
Abstract
Vitamin K-dependent clotting factors are commonly divided into prohemorrhagic (FII, FVII, FIX, and FX) and antithrombotic (protein C and protein S). Furthermore, another protein (protein Z) does not seem strictly correlated with blood clotting. As a consequence of this assumption, vitamin K-dependent defects were considered as hemorrhagic or thrombotic disorders. Recent clinical observations, and especially, recent advances in molecular biology investigations, have demonstrated that this was incorrect. In 2009, it was demonstrated that the mutation Arg338Leu in exon 8 of FIX was associated with the appearance of a thrombophilic state and venous thrombosis. The defect was characterized by a 10-fold increased activity in FIX activity, while FIX antigen was only slightly increased (FIX Padua). On the other hand, it was noted on clinical grounds that the thrombosis, mainly venous, was present in about 2% to 3% of patients with FVII deficiency. It was subsequently demonstrated that 2 mutations in FVII, namely, Arg304Gln and Ala294Val, were particularly affected. Both these mutations are type 2 defects, namely, they show low activity but normal or near-normal FVII antigen. More recently, in 2011-2012, it was noted that prothrombin defects due to mutations of Arg596 to Leu, Gln, or Trp in exon 15 cause the appearance of a dysprothrombinemia that shows no bleeding tendency but instead a prothrombotic state with venous thrombosis. On the contrary, no abnormality of protein C or protein S has been shown to be associated with bleeding rather than with thrombosis. These studies have considerably widened the spectrum and significance of blood coagulation studies.
Any given clotting factor or protein is commonly associated with either bleeding or thrombosis. The only known exception to this rule was fibrinogen, which in one of its defects, dyfibrinogemia or hypodysfibrinogemia, demonstrated to cause both bleeding and thrombosis. 1 –4 Recent studies have discovered that other clotting proteins or factors could present a similar bivalent behavior. The clotting factors involved are FII, FVII, and FIX. 5 –9 These are all vitamin K-dependent and are usually associated with a variable bleeding tendency. For 2 of these factors, FII and FIX, the association with thrombosis, besides the clinical observation, has been demonstrated by molecular studies. 5,8 For the third factor, FVII, the demonstration is still based only on clinical and FVII antigen evaluation. 7,10 –12 The purpose of the present article is to analyze these new findings that have considerably complicated the diagnosis of clotting defects but greatly increased our knowledge of blood clotting.
Classification
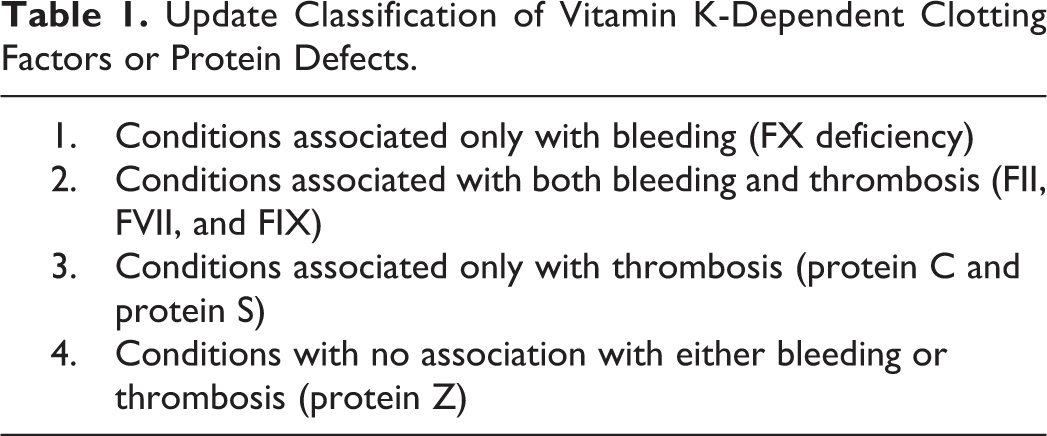
Vitamin K-dependent coagulation proteins should be divided today into (1) conditions associated only with bleeding (FX); (2) those associated with both bleeding and thrombosis (FII, FVII, and FIX); (3) those associated only with thrombosis, (protein C and protein S); and, finally, (4) those probably associated with neither bleeding nor thrombosis (protein Z9; Table 1).
Update Classification of Vitamin K-Dependent Clotting Factors or Protein Defects.
Conditions Associated Only With Bleeding
Only FX deficiency remains in this category. The condition was first described in 1956 to 1957 by British, Swiss, and American research. 13 During the past 60 years, several cases have been reported all over the world. However, the defect is still to be considered one of the rarest so far discovered. A prevalence of 1:1 000 000 or 1:1 500 000 has been postulated. About 150 mutations have been discovered, mainly missense mutations. The defect, at the homozygous or the compound heterozygous level, is always symptomatic. Bleeding tendency may be severe with brain hemorrhage, hemarthrosis, and deep hematomas. Two types of defects are present, namely, type 1 in which there is a parallel decrease in FX activity and FX antigen and type 2 in which FX activity is low but FX antigen is normal or near normal. Laboratory diagnosis is based on a prolongation of both activated partial thromboplastin time (aPTT) and prothrombin time (PT) corrected by the addition of normal plasma or serum. Type 2 forms show a different reactivity toward different activating agents (cephalin, tissue factor, or Russell Viper Venom [RVV]). Therefore, a correct clotting diagnosis has to include an exploration of all systems (intrinsic by cephalin and extrinsic by tissue factor and RVV-dependent by RVV clotting time). The paradigmatic example of these discrepancies is represented by FX Friuli (Arg343Gln), which shows a prolonged aPTT and PT but a normal RVV clotting time. 9,14,15
Condition Associated With Both Bleeding and Thrombosis
The vitamin K-dependent coagulation factors that belong to this group are FII (prothrombin), FVII (proconventin), and FIX (antihemophilic factor B). (1) Prothrombin defects
Congenital prothrombin deficiency is one of the rarest coagulation disorders. 10,16 Homozygotes or compound heterozygotes with FII levels <10% of normal present a severe bleeding tendency. Complete absence of prothrombin seems incompatible with life. 10,16 Heterozygotes with FII levels around 40% to 60% of normal may present occasional bleeding during surgery or tooth extractions. 17 No thrombotic event has ever been reported in “true” prothrombin deficiency. 10 Recently, a few cases of prothrombin abnormalities have been associated with a thrombotic tendency. 5,18 –21
Antithrombin (AT) is a small glycoprotein with a molecular weight of 58 000 Dalton produced by the liver and circulating at a concentration of about 0.12 mg/mL. When coupled with heparin, it exerts mainly an anti-FII and anti-FX activity. Without heparin, the activity of AT is markedly reduced. The increased resistance of these abnormal prothrombins to the action of AT creates a condition of prolonged thrombin activity which may cause thrombosis. The condition has been termed “antithrombin resistance.” 5
This is a new clinical entity characterized by a relative decrease in AT activity due to the presence of abnormally resistant prothrombins (thrombins) which have mutations in a special region of the molecule, encoded by exon 12, that is supposed to interact with AT. Due to these mutations, the generation of the complex thrombin–antithrombin is defective, whereby AT activity is decreased, thrombin persists in the circulation, and a thrombophilic state ensues. 5,18 –21
The first prothrombin abnormality responsible for this effect was reported in 2012 (Prothrombin Yukuhashi). 5 Subsequently other similar cases were published in Serbia, India, and Italy. 16 –19 The 5 families involve 3 different mutations on the same amino acid, an Arginine: Prothrombin Yukuhashi, Arg596Leu 5 ; Prothrombin Belgrade, Arg596Gln 18 ; and Prothrombin Padua 2, Arg596Trp 19 (Table 2).
Cases of Dysprothrombinemias due to Arg596 Mutations Associated With a Gain in Function Toward Antithrombin With Consequent Appearance of a Thrombophilic State.a
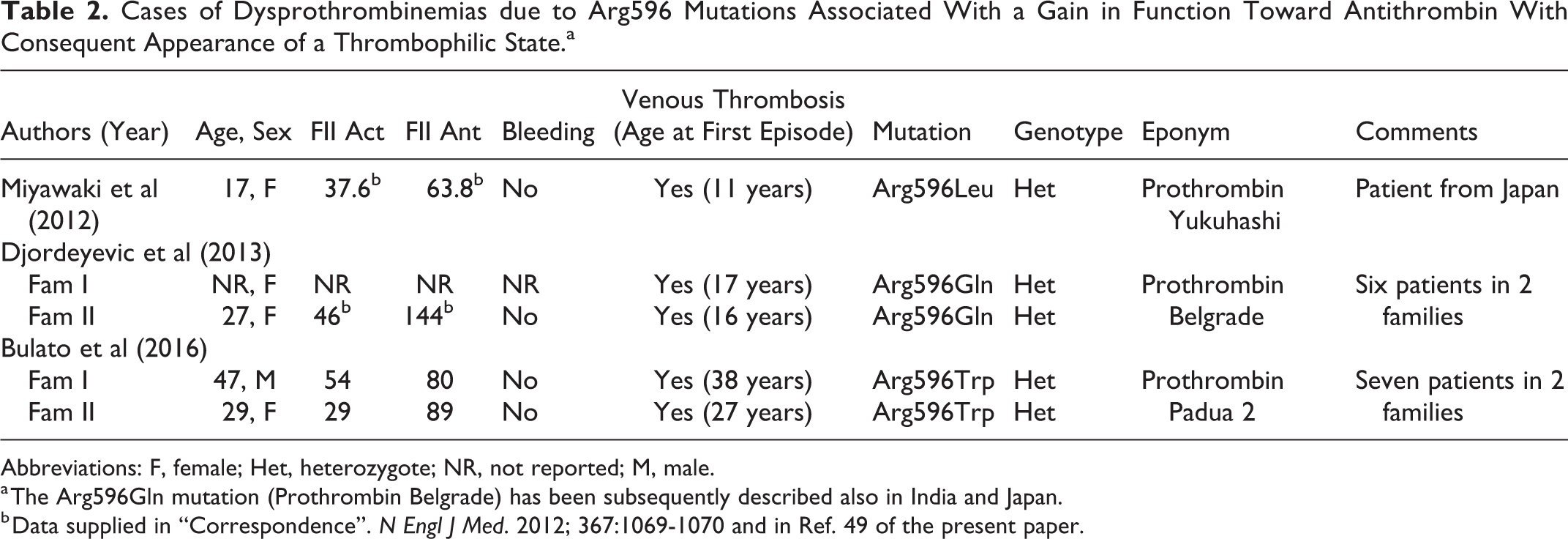
Abbreviations: F, female; Het, heterozygote; NR, not reported; M, male.
a The Arg596Gln mutation (Prothrombin Belgrade) has been subsequently described also in India and Japan.
b Data supplied in “Correspondence”. N Engl J Med. 2012; 367:1069-1070 and in Ref. 49 of the present paper.
Another prothrombin abnormality seen in Japan is identical to Prothrombin Belgrade, namely, Arg596Gln. 20 The main feature of these dysprothrombinemias is the occurrence of thrombosis at a young age. Prothrombin Amrita has always an Arg596Gln mutation, but in this case, venous thrombosis occurred at the age of 60. 21 Furthermore, there is no family history for thrombosis. It is still unknown at what level of the codon sequence a mutation can cause the shifting of a bleeding condition into a thrombophilic one. Prothrombin Greenville shows an Arg517Gln mutation and a mild bleeding tendency but no thrombosis. 22 It is interesting to note that all these patients are heterozygotes for the mutation. This indirectly confirms the fact that homozygosis for prothrombin defects are very severe and sometimes incompatible with life. 16,17
The main laboratory and clinical features of the 3 dysprothrombinemias due to the mutation of Arg596 are gathered in Table 1. All patients had venous thrombosis; there is no information about arterial thrombosis. It is likely that other cases will be discovered. A clinical suspicion should arise from the following observations: (1) venous thrombosis in a young patient with no other known prothrombotic defect (AT and protein C deficiencies and so on); (2) slightly decreased or borderline low prothrombin activity level; (3) prothrombin antigen level higher than the activity counterpart; (4) and positive family history for venous thrombosis. 5,18,19 Needless to say that genetic analysis is needed to confirm the suspicion.
The occurrence of thrombosis at a young age is of paramount importance. The mean age, excluding the case from India, is 20.1 (range 11-38). It is worth noting that so far, no abnormality of FX has been described which could generate an impairment in the activity of AT with a consequent AT resistance. On theoretical grounds, the possibility that such mutation in the FX gene exist is fully plausible and even likely.
For the sake of completion, it should be mentioned, dealing with prothrombin, that the polymorphism G to A 20210 of the untranslated region of the gene has been associated with slightly increased levels of this clotting factor and an increased incidence of venom thrombosis.
6
The thrombotic events occur mostly in patients who present other concomitant risk factors. (2) FVII Defects
FVII defects are also subdivided into type 1 and type 2. Bleeding tendency is variable and not always strictly related to the FVII activity level. 7 Heterozygotes do not bleed. 23 Patients with type 2 defects seem to have, often, only a mild bleeding tendency. These are the patients who sometimes present thrombotic events. The mutations frequently involved with thrombotic events are Arg304Gln (FVII Padua) and Ala294Val. These are both type 2 defects. 11
According to some authors, about 3% of patients with FVII deficiency have thrombotic manifestations. 7 Venous thromboses prevail, and this seems in contrast to FXI deficiency, where venous thrombosis is rare. 24
It has also been demonstrated that the majority of patients with FVII deficiency and thrombosis have concomitant triggering events such as immobilization, replacement therapy especially that with aFVII concentrates, oral contraceptives, surgical procedures, and pregnancy.
12,25,26
(3) FIX Defects
FIX deficiency is responsible for hemophilia B. This is a sex-linked severe bleeding disorder. The defect is also subdivided into type 1 and type 2. The FIX Padua abnormality is due to the hemizygous mutation Arg338Leu in exon 8. 8 The propositus has highly elevated FIX activity, while the FIX antigen is only mildly increased. There is no bleeding diathesis but a venous thrombosis. A brother is similarly affected but asymptomatic. The mother is a carrier and asymptomatic.
The clinical significance of this mutation in the pathogenesis of inherited thrombosis is limited, since the abnormality seems rare. 27,28 It has instead a great scientific impact, since it demonstrates, as it is true for the dysprothrombinemias, that a clotting factor, depending on the site of the mutation, may cause either bleeding or thrombosis. 29
There are other FIX variants due to several mutations, FIX BM and FIX Leiden, but these variants are not associated with thrombophilia. 30,31 Hemophilia BM is a variant of Hemophilia B+ that is associated with a slight prolongation of the PT. The prolongation is particularly evident when an ox-brain tissue thromboplastin is used in the assay system. 30
The finding is due to an inhibitor effect exercised by the abnormal FIX on the Tissue Factor + FVII complex. Hemophilia BM has to be considered a special forma or variant of Hemophilia B+ (type 2). Hemophilia B+ does not show the inhibitor activity. Hemophilia B Leiden is characterized by an increase in FIX activity as the age of the patient increases. 31 In these 2 FIX variants, no thrombosis has ever been described.
Conditions Associated Only With Thrombosis
Protein C is another vitamin K-dependent clotting protein. Its absence or abnormality is associated with the appearance of a hypercoagulable or thrombophilic state. Once activated by thrombin, PC inhibits or downregulates aFVIII and aFV, therefore regulating the homeostatic balance. Protein S acts a cofactor in aPC function. 32,33
Deficiency or abnormalities of protein C or protein S are associated with a thrombophilic state and thrombosis, mainly venous. No genetic abnormality of either protein C or protein S gene has shown reversal of its biological action, which is anticoagulant.
Conditions not Associated With Bleeding and Thrombosis: Protein Z Deficiency Belongs to This Group
Protein Z deficiency
Protein Z deficiency should also be mentioned here, since a few sporadic observations or articles have suggested but not proven the possibility that this factor plays a role in blood coagulation. 9
Protein Z is a 62 000-Da, single-chain, vitamin K-dependent glycoprotein.
It is synthesized in the liver under the coding of a gene located at chromosome 13q34, close to the genes encoding for FVII and FX. It has 8 exons and a structure similar to those encoding for other prothrombin complex (PC) factors. 34
The possibility that protein Z might be involved in bleeding diathesis arose from the observations of decreased protein Z levels in patients with a variable bleeding tendency but without other clotting defects that the diathesis could be attributed to. 35,36
Other studies have not confirmed the findings and shown a great variability in protein Z levels even in the normal population. 37 Furthermore, it is interesting to know that no family has been described, where both homozygotes (severe deficiency) and heterozygotes (mild deficiency) were present with an established hereditary pattern. Isolated cases with a severe deficiency have also never been reported.
For example, recent studies on the protein Z-dependent protease inhibition might clarify the pattern. In fact, since the activity of this inhibitor seems directed toward FXa, this could supply some support to a bleeding role of this protein, at least an indirect one. 33
Protein Z has also been suggested to play both a prothrombotic and/or a protective role in patients with other thrombotic conditions (FV Leiden) based on association studies. However, even in this area, results are not univocal and therefore do not seem conclusive. 33 No thrombosis has even been described in patients with decreased protein Z levels. Therefore, protein Z is still a clinically functional orphan glycoprotein. Needless to say, future studies might clarify the pattern.
Discussion
Prothrombin, FVII, FIX, protein C, and protein S are vitamin K-dependent clotting factors or proteins strictly related to blood coagulation. The ties of another protein, protein Z with blood coagulation, is less evident or still poorly defined.
Prothrombin abnormalities due to Arg596 substitution have been reported so far to be associated with venous thrombosis. 5,18,19 The same is true for the FIX Arg338Leu mutation. 8 Disregarding for the present time, protein Z, it is astonishing to see that both coagulant and anticoagulant proteins are dependent on the vitamin K system.
This is one of the most important homeostatic systems in blood coagulation. There is no other similar system in blood coagulation. The phylogenetic significance of it is unknown. Did the procoagulant factors appear first as a defense from bleeding, and the antithrombotic components appear later as a defense from thrombosis? In FII and FIX defects, no arterial thrombosis has ever been reported. On the contrary, in FVII deficiency, both venous and arterial thromboses have been reported although the majority of events involve the venous system. 12,25 It is still unknown whether this discrepancy is due to the rarity of the Arg596 dysprothrombinemias and of the Arg338Leu FIX mutations or if it has a specific significance.
In both these instances, concerning FII or FIX, an Arg residue is the substitution involved. The mutations associated with venous thrombosis in FVII deficiency are mostly Ala294Val and Arg304Gln 11 These are both type 2 disorders with low activity but normal or near-normal antigen. However, the correlation between mutation and thrombosis in this case is not so strict as that observed for FII and FIX. In fact, venous thrombosis has also been seen, although rarely, in patients with other mutations. 11
In sharp contrast with this ambivalent behavior of FII, FVII, and FIX, no data are available on a similar behavior for protein C or protein S. There is no available report that mutations in these 2 antithrombotic proteins might turn them into prohemorrhagic entities. Can this be excluded? Obviously not. The same was true for prothrombin before the first case of Arg596Gln. Mutation was discovered in 2012. 5
It is worth noting that there is no direct relation between Vitamin K-dependent coagulation proteins. Protein C and protein S play no direct role in contrasting the clotting activity of FII, FVII, or FIX. Once activated by thrombin, their inhibitory activity is against aFV and aFVIII, thereby downregulating blood coagulation. This represents a link between the Vitamin K-dependent clotting proteins and the FVIII and FV system.
Due to the structural similarities existing between FV and FVIII, it is no surprise that a protein C with the help of protein S may inhibit or downregulate both of them. There are also useful clinical and laboratory implications involved. The occurrence of venous thrombosis at a young age is important. Similarly, important is the observation that venous thrombosis may be present in a family in association with decreased prothrombin activity as seen in dysprothrombinemias. 38
The ambivalence of FII and FIX and, to a lesser degree, that of FVII have considerably widened the spectrum of congenital clotting defects. It remains now to be seen whether other clotting factors, for example, FX and Protein Z, might show similar features. The sol to gel transformation of blood is still, after so many years, a material for study. These studies on the prothrombin complex have further shown the complexity of the relation existing among clotting factors. The prothrombin complex could be envisaged as one of the homeostatic mechanisms in blood coagulation.
Footnotes
Authors’ Note
The study was performed according to the Helsinki convention and its ethical standards. No grant number, (only secretarial support). This article does not contain any study with human participants performed by any of the authors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported in part by the “Associazione Emofilia ed altre coagulopatie delle Tre Venezie”.