
Abstract
Rivaroxaban, a direct factor Xa inhibitor, is widely used to reduce the chance of stroke in patients with atrial fibrillation (AF). It is not clear why the prothrombin time (PT) of the international normalized ratio (INR) fails to correlate with treatment using rivaroxaban in patients with AF. In this study, patient characteristics, the rivaroxaban dosage, AF type, drug history, biochemical properties, and hematological profiles were assessed in patients treated with rivaroxaban. In 69 patients with AF receiving rivaroxaban, 27 (39.1%) patients had a normal INR (≤1.1, group 1), 27 (39.1%) patients had a slightly prolonged INR (1.1∼1.5, group 2), and 15 (21.7%) patients had a significantly prolonged INR (>1.5, group 3). Group 1 patients had a higher incidence of a stroke history than did patients in group 2 (P = .026) and group 3 (P = .032). We scored patients with a persistent AF pattern (1 point), paroxysmal AF pattern (0 point), renal function (ie, the creatinine clearance rate in mL/min/1.73 m2 of >60 as 0 points, of 30∼60 as 1 point, and of <30 as 2 points), and no history of stroke (1 point), and we found that group 3 had a higher score than groups 2 or 1 (2.9 ± 0.8, 2.4 ± 0.7, and 2 ± 0.7, respectively; P < .05). There were similar incidences of bleeding, stroke, and unexpected hospitalizations among the 3 groups. The PT of the INR is determined by multiple variables in patients with AF receiving rivaroxaban. Rivaroxaban-treated patients with AF having different INR values may have similar clinical outcomes.
Introduction
Atrial fibrillation (AF) is the most common sustained cardiac arrhythmia requiring medical care. 1,2 Atrial fibrillation is associated with a 4∼5-fold increase in the risk of ischemic stroke 3 and accounts for up to 15% of strokes in persons of all ages and 30% in persons older than 80 years. 4 Anticoagulant agents are useful for stroke prevention in patients with AF. With the traditional vitamin K antagonist, frequent monitoring of coagulability is required. Direct factor Xa inhibitors, that is, direct oral anticoagulants (DOACs), exhibit predictable pharmacokinetics and pharmacodynamics. The DOACs are given at fixed doses without routine coagulation monitoring. 5,6 Although DOACs have varying effects on coagulation assays, 7 routine monitoring is not needed. The anticoagulability ability of DOACs is variable in patients in clinical practice. 8,9 Coagulation testing may be useful in some situations, such as during urgent surgery, during urgent invasive procedures, with major bleeding, in an overdose situation, and with renal or liver failure. 10,11 Therefore, investigating factors that affect the blood coagulability when using DOACs is important.
Rivaroxaban is a direct factor Xa inhibitor with consistent and predictable anticoagulation effects. 6,8 Comorbidities play critical roles in determining the risk of stroke in patients with AF, 12 –14 which suggests that multiple factors may contribute to the coagulant status of patients with AF. Additionally, the safety of rivaroxaban in patients with AF treated with an anticoagulant is also not well established, whereas hypertension, abnormal liver and renal function, stroke, bleeding, labile international normalized ratios (INRs), elderly, and drugs and alcohol score were proposed for assessing major bleeding risks. 15 The prothrombin time (PT)-INR is a common method used for determining the coagulation status in clinics (especially for patients receiving warfarin). However, the roles of the PT and INR in patients with AF receiving rivaroxaban have not been well elucidated. Tripodi et al reported that PT-INR is useful for monitoring rivaroxaban concentrations, 16 but Testa et al found a poor responsiveness of the PT-INR to DOAC concentrations. 17 Although measuring anti-factor Xa was shown to be superior to monitoring the PT-INR in evaluating the efficacy of DOACs, it is not as widely available in practice compared to the PT-INR. Therefore, the purposes of this study were to evaluate which factors determine the PT-INR in patients with AF receiving rivaroxaban and investigate whether the INR can predict the risks of stroke and bleeding.
Methods
Study Population
This retrospective study included patients with AF using rivaroxaban. The PT-INR was checked after using rivaroxaban. The entire study was conducted with the approval (no. N201706043) of the Taipei Medical University-Joint Institutional Review Board. The following parameters were assessed in each participant: medical history, weight, height, body-mass index (BMI; weight in kg/height2 in m2), laboratory assessment of the PT-INR, and biochemical and hematological profiles. The PT-INR was measured using the STA-Neoplastine CI PLUS kit (Diagnostica Stago, Asnieres, France) with the analyzer system STA-R evolution (Diagnostica Stago, Asnieres, France). Any adverse events, such as stroke or bleeding, after using rivaroxaban were also recorded.
We developed a coagulation score to estimate the coagulability after using rivaroxaban. This score included renal function (creatine clearance rate [CCr]; 2 points for a CCr of <30 mL/min, 1 point for 30 mL/min ≤ CCr < 60 mL/min, and 0 points for a CCr of ≥ 60 mL/min), AF type (0 points for paroxysmal AF and 1 point for persistent AF), and history of stroke (0 points for a positive history and 1 point for a negative history). The CCr was calculated with the Cockcroft–Gault formula: CCr = {[(140 – age) × 5 5 weight]/(72 × serum creatinine)} (× 0.85 for women). 18
Statistical Analysis
Continuous variables are expressed as the mean (standard deviation). Differences between the different groups were compared by a 1-way analysis of variance with a post hoc Fisher least significant difference (LSD) test. Categorical variables are reported as frequencies and were compared using Pearson χ2 analysis. Statistical significance was set to P < .05. All statistical analyses were performed with SigmaPlot vers. 12.3 software (Systat Software, San Jose, California).
Results
Sixty-nine patients using rivaroxaban were included in this study. Twenty-seven (39.1%) patients had a normal INR (≤1.1, group 1), 27 (39.1%) patients had a slightly prolonged INR (1.1∼1.5, group 2), and 15 (21.7%) patients had a significantly prolonged INR (>1.5, group 3).Table 1 shows the baseline characteristics of these 3 groups. The gender, age, body weight, height, BMI, incidences of hypertension, diabetes mellitus, stroke, coronary artery disease, renal function, liver function, platelet count, hemoglobin, medication history, and the sampling interval for measuring the PT-INR were similar among the 3 groups. However, group 1 patients had a higher incidence of a stroke history than did groups 2 (P = .026) and 3 (P = .032). In addition, patients in the 3 groups had different CCr values and types of AF. Coagulation scores significantly differed in the 3 groups while that of group 3 was significantly greater than that of group 1 (2.9 ± 0.8 vs 2 ± 0.7, P < .05), and coagulation scores between groups 1 and 2 and between groups 2 and 3 were the same (Figure 1). In addition, there was a good correlation of the INR with coagulation scores (Figure 1B).
Characteristics of Patients Using Rivaroxaban in the Different Coagulability Groups.a
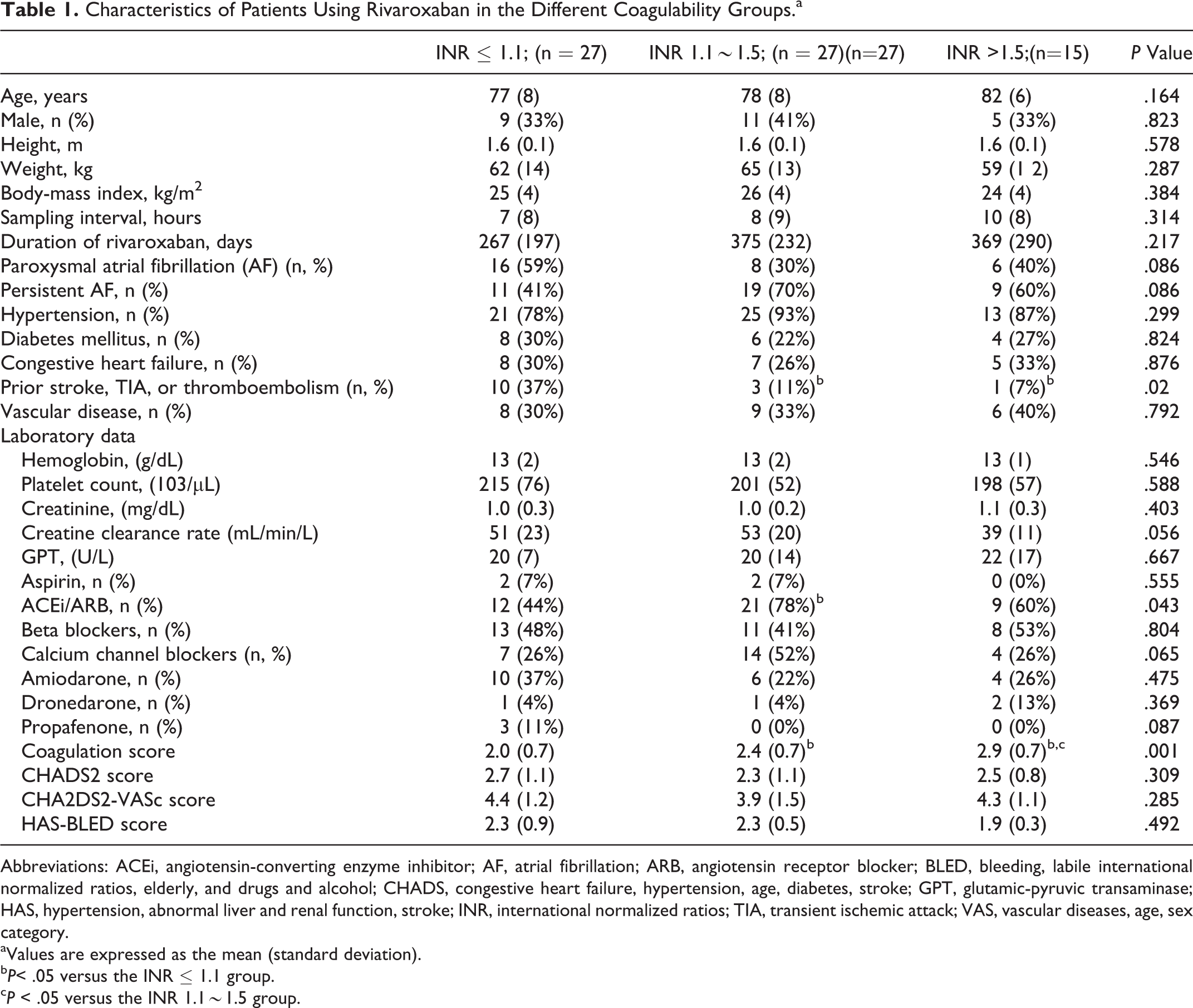
Abbreviations: ACEi, angiotensin-converting enzyme inhibitor; AF, atrial fibrillation; ARB, angiotensin receptor blocker; BLED, bleeding, labile international normalized ratios, elderly, and drugs and alcohol; CHADS, congestive heart failure, hypertension, age, diabetes, stroke; GPT, glutamic-pyruvic transaminase; HAS, hypertension, abnormal liver and renal function, stroke; INR, international normalized ratios; TIA, transient ischemic attack; VAS, vascular diseases, age, sex category.
aValues are expressed as the mean (standard deviation).
bP< .05 versus the INR ≤ 1.1 group.
cP < .05 versus the INR 1.1∼1.5 group.
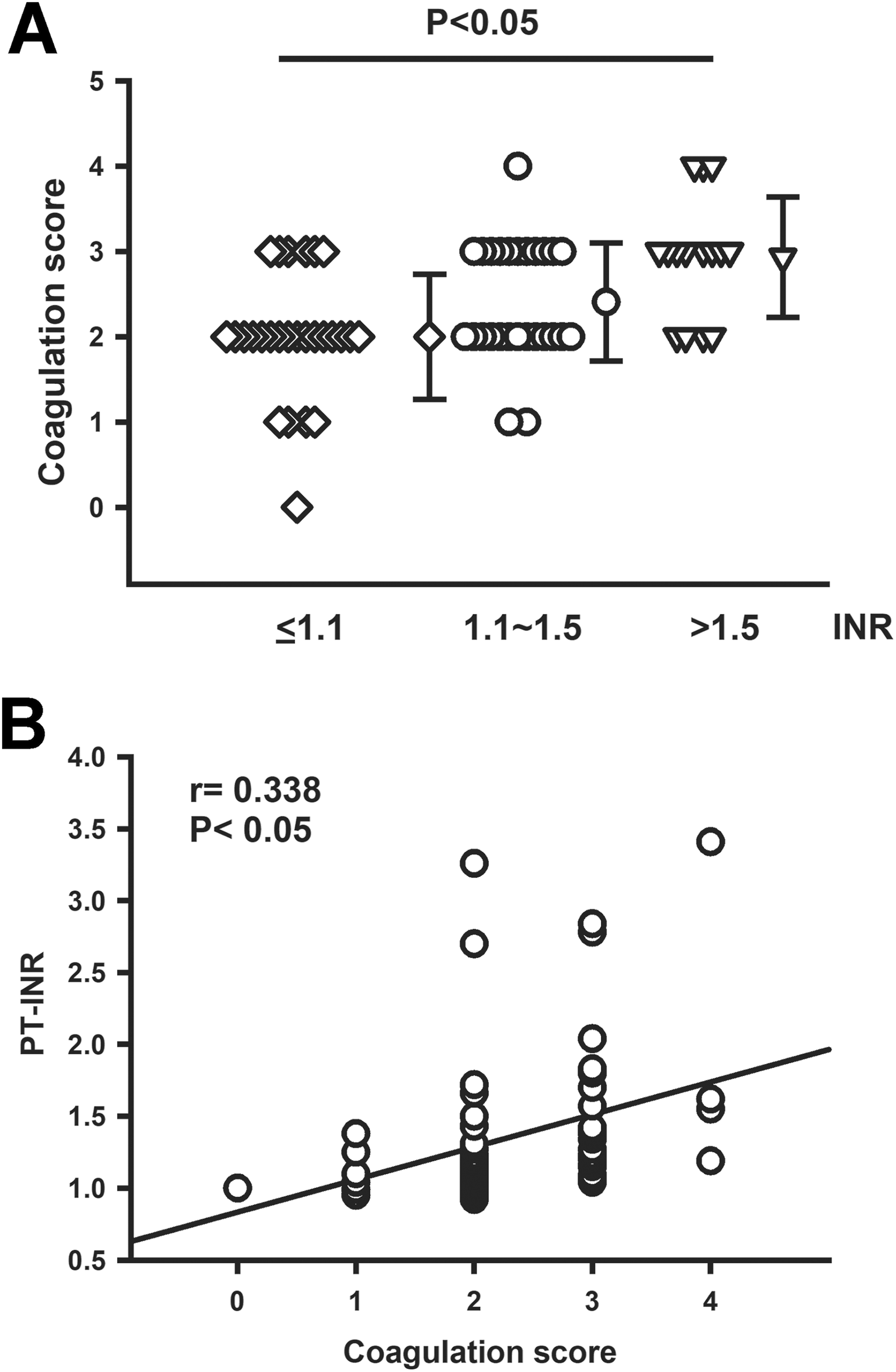
Panel A. Distributions of coagulation scores in different international normalized ratio (INR) groups. The coagulation score in the normal prothrombin time (PT)-INR group was significantly lower than those of the other 2 groups (P < .05). Panel B. A good linear correlation was found between the INR and coagulation scores.
We studied outcomes in different groups and found that there were similar incidences of bleeding, stroke, and unexpected hospitalizations (Figure 2). In patients with paroxysmal AF, there were similar incidences (19%, 25%, and 50%, respectively, P > .05) of AF recurrence noted by medical records in groups 1, 2, and 3 patients. Figure 3 shows the percentage of a prolonged INR in groups with different coagulation scores, whereas the higher-score groups had higher percentages of a prolonged INR than did lower-score groups (P < .05).
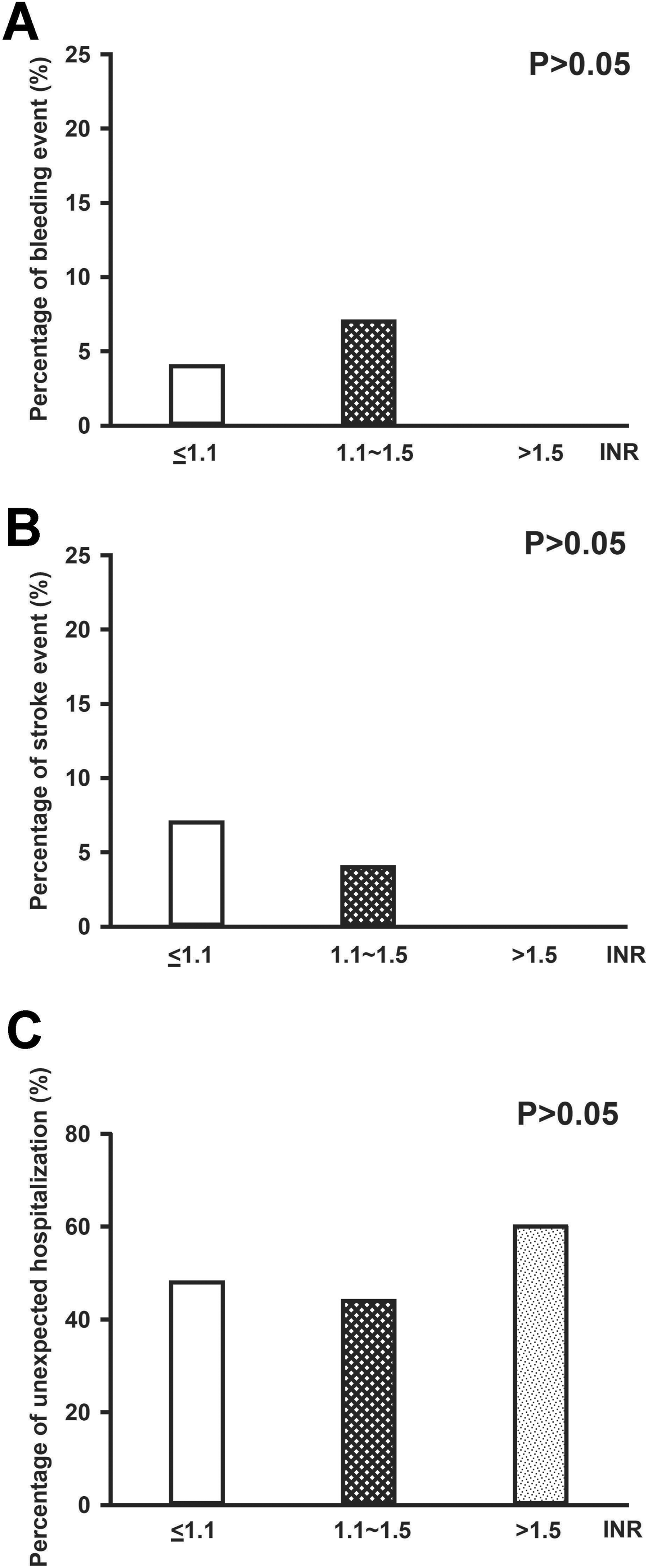
Clinical outcomes after using rivaroxaban in different international normalized ratio (INR) groups. There were similar incidences of major bleeding, stroke, and unexpected hospitalizations.
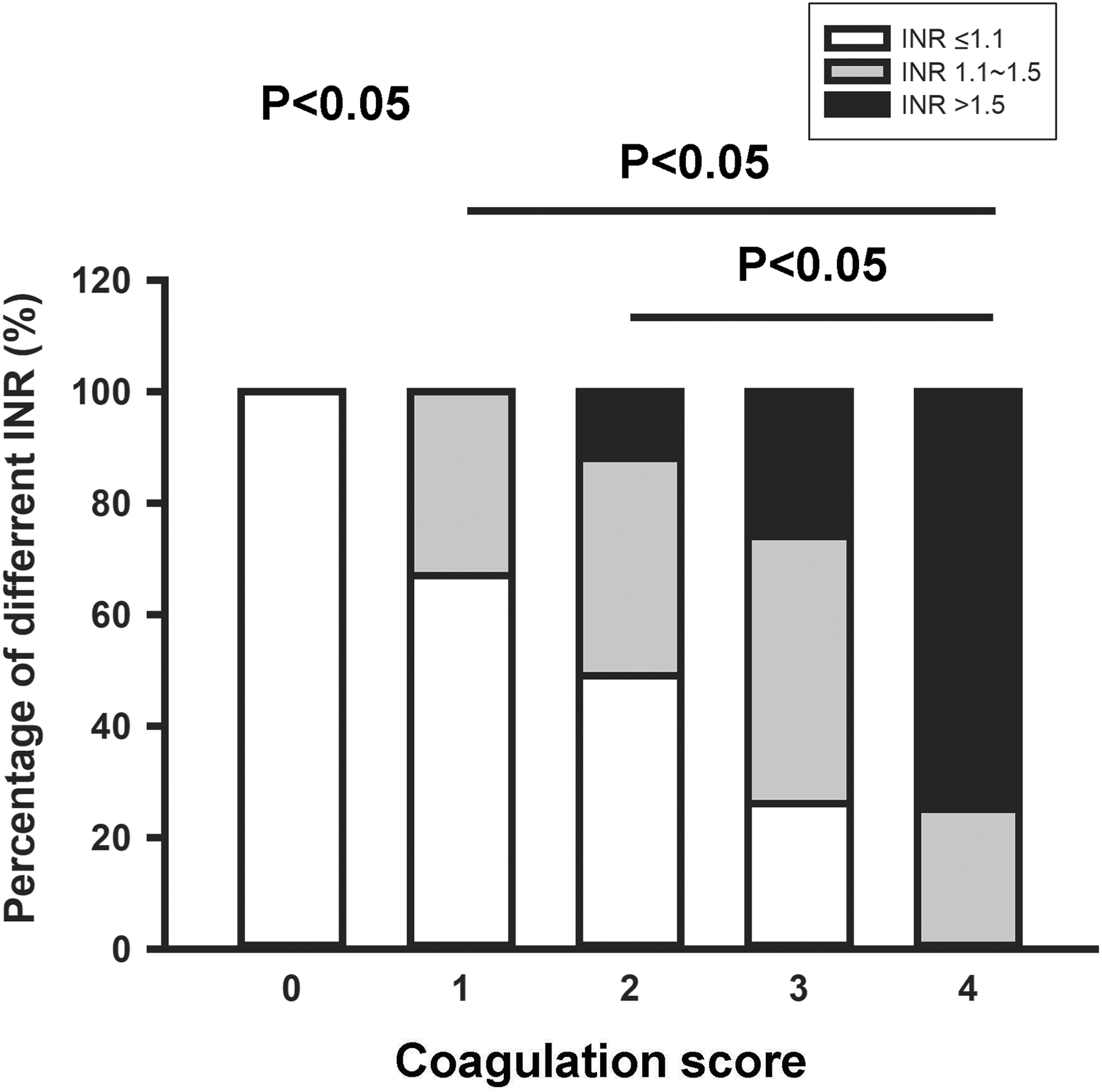
Percentages of different prothrombin time-international normalized ratio (PT-INR) groups (≤1.1, 1.1∼1.5 and >1.5) with different coagulation scores.
Discussion
Direct oral anticoagulants are used to replace traditional vitamin K antagonists for stroke prevention. They provide an alternative treatment that has predictable pharmacokinetics and pharmacodynamics and do not require routine coagulation monitoring. However, there is no available information on the role of the INR and the use of DOACs. In this study, we identified several potential factors that determine the PT-INR in patients with AF receiving rivaroxaban. In addition, for the first time, this study found that patients with an INR of >1.5 may have fewer adverse events (bleeding, stroke, and unexpected hospitalizations) than those with an INR of ≤ 1.5. These findings indicate a novel prognostic role of the INR in patients with AF treated with DOACs.
Body weight has a limited influence on the effect of rivaroxaban. 19 In older patients, rivaroxaban clearance is reduced, which may increase the risk of bleeding. 20 However, in this study, we found that age did not differ among the different INR groups in our study. We found that renal function tended to be poorer in patients with AF with a prolonged INR after rivaroxaban. Renal impairment may increase exposure to rivaroxaban. 9 Since data on the pharmacokinetics and pharmacodynamics suggest that rivaroxaban might not cover 24-hour anticoagulant effects, patients with relatively poorer renal function are expected to have longer effective concentrations of rivaroxaban with daily use, which may contribute to a higher INR and better clinical outcomes. However, the Canadian Cardiovascular Society suggests follow-up for reassessment of therapy at least every 6 months and every 3∼6 months for renal impairment in patients receiving rivaroxaban. 21
A hypercoagulability status was noted in patients with AF. 19 A previous study showed that the efficacy and safety of DOACs in treating patients with AF were consistent irrespective of a history of stroke. 22 In our study, the prolonged INR group had less of a stroke history, which suggests the possibility that this group of patients were less hypercoagulant, resulting in a prolongation of the INR. Interestingly, this study found that patients treated with rivaroxaban and with a lower INR may have had a lower percentage of persistent AF. Although the mechanism is not clear, we could not exclude the probability that patients in this group may have had poorer adherence to rivaroxaban.
Although the INR differed among these 3 groups, bleeding events did not significantly differ among the different INR groups. Similarly, stroke incidences did not significantly differ among the different INR groups. However, there were 2 cases among normal INR patients (group 1) and no cases in groups 2 or 3 who had a stroke, which suggests the potential role of the INR in the potency of rivaroxaban in AF prevention. This study found that patients treated with rivaroxaban in the different PT-INR groups had similar incidences of bleeding and stroke events. However, patients with a PT-INR of >1.5 had no stroke events, suggesting that an adequately prolonged PT-INR is a potential marker for efficacious treatment of patients having AF with rivaroxaban. Therefore, monitoring the PT-INR may be recommended in patients with a high stroke risk and persistent AF. Further studies including more patients with longer follow-up times are needed to confirm this suggestion.
Although the mechanism of having a positive coagulation score when using rivaroxaban is not clear, rivaroxaban may more greatly prolong coagulation with persistent AF than with paroxysmal AF. In patients receiving DOACs, those with paroxysmal AF had a lower risk of stroke than those with persistent AF. 23,24 These findings may imply that patients with persistent AF were hypercoagulant with a prolonged INR. Therefore, we chose the renal function, stroke history, and AF type to comprise the coagulation scoring system.
In conclusion, the PT-INR of the INR is determined by multiple variables in patients with AF receiving rivaroxaban. Rivaroxaban-treated patients with AF with different INR values may have similar clinical outcomes.
Limitations
Potential limitations of our study merit consideration. First, activities of DOACs change dynamically, and the maximal effect of rivaroxaban is reached 3 hours after drug intake. 25 Based on the known pharmacodynamics of rivaroxaban, 25 the expected plasma concentration of rivaroxaban with the sampling intervals of 7 to 10 hours in this study may be around half of its peak concentration. Therefore, we did not detect the maximal effect of rivaroxaban. Second, the anti-factor Xa activity chromogenic assay was proven to have excellent correlation with plasma concentrations of DOACs 26 –30 and is a reliable marker for assessing compliance with DOACs, especially in special populations such as those with chronic kidney disease (stage III), pregnancy, multiple drug interactions, and so on. However, anti-factor Xa levels were not available in this study. Third, Douxfils et al released a very important guidance for laboratory assays, which suggested that PT-INR sensitivity to rivaroxaban was highly dependent on the reagent used. 31 Previous studies showed that interactions between DOACs and different reagents were variable. 25,26 Reagents, such as neoplastin and recombiplastin, are more sensitive in the presence of rivaroxaban at both the trough and peak levels. 27 However, this method has not yet been widely been applied in clinics due to different reagent sensitivities and variable impacts on assay results. Since STA-Neoplastin CI is the only agent used in our hospital, it is not clear whether measuring the PT-INR using other reagents may produce similar findings. In addition, rivaroxaban, unlike other DOACs, was only used in patients with a CCr value of >30 mL/min. We do not know whether this result can be applied to other DOACs. Finally, the scale of this study was too small to elucidate the clinical relevance between the PT-INR and patient outcomes. Durations of follow-up were variable and that may have affected the results of the study. In addition, observations of AF may have been underestimated. Thus, this study may be more like hypothesis-generating research rather than a conclusive study.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The present work was supported by grants (MOST 103-2314-B-038-055 and MOST107-2314-B-038-097-MY2) from the Ministry of Science and Technology, Taiwan and (102TMU-WFH-09, 105swf02, and 106-eva-06) from Wang Fang Hospital, Taipei Medical University.