
Abstract
Adherence to non-vitamin K antagonist oral anticoagulants (NOACs) is an important factor for ensuring efficacy and safety in nonvalvular atrial fibrillation (NVAF). There are controversial results regarding NOAC adherence in real-world data and there are no data about NOAC adherence in Turkish population. This study investigated the NOAC adherence based on self-report, factors affecting nonadherence, and the relation of the adherence level with efficacy and safety outcomes. This multicenter cross-sectional study included 2738 patients (59% female) using NOAC (dabigatran, apixaban, and rivaroxaban) due to NVAF for more than 3 months with >30 days of supply between September 1, 2015, and February 28, 2016. To measure the adherence level, an 8-item Morisky Medication Adherence Scale was used. The mean age of the patients was 70 ± 10 years. Of the 2738 patients, 44% were receiving dabigatran, 38% rivaroxaban, and 18% apixaban. A total of 630 (23%) patients had high medication adherence, 712 (26%) moderate adherence, and 1396 (51%) low adherence. Nonadherence had related to stroke (5.6% vs 2.5%, P < .001) and minor (21.2% vs 11.1%, P < .001) and major (6.1% vs 3.7%, P = .004) bleeding rates. The adherence to NOAC was found to be quite low in Turkey. Nonadherence is associated with bleeding and thromboembolic cardiovascular events. Age, taking NOAC twice a day, and the additional noncardiac diseases, depression, and dementia were the independent factors affecting poor medication adherence.
Introduction
Atrial fibrillation (AF) is the most common type of cardiac arrhythmia encountered in clinical practice. Atrial fibrillation can result in death, stroke, heart failure, a decrease in exercise capacity, left ventricular dysfunction, and a decrease in quality of life. 1
To date, vitamin K antagonists (VKAs) have been the oldest and most commonly used anticoagulant drugs in the treatment of AF. Although VKAs are efficient drugs in the prevention and treatment of thromboembolic disorders, they have several disadvantages including a narrow therapeutic index, delayed onset and offset of action, and interaction with diet and other drugs. 2 Because of these reasons, the patients using VKA should be monitored frequently and followed up closely to keep them in the time in therapeutic range (TTR). Non-vitamin K antagonist oral anticoagulants (NOACs) are current anticoagulant drugs which were developed in order to overcome these disadvantages of VKAs and whose efficacy and safety were proven in randomized controlled trials in patients with nonvalvular AF (NVAF). 3 –7
Rapid onset of action, stable fixed-dose combination, and the absence of the need for monitoring are their main advantages of NOACs over VKAs. 8,9 Because of these features of NOACs, the frequency of outpatient follow-up visits is lower. Due to their short half-life, the efficacy of NOACs may disappear quickly if the dose is missed. 2 Hence, medication adherence is particularly important for NOACs. Even though patient compliance was found to be high in phase III trials, it is difficult to compare with real-world data due to selective inclusion and close follow-up of patients during trial by researchers. The real-world data about adherence to NOACs are controversial, and adherence rates vary by population. There is no previous study about adherence to NOACs in Turkish population. The studies on the use of VKA in patients from Turkey showed a quite low TTR rate (49.52%). 10 According to the regulations of the social insurance institution in Turkey, almost all patients with NVAF receiving NOAC have previously used VKA; for this reason, the assessment of adherence to NOAC treatment becomes even more important.
In this study, we evaluated the level of medication adherence of a Turkish population with NVAF receiving NOACs by using an 8-item Morisky Adherence Scale. We also investigated the risk factors for nonadherence and the relation between nonadherence to NOACs with effectiveness (thromboembolic event) and safety (bleeding) outcomes.
Material and Methods
This multicenter cross-sectional study was conducted between September 2015 and February 2016 in 45 centers encompassing all the geographical regions of Turkey. According to Republic of Turkey Ministry of Health and Social Security Institution, the conditions for the reimbursement of NOAC treatment have been determined as inadequate TTR or cardioembolic event during VKA treatment; therefore, the study population consisted of patients who had previously received VKA. The study included patients older than 18 years, who were followed up in cardiology clinics, and who received dabigatran (110-150 mg), rivaroxaban (15-20 mg), or apixaban (2.5-5 mg) for the last 3 months with >30 days of supply due to NVAF. This study was approved by the research ethics committee of the city of Afyonkarahisar (decision number 2015/340) and registered at ClinicalTrials.gov (identifier NCT02480920). Written informed consent was obtained from all patients. Patients with valvular AF, deep vein thrombosis, and pulmonary embolism were not evaluated. A total of 3150 patients were evaluated in this study. The 163 patients with a sociocultural level inadequate to fill the questionnaire and the 249 patients who received new oral anticoagulant for less than 3 months were excluded from the study. This study was conducted with the remaining 2738 patients. All enrolled patients responded to the questionnaire form including demographic features, currently used oral anticoagulant, previously used drugs, and cardiovascular and noncardiac comorbidities. Furthermore, medical history and hospital records were reviewed to investigate adverse effects, stroke, and any bleeding complication during NOAC treatment. Major bleeding was defined as a hemorrhage leading to a reduction in hemoglobin concentration of 2 g/dL, necessitating the transfusion of 2 or more units of blood, or symptomatic bleeding into a critical area or organ. All other bleedings were considered as minor.
Congestive heart failure/left ventricular dysfunction, Hypertension, Age ≥75 years (doubled), Diabetes, Stroke (doubled)–Vascular disease, 65-74 years of Age, and Sex category (female) [CHA2DS2-VASc] score and Hypertension, Abnormal renal/liver function, Stroke, Bleeding history or predisposition, Labile INR, Elderly (eg, age: 65, frailty, etc), Drugs/alcohol concomitantly [HAS-BLED] score were calculated for all patients with NVAF. At the last part of the questionnaire, the 8-item Morisky Adherence Scale questions were posed.
Morisky Adherence Scale
The validity of the Morisky Adherence Scale had already been demonstrated with regard to medication adherence in patients receiving VKA. 11 An extended 8-item Morisky scale was used instead of the original 4-item Morisky scale in order to better identify the situations and the conditions that could affect medication adherence and to better assess the psychometric features (Table 1). 12 The reliability and the validity of the 8-item Morisky Adherence Scale translated into Turkish had been demonstrated in Turkish population by previous studies. 13,14
Morisky 8-Item Medication Adherence Questionnaire.a
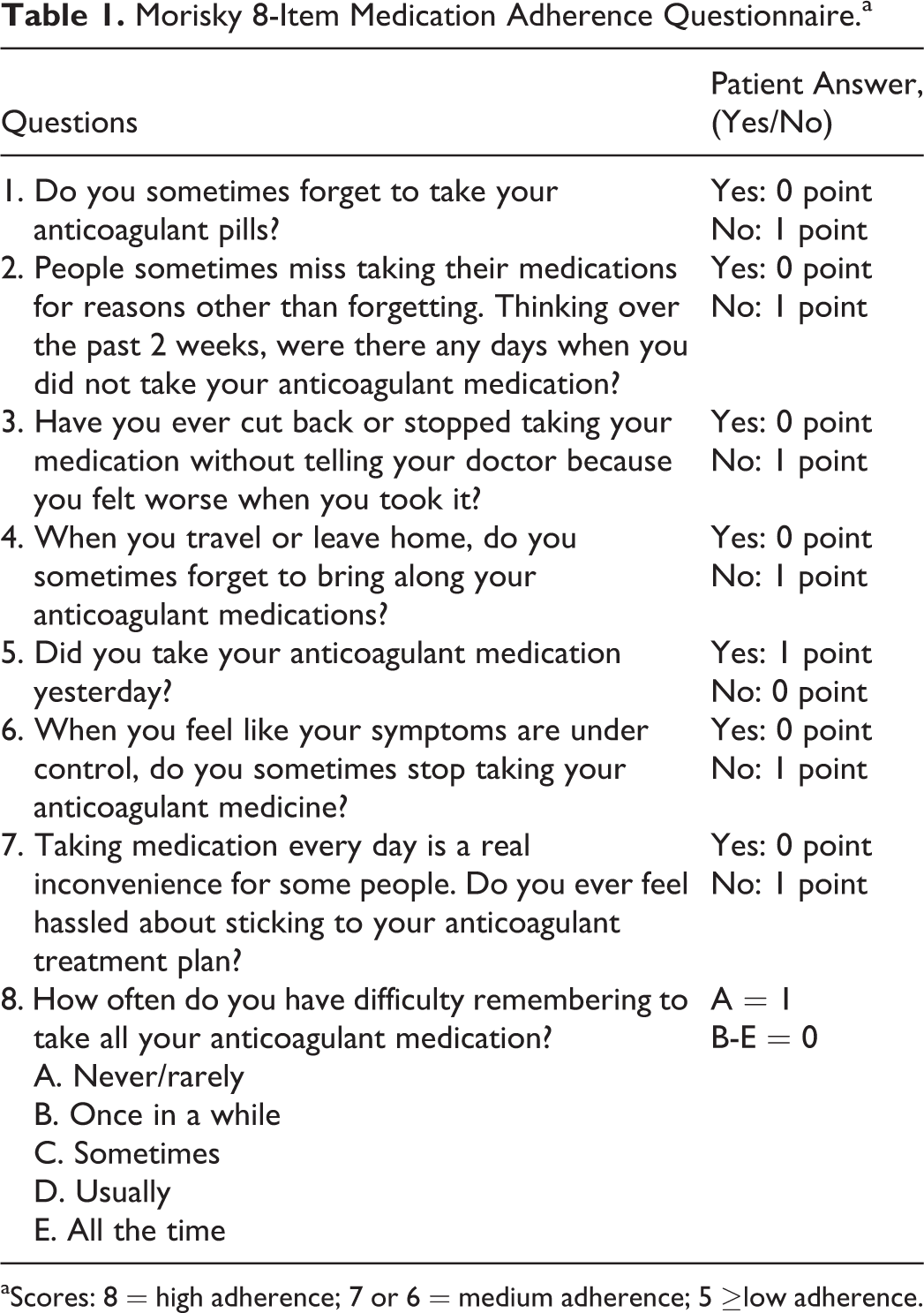
aScores: 8 = high adherence; 7 or 6 = medium adherence; 5 ≥low adherence.
In this scale, each question answered by the patient was scored as 0 or 1 according to a “yes” or “no” answer, respectively. Accordingly, a total score of maximum 8 and minimum 0 point could be calculated per the answers of the patient. In the 8-item Morisky scale, 8 points was considered as high adherence, 6 to 7 points as medium adherence, and 5 points or less as low adherence. In order to identify the independent predictive variables that could affect the medication adherence of the patients with logistic regression analysis, the patients were categorized into 2 groups as adherent patients who had high and medium adherence (Morisky score 6 or more) and nonadherent patients who had low adherence (Morisky score 5 or less). 12
Statistical Analysis
SPSS version 15.0 for Windows (SPSS Inc, Chicago, Illinois) software program was utilized for the analyses of the study. Mean and standard deviation were used to present numerical data, while frequency and ratio were used for categorical data. To compare numerical data between the patient groups, independent t test was performed for 2 groups and 1-way analysis of variance test for 3 groups, whereas χ2 test was used for categorical data. The factors found to be associated with medication adherence in univariate analysis (P < .20) were evaluated with multivariate logistic regression analysis. Odds ratio (OR) and 95% confidence interval (CI) were estimated with standard methods. The limit of statistical significance (type I error) was considered as P < .05 in all analyses.
Results
The mean age of the patients was 70 ± 10 years, the median being 71 years (range: 23-97 years). The number of the female patients was more (1623, 59%). All patients had previously received VKA treatment and were later switched to NOAC treatment. Patients were switched to NOACs because 25% had previous minor and major bleeding, 7% had previous thrombosis, and 92% had also poor TTR. A total of 44% dabigatran, 38% rivaroxaban, and 18% apixaban users were identified. All patients received NOAC at least 90 days, and the average duration of NOAC use was 360 ± 230 days. The patients were predominantly illiterate or primary school graduate (78%). Fifty-two percent of the patients was unemployed and a great majority (69%) was living in other provinces. Almost all patients (99%) were receiving 1 or more additional drugs. The demographic characteristics of the patients are shown in Table 2.
Baseline Characteristics of Patients.
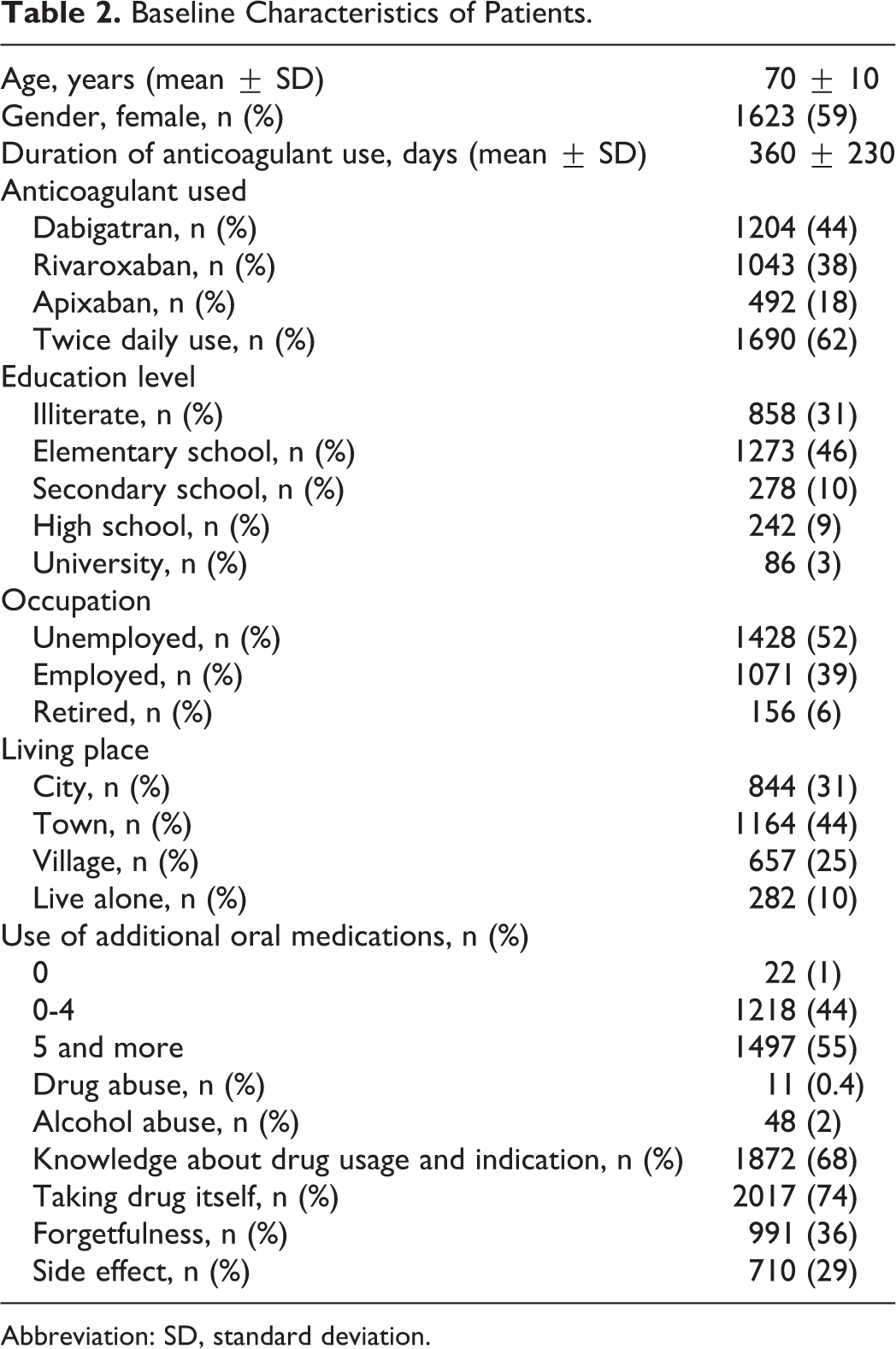
Abbreviation: SD, standard deviation.
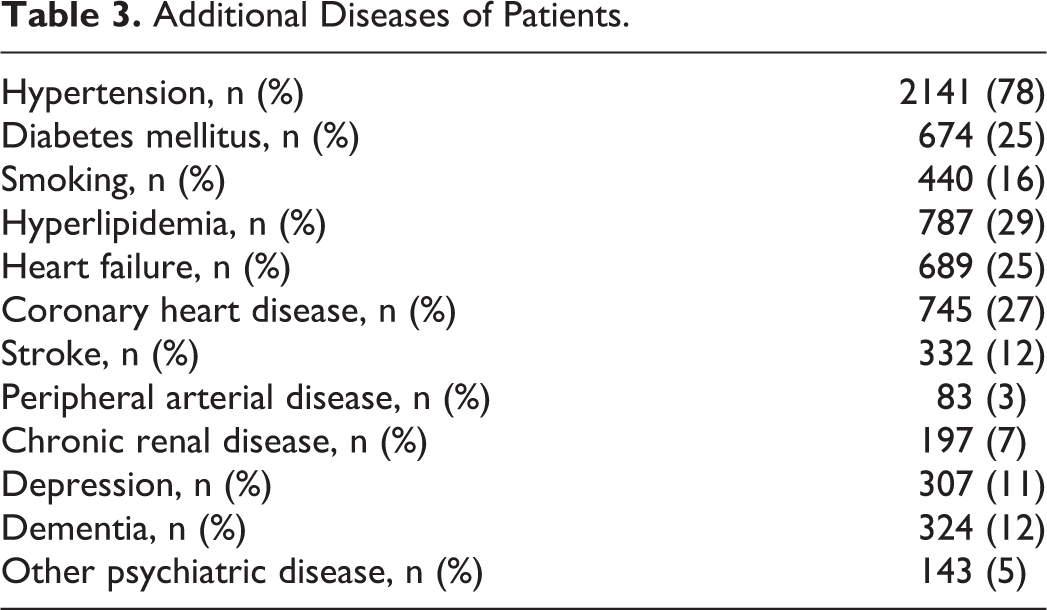
The frequencies of cardiovascular risk factors and diseases were found to be high. The mean CHA2DS2-VASc score was 3.5 ± 1.4. The mean CHA2DS2-VASc score in patients receiving dabigatran, apixaban, and rivaroxaban was 3.5 ± 1.4, 3.5 ± 1.4, and 3.5 ± 1.3, respectively. There was no significant difference between the groups (P = .940). The clinical features of the patients are shown in Table 3.
Additional Diseases of Patients.
Of the patients, 630 (23%) had high medication adherence, 712 (26%) moderate adherence, and 1396 (51%) low adherence. In logistic regression analysis, those with high and moderate medication adherence were grouped as adherent. Independent risk factors affecting poor medication adherence were advanced age (≥65 years, OR: 1.57, 95% CI: 1.27-1.94; P < .001), use of 5 or more drugs (OR: 1.46; 95% CI: 1.23-1.73; P < .001), taking the dose twice a day (OR: 1.32; 95% CI: 1.11-1.57; P = .001), higher education (OR: 0.41, 95% CI: 0.22-0.66; P = .005), being informed about the drug (OR: 0.50; 95% CI: 0.41-0.61; P < .001), living in a village (OR: 1.46; 95% CI: 1.16-1.84; P = .001), administration of the drug by someone else (OR: 1.51; 95% CI: 1.21-1.87; P < .001), adverse effect (OR: 1.46; 95% CI: 1.10-1.94; P = .009), depression (OR: 1.94; 95% CI: 1.47-2.57; P < .001), and dementia (OR: 1.66; 95% CI: 1.21-2.27; P = .001). Independent predictors for poor medication adherence are shown in Table 4.
Multivariate Logistic Regression Analysis of Predictors for Poor NOAC Adherence.
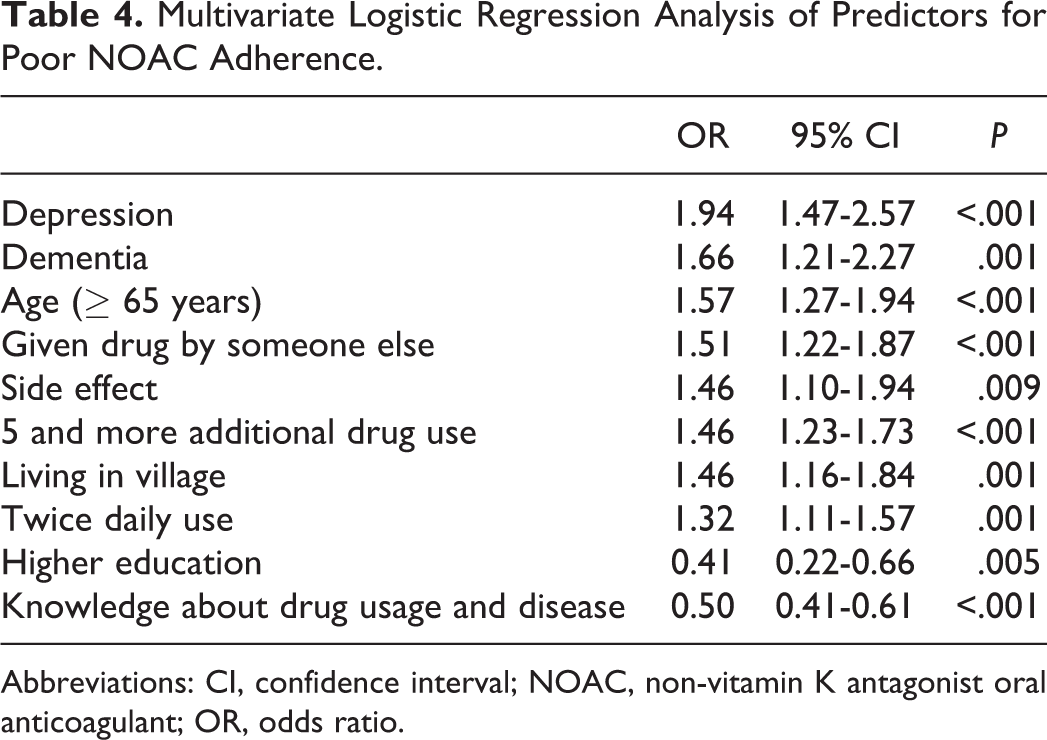
Abbreviations: CI, confidence interval; NOAC, non-vitamin K antagonist oral anticoagulant; OR, odds ratio.
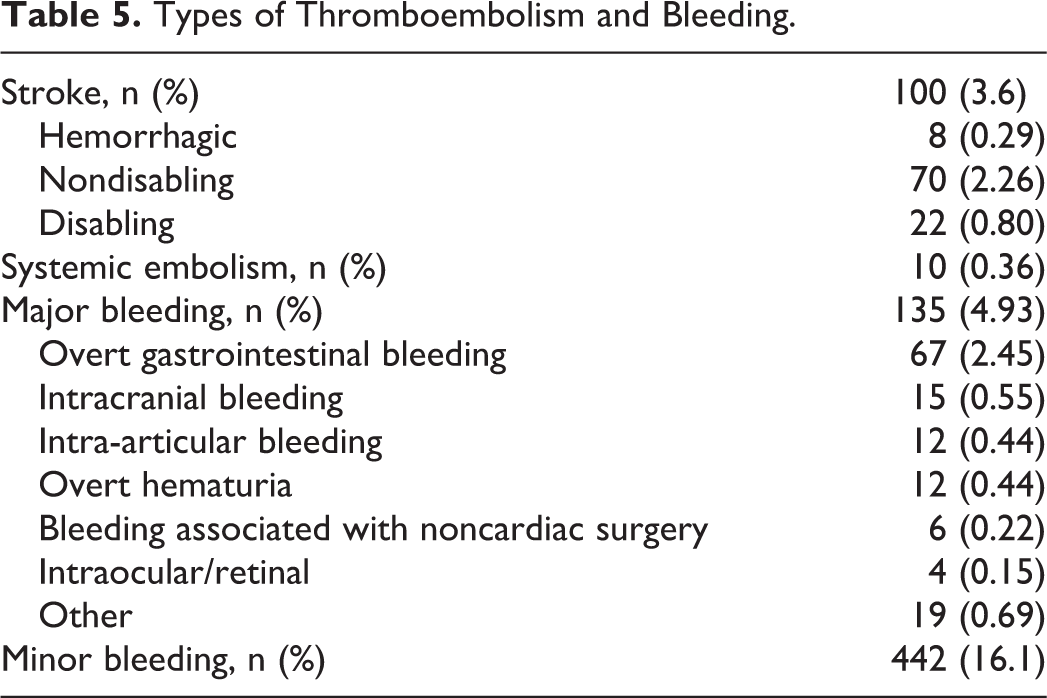
Totally, 577 (21.1%) patients had bleeding event during NOAC treatment. Type of major bleeding is presented in Table 5. Nonadherent patients have higher HAS-BLED score than adherent and moderate adherent patients (3.4 ± 1.1 vs 3 ± 1, P < .001). In nonadherent patients, the rates of major and minor bleeding were increased (P < .05; Table 6). Besides this, bleeding rates were higher in patients with Non streoid antiinflammatory drugs (NSAID) usage (29.7% vs 14.7%, P < .001), chronic renal failure (11.4% vs 6.3%, P < .001), and alcohol abuse (3.2% vs 1.4%, P < .007). However, additional antiplatelet treatment rate was similar between patients with and without bleeding (14.3 vs 11.8, P = .124).
Types of Thromboembolism and Bleeding.
The Relation of the Adherence Level With Efficacy and Safety Outcomes.
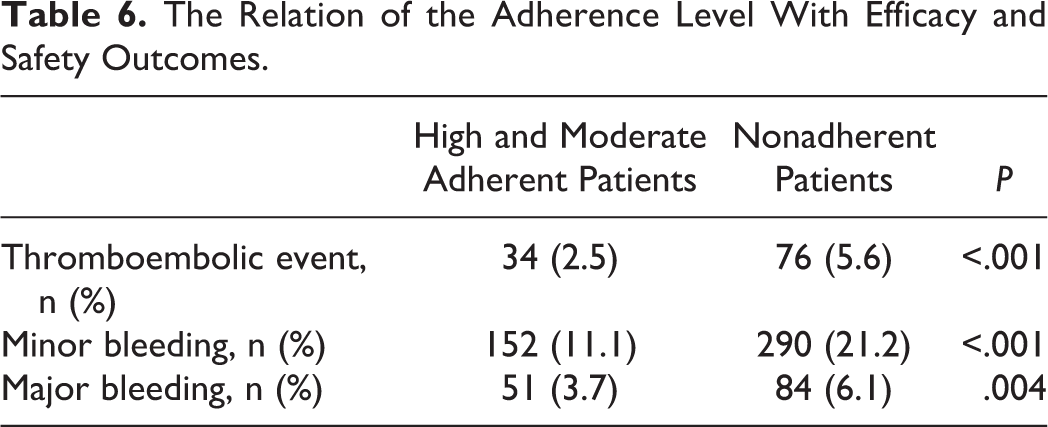
The mean CHA2DS2-VASc score was higher in nonadherent patients (3.7 ± 1.4 vs 3.2 ± 1.4, P < .001). A total of 110 patients had thromboembolic event while taking NOAC treatment. The types of thromboembolic event are presented in Table 5. Thromboembolic events were determined to be increased in nonadherent patients (P < .001).
In comparison with single dose, taking NOAC twice a day was observed to decrease adherence but to have no additional effect on minor (17% vs 16%, P = .411) and major bleeding (5.1% vs 4.7%, P = .645). There was no difference between the use of single (3.6%) and double dose (4.3%) in terms of thromboembolic event during NOAC treatment (P = .421). Duration of NOAC treatment was similar between adherent and nonadherent patients (364 ± 231 vs 355 ± 229, P = .296). However, duration of NOAC treatment was higher in patients who had bleeding (398 ± 255 vs 351 ± 223, P < .001) and stroke (404 ± 244 vs 358 ± 229, P = .049).
Discussion
To our knowledge, this multicenter study is the one with the largest population in which the adherence to NOACs is assessed with self-report based on the 8-item Morisky Adherence Scale. The main findings of this study are as follows: (1) the adherence of Turkish population to NOACs is quite low (<50%); (2) the low level of adherence is associated with bleeding and thromboembolic event; (3) single dose is more advantageous than double dose with regard to medication adherence; (4) education level, sociocultural status, and information about the disease affect the medication adherence; (5) the number of the drugs, additional diseases, and psychiatric disorders decrease medication adherence.
Adherence to NOAC
The high level of medication adherence is of utmost importance for the efficiency of anticoagulant treatment. Nonadherence to NOAC treatment is directly proportional to cardioembolic events. 15,16 In the phase III trials of NOACs, medication adherence of the patients was generally found to be over 90%. 3 –5,17 The high level of adherence rates in clinical trials is thought to result from selection of patients who are less risky for nonadherence, strong motivation by researchers to take the drug, and frequent visits over the course of the trial. The current real-world data appear to differ from the results of randomized controlled trials. In real-world data, medication adherence level evaluated with proportion of days covered (PDC) method was reported to be in a wide range between 47.7% and 95%. 18 –20 This discrepancy is thought to result from the difference and number of the population in which medication adherence is assessed, follow-up duration, divergence of indications for NOAC, and diversity of the methods used to evaluate adherence. The studies with self-report method had also controversial results. Castellucci et al found the general adherence level to NOAC as 56.2%, using the 4-item Morisky Adherence Scale based on self-report in 130 patients with venous thromboembolism. 21 In another study, the medication adherence of 80 patients with strokes receiving dabigatran and rivaroxaban for secondary prophylaxis was 75.8% with the 8-item Morisky Adherence Scale, and the results were found to be correlated with PDC method. Our study involved a much larger population, a great majority of which had been using NOAC for a relatively long time due to NVAF. The adherence level using the 8-item Morisky Adherence Scale was observed to be lower (49%) than those assessed by studies using self-reported method. The reason why the patients have relatively poor medication adherence is that almost all of patients had poor TTR values while using VKA before NOAC treatment, which shows those patients tend to be noncompliant to oral anticoagulants. On the other hand, a nationwide study in Turkey demonstrated that TTR value of patients with NVAF continuing to take VKA instead of NOAC was 50.1 ± 22.9. 10 Based on these data, Turkish patients’ adherence level to oral anticoagulants is below the expected level.
Low medication adherence leads not only to decreased efficacy but also to increased rate of bleeding. Considering the short half-life of NOACs, skipping medication for even a short time can increase the risk of bleeding. 16 Similar to available data, our study also found that the rates of minor and major bleeding were significantly increased further in nonadherent patients.
Reasons for Nonadherence
Studies about the factors affecting medication adherence in patients receiving NOAC are inadequate. Available data are based on experience with VKAs. Ethnicity, economical status, education level, unemployment, forgetfulness, lack of information about drug usage, use of additional medications, addiction to drugs and alcohol, and emotional factors could negatively influence the adherence to VKAs. 22 The Program for the Reduction In Medication Errors (PRIME) component of the INR Adherence and Genetics (IN-RANGE) study investigated for 32 months the factors affecting the adherence to VKA. Factors such as smoking, unemployment, indication for medication use, poor quality of life, and cognitive disorder were identified to influence adherence negatively. 23 In this study, several demographical and clinical factors were observed to be independent risk factors for adherence. One of the most important risk factor is having high frequency of cardiovascular risk factors (CHA2DS2-VASc score: 3.5 ± 1.4) of patients. Other risk factors for low adherence level were demographical factors such as advanced age, low level of education and less knowledge about their drug and disease, and living predominantly in rural areas with limited access to a specialist. Administration of the drug by the patient’s relative did not improve but conversely increased nonadherence.
Decreasing the dosage frequency is known to enhance medication adherence. Pan et al demonstrated that compared to 2-pill therapy, a fixed-dose combination can yield important improvements in patient adherence. 24 In another study including 10 697 patients with AF, single doses of antidiabetic, antihypertensive, calcium channel blocker, and diuretic were demonstrated to have advantage over double-dose regimens with regard to medication adherence. 25 Some studies on NOACs showed that single-dose regimen of rivaroxaban was superior to double-dose regimens of apixaban and dabigatran in terms of medication adherence. 19,26 Other studies found no difference in medication adherence between single- and double-dose regimens. 21,27 In our study, double-dose regimen was identified as one of the independent risk factors affecting medication adherence negatively, which is consistent with the hypothesis that fixed-dose combination has better compliance than with a multi-pill regimen. As mentioned above, bleeding rate was not increased in patients taking the medication twice a day, even though nonadherence augmented the rate of bleeding. The reason was that double-dose regimen had a direct impact on medication adherence but was not enough to increase bleeding rate per se.
Improving Adherence
Because there are several factors affecting the level of adherence, patient-based factors associated with medication adherence should be evaluated thoroughly. Since lack of knowledge about medication and disease is a factor impairing adherence, sympathizing with patients who have fear and anxiety, talking face to face about advantages and disadvantages of the treatment, and even explaining the treatment with a comprehensible written form before the start of the therapy would favor adherence. 28,29 Due to the fact that forgetfulness is a distinct risk factor, sharing information on treatment frequently and requesting neurological and psychiatric consultations for disorders that can lead to forgetfulness such as depression and dementia may be needed. For the patients with inalterable risk factors such as advanced age, additional chronic disease, and place of residence, increasing the frequency of follow-up visits to improve adherence may be planned. Wu et al reported that telephone counseling by health-care providers increased adherence substantially and decreased mortality by 41% in nonadherent patients receiving 5 or more drugs. 30
Limitations of the Study
The fact that the data obtained in this study were based on hospital records and patient knowledge might have led to biased and incorrect results. The tests used to assess medication adherence have advantages and disadvantages. No method is gold standard; however, evaluation of the Morisky Adherence Scale according to patient answers might have resulted in overestimating or underestimating the level of medication adherence. Moreover, the fact that enrolled patients had a history of inadequate TTR or cardioembolic event during VKA treatment might have caused a lower-than-expected adherence level. Although the patients receiving NOAC treatment were evaluated during the study for the development of cardioembolic event, long-term follow-up studies are needed to obtain more reliable data.
Conclusion
In our study population from Turkey, adherence to NOACs was found to be considerably low (<50%), using self-reported method with the 8-item Morisky Adherence Scale. Several factors influenced medication adherence, whereas daily single-dose regimen of NOAC had no impact on cardiovascular end points. To improve medication adherence, risk factors particular to the patient should be evaluated and clinical and educational processes should be coordinated.
Footnotes
Acknowledgments
The authors are grateful to İbrahim Halil Özdemir, Utku Şenol, Nurullah Çetin, Asım Enhoş, Cemal Köseoğlu, Abdurrahman Akyüz, Volkan Doğan, Fatih Levent, Ümit Yaşar Sinan, Yüksel Dereli, Tolga Doğan, Özcan Başaran, Özkan Karaca, Ilgın Karaca, Yılmaz Ömür Otlu, Çağlar Özmen, Barış Düzel, Selvi Coşar, Mutlu Sümerkan, Erdal Gürsul, Salih Kiliç, and Kıvanç Yüksel who provide detailed information about patients.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.