
Abstract
The objective of our study is to detect the patient group that will most benefit from intravenous (IV) thrombolytic therapy by showing predictive factors of good functional outcomes. The present study covers 88 patients who were admitted to our clinic within the first 4.5 hours from the onset of stroke symptoms, diagnosed with acute ischemic stroke and who received IV thrombolytic therapy between May 2014 and June 2017 as a result of a retrospective analysis of a database prospectively collected. The patients with a score of ≤2 on modified Rankin scale within 3 months were accepted as good functional outcome and those with a score of >2 were accepted as poor functional outcome. As a result, within the period of 3 months posttreatment, good functional outcomes were obtained in 45 (51.1%) patients and poor functional outcomes were obtained in 43 (48.9%) patients. In comparisons, cardioembolic stroke group was statistically significantly higher in the good functional outcome group (P = .03). Pretreatment National Institute of Health Stroke Scale (NIHSS) scores (P < .001), presence of proximal hyperintense middle cerebral artery sign in noncontrast computed brain tomography (P = .03), and being aged ≥80 and older (P = .04) were markedly higher in the group with poor functional outcomes. In conclusion, our study demonstrated that cardioembolic strokes may have an impact on good functional outcomes and being aged 80 and older, presence of proximal HMCAS in computed brain tomography, and pretreatment NIHSS scores may have an impact on poor functional outcomes.
Introduction
After the Food and Drug Administration of the United States approved the use of intravenous (IV) thrombolytic therapy with recombinant tissue plasminogen activator (r-tPA) in acute ischemic stroke, the American Heart Association/American Stroke Association (AHA/ASA) published that it is very effective when administered within 3 hours of the onset of symptoms in patients who met the eligibility criteria and remained effective for up to 4.5 hours. 1,2 Randomized controlled studies have shown that IV r-tPA therapy administered within the first 3 hours after acute ischemic stroke led to a 10% to 30% decrease in the mortality and disability of patients at 3 to 6 months posttreatment. Whether there are any benefits of administration after 3 hours is controversial. 3 -6 Other controlled randomized studies have shown that the death rate caused by fatal intracranial hemorrhage within 7 to 10 days following IV r-tPA administration is high. Despite this high baseline risk, the mortality rate was lower in the group receiving therapy than in the control group after 3 months. 4 During an 18-month follow-up, researchers from the third International Stroke Trial detected that the group receiving IV r-tPA therapy was functionally better. 7 Recent studies have shown that results obtained by mechanical methods were superior to IV thrombolytic therapies. 8,9 However, the number of centers in our country and throughout the world that are conducting initiative therapy is insufficient. Therefore, IV therapy with r-tPA remains important for the treatment of acute ischemic stroke. Predicting the groups for which this therapy will be most effective is important for minimizing mortality and improving functional outcomes. We aimed to determine which patient group will benefit most from this therapy by reviewing the risk factors and results of our patients who were admitted to emergency services within the first 4.5 hours from the onset of symptoms due to acute ischemic stroke and subsequently received IV thrombolytic therapy.
Materials and Methods
The clinical data of 88 patients who were admitted to emergency services within the first 4.5 hours following the onset of symptoms and were then diagnosed with acute ischemic stroke and received thrombolytic therapy with IV r-tPA between May 2014 and June 2017 were retrospectively reviewed. All patients were analyzed according to the AHA/ASA 2013 10 and 2016 11 guideline recommendations for enrollment and contraindications before thrombolytic therapy was administered. The patients received 10% of the total dose of r-tPA, which was calculated as 0.9 mg/kg (maximum 90 mg, Activase), as an IV bolus, with the remaining 90% given as an infusion over the course of 1 hour. Risk factors that could cause the ischemic stroke, detailed demographics and clinical characteristics, blood hemogram and biochemistry results, and onset-to-needle time were recorded from patient files. The age limit was set at 60 years, and the patients were categorized into groups of <60 years, 60 to 80 years, and >80 years. All patients were grouped according to the etiological classification of Trial of Stroke Org 10172 in Acute Stroke Treatment (TOAST). 12 A 16-slice tomography device (Siemens Somatom Emotion) was used for computed brain tomography (brain CT) scans taken before and 24 hours after the treatment and when needed. Brain CTs were obtained using a 4-mm slice thickness, and no contrast substance was used. In the first brain CT, hyperintense middle cerebral artery sign (HMCAS) presence was noted as a proximal (p-HMCAS) or distal (d-HMCAS) embolism. Intracerebral hemorrhage causing a disruption in general conditions was defined as symptomatic intracerebral hemorrhage (sICH), and an intracerebral hemorrhage that was detected incidentally in control imaging was defined as asymptomatic intracerebral hemorrhage (aICH). Intracranial hemorrhages occurring within the first 36 hours posttreatment were evaluated as r-tPA complications. Pretreatment neurological disabilities of the patients were evaluated by The National Institute of Health Stroke Scale (NIHSS) scores, and neurological disabilities 3 months posttreatment were evaluated by modified Rankin scale (mRS) scores. Modified Rankin scale scores ≤2 in the third month were accepted as good functional outcomes, and mRS scores >2 were accepted as poor functional outcomes. All data are summarized in Table 1.
Demographic and Clinical Characteristics of Patients.
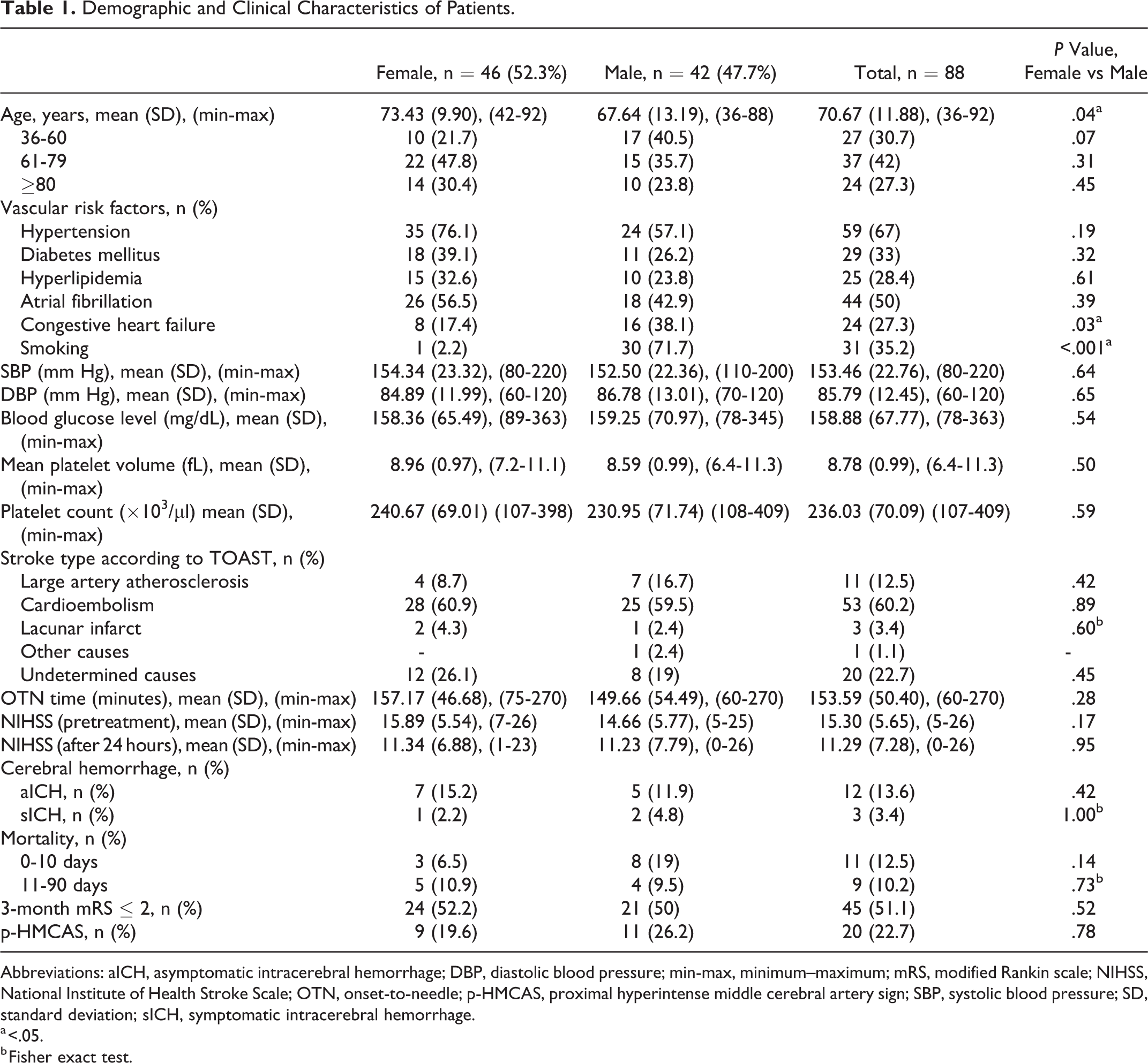
Abbreviations: aICH, asymptomatic intracerebral hemorrhage; DBP, diastolic blood pressure; min-max, minimum–maximum; mRS, modified Rankin scale; NIHSS, National Institute of Health Stroke Scale; OTN, onset-to-needle; p-HMCAS, proximal hyperintense middle cerebral artery sign; SBP, systolic blood pressure; SD, standard deviation; sICH, symptomatic intracerebral hemorrhage.
a <.05.
b Fisher exact test.
Statistical Analysis
Statistical analysis was performed with Statistical Package for the Social Sciences (version 24.0; IBM Corp, Armonk, NY, USA). χ2 was used for comparing the baseline categorical data, Student t test was used for the parametric data to compare the 2 independent groups, and Mann-Whitney U tests were used for nonparametric data. For statistically significant (P < .05) parameters in the single variable analyses, logistic regression and multivariable linear regression analyses were applied. Data were analyzed with a confidence interval of 95%, and P < .05 was accepted as statistically significant.
Results
Out of the 88 patients enrolled in the study, 42 were male (47.7%), with an average age of 67.64 ± 13.19 years, and 46 were female (52.3%), with an average age of 73.43 ± 42.92 years. The demographic and clinical characteristics of the patients are presented in Table 1. Even though there was no difference in sex distribution, according to the age range, male patients were younger (P = .04). Congestive heart disease (P = .03) and smoking (P < 0.001) were more common in male patients than in female patients. There was no sex difference for any other risk factors. According to TOAST classification, strokes were caused by large artery atherosclerosis in 11 (12.5%) patients, cardioembolic strokes in 53 (60.2%), lacunar infarcts in 3 (3.4%), and other in 1 (1.1%). No cause could be determined in 20 (22.7%) patients. Onset-to-needle time was the mean (SD) (min-max) of 153.59 (50.40) (60-270) minutes. In the third month control posttreatment, good and poor functional outcomes were detected in 45 (51.1%) and 43 (48.9%) patients, respectively. In comparisons, according to stroke subtypes, the strokes caused by cardioembolisms appeared to have better functional outcomes (71.1% vs 48.8%, P = .03). Advanced age (P = .005), elevated pretreatment NIHSS scores (P < .001), and the presence of a HMCAS (31.6% vs 13.3%, P = .03) negatively affected the functional outcomes (Table 2). Poor functional outcomes were remarkably high in patients >80 years of age (37.2% vs 17.8%, P = .04).
Comparison of Potential Predictive Factors and Mortality Times of Good and Poor Functional Outcomes of Patients at the End of the 3-Month Period.
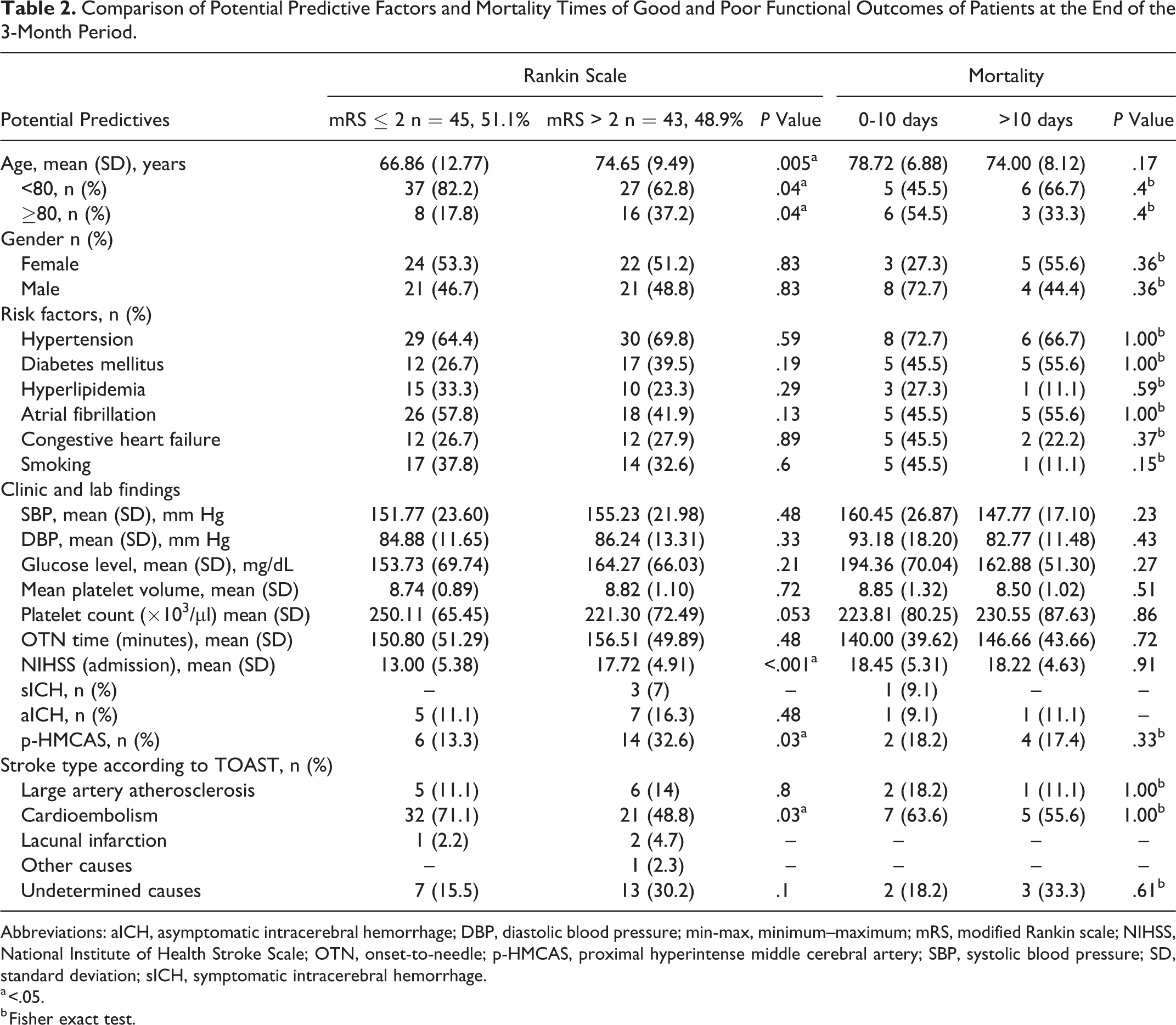
Abbreviations: aICH, asymptomatic intracerebral hemorrhage; DBP, diastolic blood pressure; min-max, minimum–maximum; mRS, modified Rankin scale; NIHSS, National Institute of Health Stroke Scale; OTN, onset-to-needle; p-HMCAS, proximal hyperintense middle cerebral artery; SBP, systolic blood pressure; SD, standard deviation; sICH, symptomatic intracerebral hemorrhage.
a <.05.
b Fisher exact test.
Posttreatment sICH and aICH were observed in 3 (3.4%) and 12 (13.6%) patients, respectively. Of these 3 patients, one developed aICH and one developed sICH and died within 10 days, and the third patient developed aICH and died after 10 days. Upon follow-up, 11 patients died within the first 10 days (3 females, 8 males), 9 patients died after 10 days (5 females, 4 males), and a total of 20 patients died within 3 months (22.7%). The causes of death were large artery atherosclerosis, immobilization, and interfering infections. There was no difference in mortality levels between the groups (Table 2).
Results from logistic regression and multivariable regression analyses of factors having an impact on functional results are presented in Table 3. According to these results, the number of patients with cardioembolic strokes was significantly higher in the good functional outcome group (R2 = 0.05, β = 0.38, 95% CI = 0.16-0.93), and the numbers of patients who were 80 years of age or older (R2 = 0.04, β = 2.74, 95% CI = 1.02-7.32), patients with high NIHSS scores (R2 = 0.17, β = 0.42, 95% CI = 0.02-0.05) and patients with detected p-HMCAS (R2 = 0.05, β = 3.13, 95% CI = 1.07-9.15) were significantly higher in the poor functional outcome group.
Results of Logistic Regression and Multivariable Regression Analyses of Factors Having an Impact on Functional Result in the 3-Month Period.
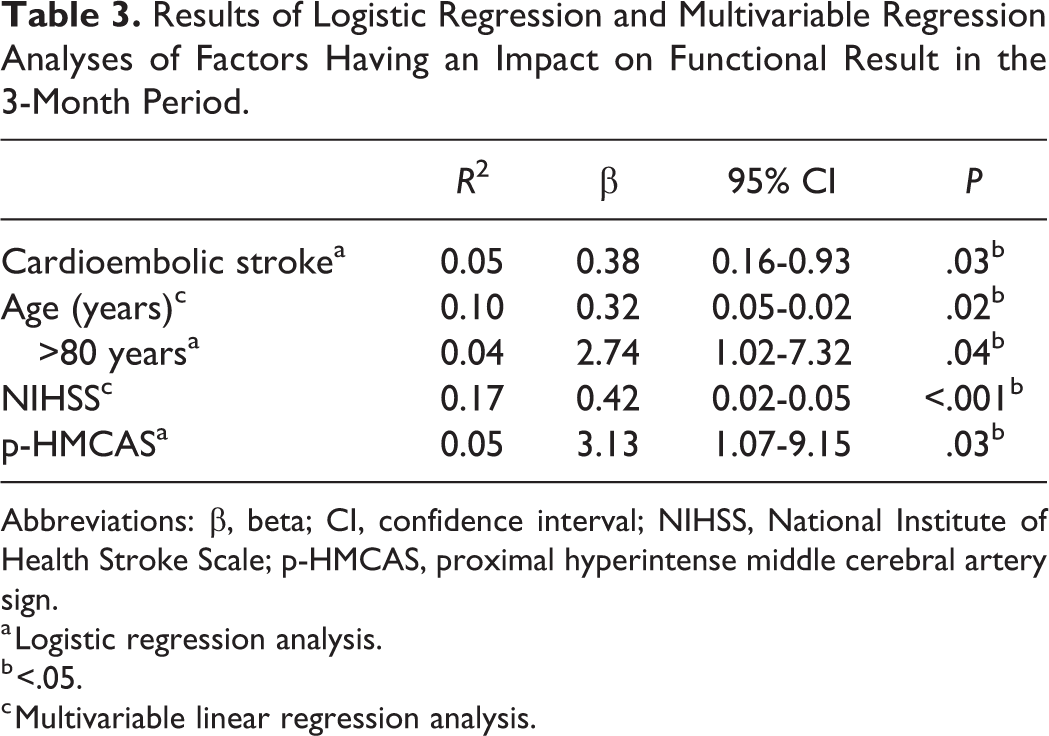
Abbreviations: β, beta; CI, confidence interval; NIHSS, National Institute of Health Stroke Scale; p-HMCAS, proximal hyperintense middle cerebral artery sign.
a Logistic regression analysis.
b <.05.
c Multivariable linear regression analysis.
Discussion
Strokes are the second most frequent cause of death around the world, and 80% to 85% of these strokes are ischemic in nature. Intravenous r-TPA administered as early as possible leads to less disability 3 to 6 months after the ischemic attack, independent of the severity of the stroke. 5 Researchers agree that the treatment should be administered before 4.5 hours. However, there is no consensus regarding patients older than 80 years of age. 13 A relative contraindication is discussed for treatment administered between 3 and 4.5 hours in patients older than 80. 11 Emberson et al conducted a meta-analysis of 9 studies, which included 3391 patients administered r-TPA and 3365 controls. The benefit rate of patients older than 80 administered r-TPA between 0 and 3 hours was the same as that of the 18 to 80 age-group. However, treatment seemed less effective in patients older than 80 who were treated between 3 and 4.5 hours. Patients older than 80 exhibited higher mortality rates and worse functional outcomes. 5 Bhatnagar and Lees reached the same conclusion in their meta-analysis of 13 studies. In addition, they emphasized that there was no difference between the age groups for possibly developing intracerebral hematomas (ISH), and deaths within 3 to 6 months were caused by immobilization and infections. Deaths occurring in the first 7 to 10 days relative to ISH were excluded. There was no sex association in both meta-analyses. 14 Buijs and Uyttenboogaart emphasized that age and sex caused a difference in permanent disability in the follow-up and reported that middle-aged females had better prognoses than males, while males with an advanced age had better prognoses than females. A decrease in neuronal plasticity, disruption in collateral circulation, comorbid conditions before the stroke, and a high number of medical complications after the stroke are thought to contribute to the increase in poor functional outcomes in the elderly patients. 15 In the group of patients older than 80 years of age in our study, mortality did not differ from that of the group of patients below 80, but the number of patients with poor functional outcomes was significantly higher. We did not detect any association with sex. These data support other studies that detected no association with gender.
Dyslipidemia has been reported to adversely affect the outcome of patients after IV recombinant tissue plasminogen activator (rt-PA). 16,17 It is thought to originate from the formation of a nonsoluble lipid-rich thrombus, which can lead to greater infarction and hemorrhagic transformation. 16
It has been reported in some studies that high blood sugar and blood pressure during admission to the hospital affect the outcome negatively. 17,18 Diabetes mellitus (DM) increases the concentration of serum plasminogen activator inhibitor 1 and decreases fibrinolysis. 19 Patients with DM had a lower chance for recovery, lower functional independence, and higher mortality rates in the Safe Implementation of Thrombolysis in Stroke-Monitoring Study trial. 20 Thoren et al also showed a relationship between basal blood glucose and cerebral edema in IV thrombolytic patients. 21 This can be said to arise from the fact that high glucose may impair the blood–brain barrier. 22
On the contrary, many researchers believe that hypertension, DM, hyperlipidemia, atrial fibrillation, congestive heart disease, smoking, alcohol consumption, and other vascular risk factors have an impact on the generation of ischemic cerebral vascular disease but that they do not contribute to permanent functional disability after r-tPA therapy. 5,14,23 We found that advanced age, presence of congestive heart disease, and smoking were important risk factors for developing ischemic strokes. While male sex was detected as a significant risk factor, this factor may be related to the fact that the previously mentioned risk factors were more common in male patients. These findings, considered a risk factor for ischemic stroke, did not have an impact on functional outcomes 3 months later.
According to current US and European guidelines, platelet count (PC) <100 × 109/L is considered as a contraindication to intravenous thrombolytic therapy (IVT). 10,13 However, in patients treated with IVT, there aren’t enough studies to investigate the effect of PC on mortality, functional outcome, and risk of bleeding. In the study of Gensicke et al, 24 it was reported that as PC decreased, the risk of sICH increased, but the mortality and poor outcome decreased. We have seen in our study that the number of platelets is not related to the functional outcome. Mean platelet volume (MPV) is an important biomarker for evaluating platelet activation and increased MPV is associated with ischemic conditions such as cerebral infarction. 25 We did not find any relationship between MPV and functional outcome in our study.
The National Institute of Neurological Disorders and Stroke study showed that IV thrombolytic therapy had a consistent impact on the functional outcome of all ischemic stroke subtypes. 3 However, subsequent studies have demonstrated that responses to r-tPA therapy may be different according to stroke subtypes, 26 and some studies have shown no difference in functional outcomes between stroke subtypes. 27 A thrombus generated due to slow blood circulation in cardiac cavities is richer in fibrin, and a thrombus generated under fast blood circulation in atherosclerotic stenotic lesions is richer in platelets. 28 Therefore, fibrinolytic agents such as tissue-type plasminogen activator and urokinase are thought to be more effective in cardiac-originating embolisms. 29 Whether responses to IV r-tPA are different in cardioembolic strokes compared to other stroke types is of interest to researchers. However, the results of studies on cardioembolic strokes are contradictory. Despite authors reporting that functional outcomes are worse in patients with cardioembolic strokes and that they are under a higher risk of hemorrhagic transformation, 29,30 most researchers believe that stroke types do not have an impact on therapy responses. 4,14,22 Molina and Montaner compared patients with cardioembolic stroke with other stroke subtypes after r-tPA and reported earlier and faster proximal middle cerebral artery recanalization. 31 In our study, compared with other patients, patients in the group of cardioembolic-related strokes were significantly better functionally after a period of 3 months. These data indicate that cardioembolisms are predictive of good outcomes.
In most stroke units, noncontrast brain CTs are used as the first imaging method in the hyperacute period. Hyperdense imaging of the cerebral artery in the noncontrast brain CT is accepted as evidence of ischemic stroke, meaning that the cerebral artery is congested due to thrombus or embolism. When HMCAS findings are compared with cerebral angiography, there is a high level of specificity (95%) but low level of sensitivity (52%). 32 In the absence of HMCAS, the possibility of artery congestion is 50%. The possibility of detecting HMCAS increases when the CT slices are taken with thinner intervals. 33 Since the diameters of proximal cerebral arteries are thicker compared to distal parts, the possibility of imaging them during a brain CT is higher (47% vs. 37%). 34 Li and Davis 35 detected 17.5% p-HMCAS in their study and reported that the presence of p-HMCAS led to bad neurological recoveries. We observed p-HMCAS in 20 (22.7%) patients from our study. Most of these patients had significantly higher poor functional outcomes following thrombolytic therapy, which was evaluated as a predictive factor.
The NIHSS is an important prognostic indicator in patients with acute ischemic stroke and is generally accepted by researchers. The NIHSS is predictive of clinical improvement following IV thrombolytic therapy in patients with acute ischemic stroke. Rocha et al published that NIHSS scores were also high before treatment in patients who did not recover dramatically following IV thromboembolism. Budimkic et al accepted that NIHSS ≤15 is a very good prognosis predictor. 36 -38 In our study, NIHSS scores were statistically higher in our group of patients with poor functional outcomes.
The effectiveness of IV r-tPA has been proven within 4.5 hours following the onset of symptoms. However, not all patients benefit from IV r-tPA as intended. There is a need for determining the subgroups of patients who will benefit from r-tPA after acute ischemic strokes. Having more information regarding factors that affect the clinical outcomes before thromboembolism will contribute to obtaining better functional outcomes. Immediate endovascular treatment methods may be considered for patients who are believed to not benefit from IV thrombolytic therapy.
The limitations of our study were that it was performed in a single center, and the number of patients was low. In this study, the predictive factors in patients with acute ischemic stroke treated with IV r-tPA were evaluated according to functional outcomes. In the older group and the group with high NIHSS scores before treatment, the presence of HMCAS was considered to be predictive of poor functional outcomes, and cardioembolic strokes were considered to be predictive of good functional outcomes. Intravenous thrombolytic therapy for acute ischemic strokes is an effective and safe treatment for selected patients with acute ischemic stroke if given within 4.5 hours. This treatment increases the number of ambulatory patients and reduces disability.
Footnotes
Acknowledgments
The investigators express their gratitude to Rahmi Özdemir for his statistical supervising.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.