
Abstract
Predictors of in-hospital mortality from massive pulmonary embolism (PE) were retrospectively assessed in 78 patients who received thrombolytic therapy. Mortality from PE was 19% (15 of 78). Mortality from PE was higher in those with shock, 36% (12 of 33) versus no shock, 7% (3 of 45; P = .001), 21% (7 of 34) with right ventricle (RV) hypokinesis, and 20% (13 of 64) with RV enlargement. Mortality was 14% (2 of 14) with normal cardiac troponin I (cTnI), 19% (4 of 21) with intermediate cTnI, and 22% (8 of 36) with high cTnI (comparisons between groups nonsignificant [NS]). Trends with combinations of risk factors showed the highest mortality with shock plus high cTnI plus RV hypokinesis (57%) or shock plus high cTnI plus RV enlargement (54%). In conclusion, among the single risk factors, shock was associated with the highest in-hospital mortality from PE and combinations with high cTnI and RV enlargement were associated with higher mortalities.
In patients who are hemodynamically unstable from pulmonary embolism (PE), mortality may be as high as 58%. 1 The outcome of patients with massive PE has been associated with predictive factors including right ventricular (RV) enlargement, RV hypokinesis, and shock.1–4 To date however, in patients receiving thrombolytic therapy for PE, RV enlargement, RV hypokinesis, and shock have not been evaluated in combination with cardiac troponin I (cTnI). With this background in mind, we assessed the predictors of in-hospital mortality from PE in patients who received thrombolytic therapy.
Methods
This was a retrospective study of 78 patients hospitalized with massive PE who received thrombolytic therapy and either survived or died of PE. One patient had been eliminated because death was from hemorrhage due to thrombolytic therapy. Sixty-eight patients were hospitalized at William Beaumont Hospital, Royal Oak, Michigan, and William Beaumont Hospital, Troy, Michigan, from January 2004 through April 2010, and 10 patients were hospitalized at Saint Joseph Mercy Oakland Hospital, Pontiac, Michigan, from January 2000 to April 2010. Medical records, reports of imaging studies, and laboratory tests were reviewed. The investigation was approved by the Institutional Review Boards of both hospitals.
Right ventricular hypokinesis and RV enlargement on echocardiograms were assessed qualitatively. Echocardiograms were not reinterpreted for purposes of this investigation.
Cardiac troponin I was measured in 71 (91%) of 78 patients within 48 hours before or after the diagnosis of PE was made. Cardiac troponin I prior to October 2006 at the William Beaumont Hospitals was measured in 18 patients by Bayer Diagnostics TnI 2-site sandwich immunoassay using Siemens ADVIA Centaur TnL-Ultra, Deerfield, Illinois. Normal was <0.3 ng/mL, intermediate or indeterminate was 0.4 to 1.4 ng/mL, and high (highly suggestive of myocardial infarction or critical) was >1.5 ng/mL.
Cardiac troponin I after October 2006 at the William Beaumont Hospitals was measured in 44 patients by Bayer Diagnostics TnI UltraTM troponin 3-site sandwich immunoassay using Siemens ADVIA Centaur TnL-Ultra, Deerfield, Illinois. Most recent interpretation was normal ≤0.05 ng/mL, intermediate or indeterminate 0.06 to 0.19 ng/mL, and high (highly suggestive of myocardial infarction or critical) ≥0.20 ng/mL.
Cardiac troponin I at St. Joseph Mercy Oakland Hospital was measured in 9 patients by a 2-site immunoenzymatic (sandwich) assay (Access Immunoassay System, Beckman Coulter, Brea, California). Normal was <0.05 ng/mL, intermediate or indeterminate 0.05 to 0.49 ng/mL, and high (highly suggestive of myocardial infarction or critical) was ≥0.50 ng/mL.
Shock was defined as systolic blood pressure ≤90 mm Hg.
Statistical Analysis
Mortality was reported as in-hospital mortality due to PE in the opinion of the treating physicians. Chi-square test was used to assess the differences in categorical variables. InStat version 3.0 Graph Pad Software, San Diego, California, was used to calculate the 2-sided P values. Student t test was used to assess the differences in the means of continuous variables. Multivariate analysis was performed using Binary Logistic Regressions (SPSS version 11, Chicago, Illinois) to assess independent predictors of in-hospital mortality.
Results
Age of the patients was 60 ± 16 years (mean ± standard deviation); 53% were women. Echocardiograms were obtained in 75 (96%) of 78 patients. Right ventricular enlargement was reported in 85% (64 of 75), and RV hypokinesis was reported in 45% (34 of 75). Thirty-three patients were in shock.
Indications for thrombolytic therapy were shock (n = 35), respiratory failure requiring ventilator support (n = 12), RV enlargement or hypokinesis (n = 22), extensive or saddle PE (n = 6), and unknown in 3.
In-hospital mortality from PE in patients who received thrombolytic therapy was 19% (15 of 78). Mortality from PE was higher in those with shock, 36% (12 of 33) compared with 7% (3 of 45) without shock (P = .001).
Mortality from PE was 21% (7 of 34) with RV hypokinesis and 20% (13 of 64) with RV enlargement compared with 0% (0 of 11) in those with no RV enlargement and no RV hypokinesis (nonsignificant [NS]).
Mortality from PE was 14% (2 of 14) with normal cTnI, 19% (4 of 21) with intermediate cTnI, and 22% (8 of 36) with high levels of cTnI. Comparisons between groups were not significant.
Cardiac troponin I in patients who died was 2.7 ± 5.3 ng/mL (mean + standard deviation) compared with 0.8 ± 1.1 ng/mL among those who survived (P = .01).
Binary logistic regression showed that among the individual variables, only shock had an independent association with mortality (P = .01).
Trends based on various combinations of predictors of mortality are shown in Figure 1 . The mortality with shock plus high cTnI plus RV hypokinesis was 57% (4 of 7). Those with shock plus high cTnI plus RV enlargement had a PE mortality of 54% (7 of 13). Probabilities of differences in mortality with various combinations of predictors are shown in the legend of Figure 1.
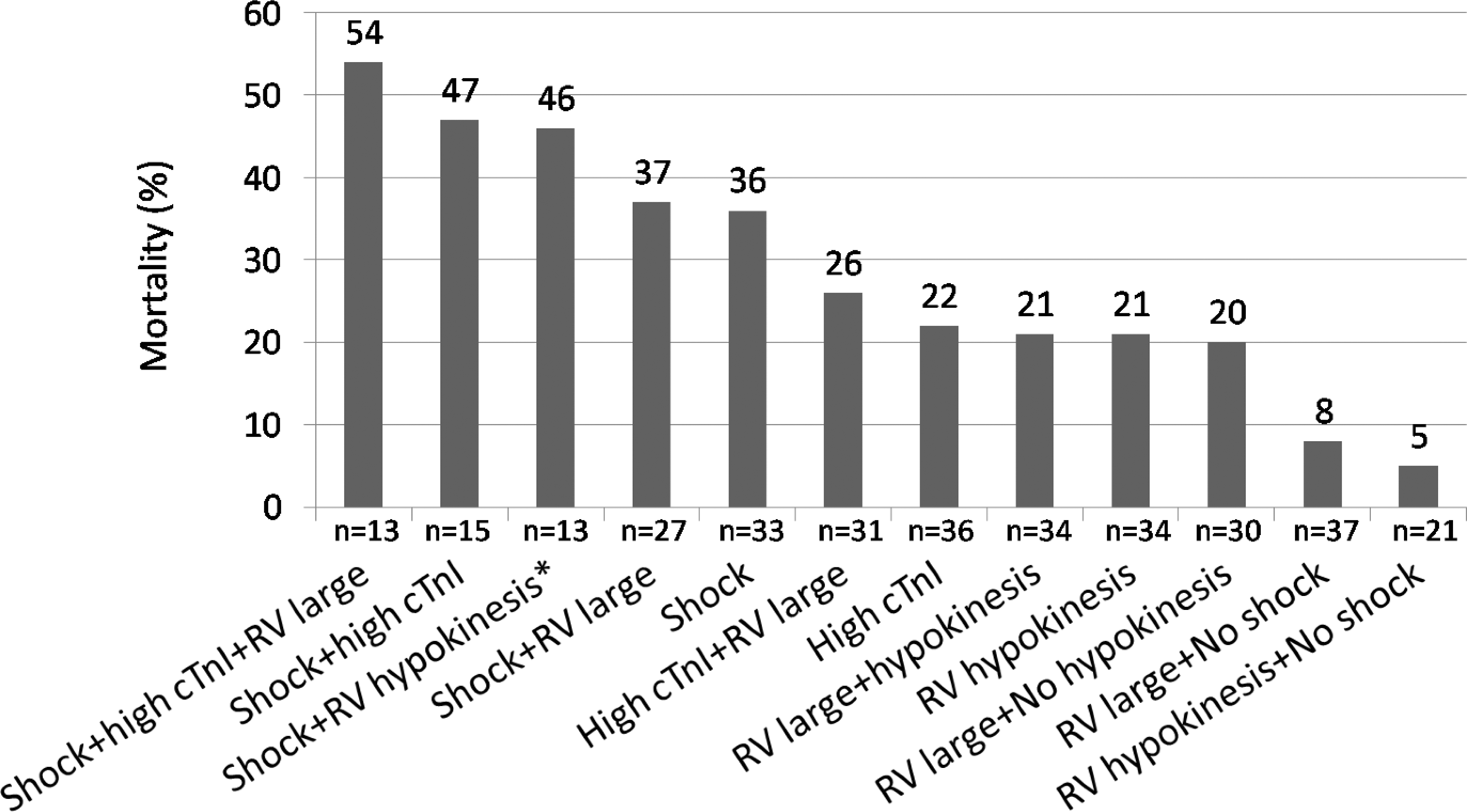
Mortality from pulmonary embolism (PE) in patients with combinations of risk factors.
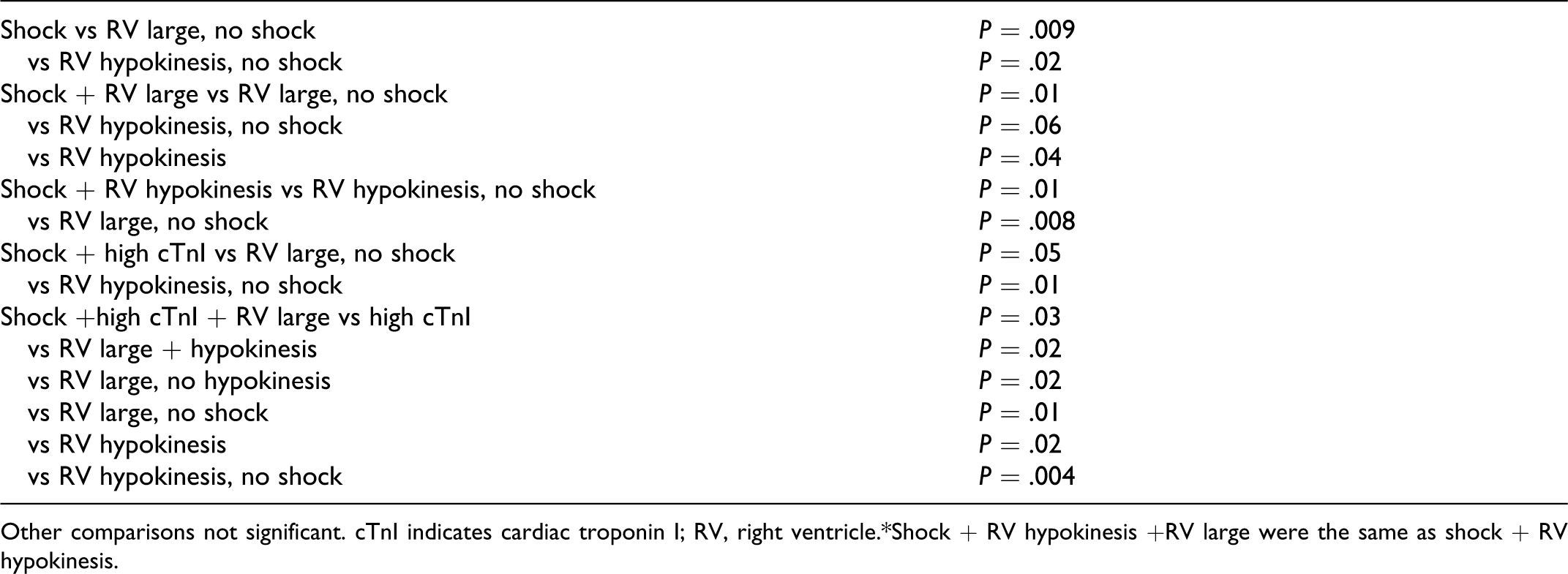
Other comparisons not significant. cTnI indicates cardiac troponin I; RV, right ventricle.*Shock + RV hypokinesis +RV large were the same as shock + RV hypokinesis.
Discussion
Shock was the only significant independent predictor of increased mortality in patients with PE who received thrombolytic therapy. Trends showed that the highest mortality from PE was in patients with shock plus high cTnI plus RV hypokinesis, 57% (4 of 7), followed by those with shock plus high cTnI plus RV enlargement, 54% (7 of 13).
The mortality from PE that we showed in patients who received thrombolytic therapy (19%) was similar to the mortality shown by Goldhaber et al (23%) in the International Cooperative Pulmonary Embolism Registry (ICOPER). 1 Others reported a mortality that ranged from 6% to 17%.3,5–8 Among patients in shock, Goldhaber et al reported a mortality of 58%, which was higher than we observed (36%). Podbregar et al showed 15% mortality from PE in the intensive care unit among patients with shock who received thrombolytic therapy. 2 Kasper et al showed 14% to 60% mortality from PE in patients with shock, depending on whether they required vasopressor therapy or cardiopulmonary resuscitation. 4 Multivariate analysis that included shock and RV hypokinesis showed that shock had a higher odds ratio for predicting mortality at 3 months. 1
Liu et al reported 5.8% in-hospital mortality from PE among patients who received thrombolytic therapy. 6 Independent risk factors for long-term mortality after thrombolytic therapy were pulmonary artery systolic pressure >50 mm Hg, RV dysfunction/dilatation, and >30% obstruction of the pulmonary vasculature shown on the lung scan. 6
Weaknesses of our study include the retrospective design, qualitative assessment of RV size and function, and different methods of measurement of cTnI in the participating hospitals.
A strength of this investigation is that it is the only investigation that includes cTnI in combination with RV enlargement, RV hypokinesis, and shock in the assessment of risk in patients who received thrombolytic therapy.
In conclusion, a trend suggests that among patients who received thrombolytic therapy for massive PE, those with shock plus high cTnI plus RV hypokinesis or shock plus high cTnI plus RV enlargement had the highest mortality.
Footnotes
The author(s) declared no conflicts of interest with respect to the authorship and/or publication of this article.
The author(s) received no financial support for the research and/or authorship of this article.