore, the VTE rate associated also with thalidomide or lenalidomide. 8 Multiple myeloma is also a hematological malignancy in which increased angiogenesis rate was detected. 9,10 Angiogenesis activators thought to play a role in MM pathogenesis include vascular endothelial growth factor (VEGF). 11 –13
The aim of this study was to measure the concentrations of serum levels of VEGF, D-dimer, and vWf in patients with MM before treatment, during therapy, and after successful therapy. The working hypothesis was that all of these factors reflect the total body burden of tumor. Angiogenic and coagulation activity should therefore decrease after successful therapy. This could be a suitable additional method for monitoring of disease activity. Moreover, it can also lead to the change in VTE prophylaxis, especially in patients with newly diagnosed MM.
Patients and Methods
The local Ethical Committee of the Jessenius Faculty of Medicine in Martin approved the study. All study participants agreed to participate in the project. Patients were initially examined and tested at the Department of Haematology and Transfusion Medicine in Martin University Hospital. From April 2012 to May 2014, 36 patients (18 men, 18 women; median age: 60.72 years; age range: 40-77 years) with newly diagnosed or relapsed MM were enrolled in this study. The diagnostic criteria of MM were based on the National Comprehensive Cancer Network Clinical Practice Guidelines in Oncology, 2011 Multiple Myeloma Guidelines. Clinical features included age, sex, and bone lesions. Biochemical parameters data were collected including blood count, liver function test, blood chemistry, LDH, β2-microglobulin, urine studies (urea, Bence-Jones proteinuria, and light chains), and protein electrophoresis. Bone marrow trephine biopsy was performed. In addition, patients were grouped into clinical stages according to International Staging System (ISS). The majority of the patients with MM had ISS stage III (n = 20). Patients have received different chemotherapeutic regimens, such CAD (cyclophosphamide, adriamycin, dexamethasone), BP (bendamustine, prednisone), RD (lenalidomide, dexamethasone), VCD (bortezomib, cyclophosphamide, dexamethasone), and VMP (bortezomib, melphalan, prednisone). All patients with relapsed MM received the regimens of RD or BP chemotherapy. Thromboprophylaxis consisting of low-dose molecular weight heparin was given to all patients. Thrombosis has not been reported. Baseline characteristics of the patients are shown in Table 1.
Clinical Characteristics.

Abbreviations: BP, bendamustine and prednisone; CAD, cyclophosphamide, adriamycin, and dexamethasone; Ig, immunoglobulin; RD, lenalidomide and dexamethasone; VCD, bortezomib, cyclophosphamide, and dexamethasone; VMP, bortezomib, melphalan, and prednisone.
Venous blood was collected using a vacutainer system in citrate (0.105 M, Beckton-Dickinson, Plymouth, United Kingdom). This blood was centrifuged at 2000g for 10 minutes. The collected plasma was additionally centrifuged for 10 minutes at 20 000g and stored in small aliquots at −70°C until use. The VWF: Antigen (vWF: Ag) was measured by an in-house sandwich enzyme-linked immunosorbent assay (ELISA) using rabbit antihuman vWF and horseradish peroxidase-conjugated antihuman vWF (Assera, Diagnostica Stago, France). Normal vWf: Ag reference ranges were 0.60 to 1.30 IU/mL. D-dimer levels were determined with a particle-enhanced immunoturbidimetric assay (Innovance, Siemens Healthcare Diagnostics, Germany) according to the manufacturer’s instructions. The reference concentration of D-dimer was less than 0.5 mg/L. The VEGF levels in the plasma were measured using an ELISA kit (Quantikine, R&D systems, Minneapolis, Minnesota) according to the manufacturer’s instructions. Normal ranges of VEGF were 145 ± 75 pg/mL. For each patient, levels of VEGF, vWf, and D-dimer were measured before treatment, during therapy (time when the chemotherapy was given to the patient), and after achievement of complete remission, that is, 1 to 6 months after chemotherapy.
Statistical Package for the Social Sciences (SPSS, Inc, Chicago, Illinois) was used for analysis. Statistical analysis consisted of basic descriptive statistics, and the results are presented as median ± standard deviation. Levels of variables in the different patients’ groups were compared using t test. Odds ratios with 95% CI were used to assess risk. Statistical significance was set at P value <.05.
Results
We measured the concentrations of selected parameters in patients with MM before treatment (vWf1, D-dimer1, and VEGF1), during therapy (vWf2, D-dimer2, and VEGF2) and after successful therapy (vWf3, D-dimer3, and VEGF3). We observed a decrease in vWf, D-dimer, and VEGF levels during the follow-up (mean ± standard deviation [SD] vWf levels: 1.52 ± 0.33 IU/mL; 1.32 ± 0.21 IU/mL; 1.16 ± 0.18 IU/mL; mean ± SD D-dimer levels: 1.02 ± 0.69 mg/L; 0.60 ± 0.33 mg/L; 0.27 ± 0.11 mg/L; mean ± SD VEGF levels: 240.36 ± 123.80 pg/mL; 145.56 ± 53.95 pg/mL; 102.61 ± 45.28 pg/mL); see Figure 1. All selected parameters were reduced back to physiological values.

Comparison between vWf, D-dimer, and VEGF during the follow-up period. VEGF indicates vascular endothelial growth factor; vWf, von Willebrand factor.
We staged the patients according to the ISS criteria. We observed the highest differences in stage III (mean ± SD vWf1 vs vWf3 levels: 1.64 ± 0.26 IU/mL vs 1.18 ± 0.19 IU/mL; mean ± SD D-dimer1 vs D-dimer3 levels: 1.3 ± 0.71 mg/L vs 0.30 ± 0.13 mg/L; mean ± SD VEGF1 vs VEGF3 levels: 298.3 ± 120.39 pg/mL vs 104.75 ± 45.64 pg/mL). These results are summarized in Table 2.
Results of Selected Parameters Before, During, and After Treatment Grouped Into Clinical Stages According to ISS.

Abbreviations: ISS, International Staging System; VEGF, vascular endothelial growth factor; vWf, von Willebrand factor.
We had done the t test to see if there are statistical differences between the means of selected parameters divided into 2 groups according to the blood sampling (before and after chemotherapy) (vWf1 vs vWf3: 95% CI: 0.25-0.48; P = .000; D-dimer1 vs D-dimer3: 95% CI: 0.53-0.98; P = .000; VEGF1 vs VEGF3: 95% CI: 95.74-179.76; P = .000). In all cases, we see the statistical significance. Moreovere, we stratified the patients according to ISS stages. After analyzing, we see again a significant difference between various ISS stages, expect for ISS I. More details are given in Table 3.
Statistical Comparisons Between Selected Parameters Before and After Treatment Group Into Clinical Stages According to ISS.

Abbreviations: ISS, International Staging System; VEGF, vascular endothelial growth factor; vWf, von Willebrand factor.
We also evaluated the parameters in both newly diagnosed and relapsed patients with MM. At the time of diagnosis, we can see that angiogenic and coagulation activity is more altered in patients with newly diagnosed MM (mean ± SD newly vWf1 vs relapsed vWf1: 1.61 ± 0.32 IU/mL vs 1.24 ± 0.24 IU/mL; mean ± SD newly D-dimer1 vs relapsed D-dimers1: 1.15 ± 0.16 mg/L vs 0.96 ± 0.92 mg/L; mean ± SD newly VEGF1 vs relapsed VEGF1: 247.25 ± 128.11 pg/mL vs 216.25 ± 80.21 pg/mL). All parameters were reduced back to physiological values. We also observed a decrease in vWf, D-dimer, and VEGF levels in both groups during the follow-up, see Table 4.
Results of Selected Parameters Before, During and After Treatment in Patients With Newly Diagnosed or Relapsed MM.
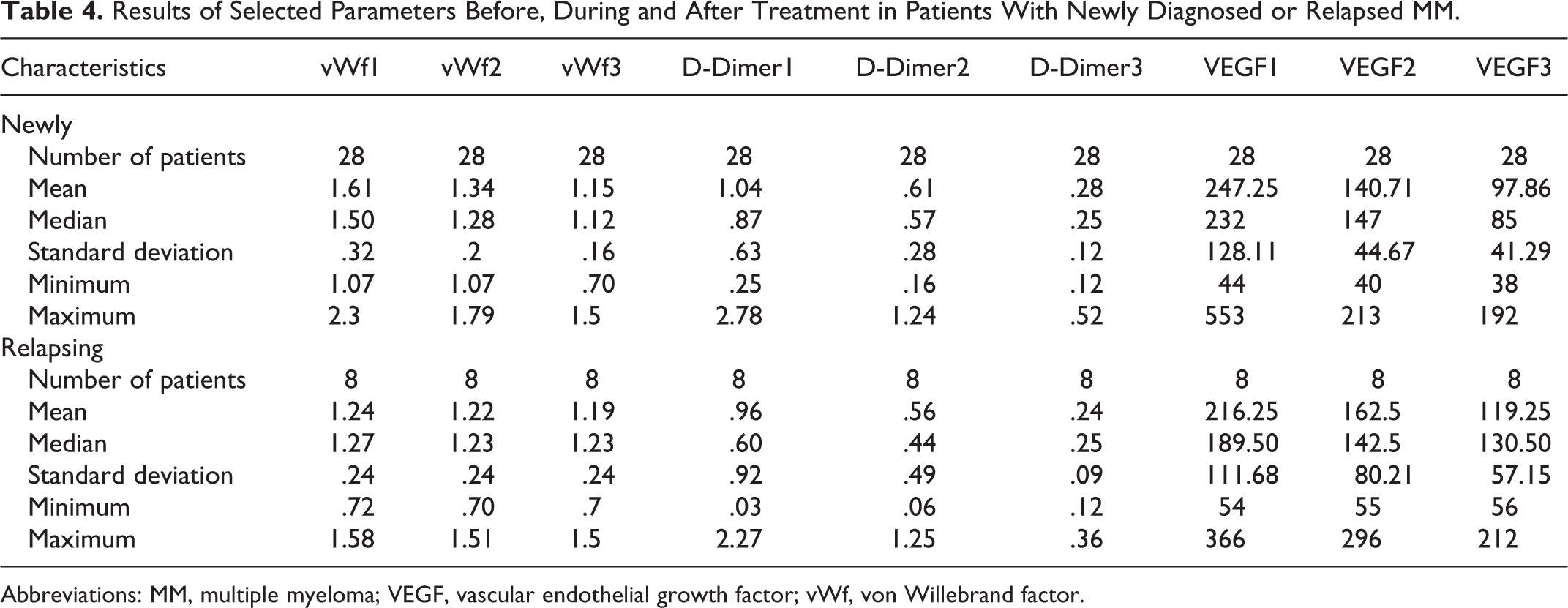
Abbreviations: MM, multiple myeloma; VEGF, vascular endothelial growth factor; vWf, von Willebrand factor.
Discussion
Patients with MM are more prone to VTE because of patient-related, disease-related, and treatment-related risk factors. The mechanisms involved in the development of thrombosis in MM are complex and remain poorly understood. The first report on altered coagulation factors in patients with MM dates back to 1976 and concerned an observed increase in FVIII levels. 14 High levels of FVIII and vWF have been reported by Minnema et al in patients with MM, which may contribute to the increased risk of thrombosis. 15 Also, it has been postulated that acquired resistance to protein C, which was observed in up to 23% of patients with MM, may be associated with the increased VTE risk. 16 In addition, several cytokines and transcription factors are elevated in patients with MM, such as interleukin-6 (IL-6), tumor necrosis factor-α (TNF-α), VEGF, and nuclear factor κB. 17 In particular, IL-6 and TNF-α promote hemostasis through several pathways, with upregulation of tissue factor, fibrinogen, and FVIII. 18,19 All in all, in patients with MM occurs hypercoagulability, as shown by higher levels of endogenous thrombin potential in a global assay of thrombin generation. 20 Another index of overall hypercoagulability as D-dimer was reported to be increased. 21,22
We had chosen vWf, D-dimer, and VEGF because we expected that they will be elevated before treatment starts. In our study, we worked with hypothesis that all of these factors reflect the total body burden of tumor and levels of these parameters should fall during the treatment. Therefore, we took a blood sample at the time of diagnosis, during therapy, and after achieving complete remission. As we expected, all levels were abnormal at the beginning of the study. In addition, we found a significant correlation between prognostic stage according ISS criteria. In other words, this could mean that patients with stage III have the highest risk of VTE. This could help to explain while 2 prospective randomized trials from GIMEMA (Grupo Italiano Malattie Ematologiche dell´Adulto) did not find a statistically significant difference between different types of antithrombotic prophylaxis. 23,24 During follow-up we observed that all selected parameters were reduced back to physiological values. Decrease in the levels were statistically significant, except stage I. This is consistent with our hypothesis (bigger tumor mass greater alteration of angiogenic and coagulation activity).
Furthermore, we found a correlation between patients with newly diagnosed and relapsed MM. Patients with newly diagnosed MM had more elevated parameters. This reflect the fact that patient with newly diagnosed MM have more altered angiogenic and coagulation activity. It can also explain the data from different studies in which the patients with relapsed/refractory MM had a lower risk of VTE compare to patients with newly diagnosed MM. 25,26
There were several limitations in our study, including the limited number of patients and a bias in patient selection (one center experience).
Conclusions
Our study indicates that selected prothrombotic abnormalities occur in patients with MM, which may contribute to the increased the risk of VTE observed in these patients. The levels of our 3 parameters were significantly higher in patient with newly diagnosed versus relapsed MM and also in patients with clinical stage III based on ISS criteria versus patients with stage I or II. Furthermore, there was a strong correlation between prognostic disease stages according to ISS criteria in all patients (newly diagnosed or relapsed MM) during the follow-up period. It would be appropriate to include angiogenic and coagulation parameters into prognostic parameters.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by grants VEGA 1/0187/17 and APVV-17-0054.