
Abstract
The presence of carotid atherosclerosis accompanied by coronary artery disease is associated with poor prognosis. A subset of patients who take aspirin continue to have recurrent cardiovascular events, which may be due to aspirin resistance (AR). Also, carotid plaques may cause turbulent flow which in turn may lead to platelet activation and poor antiplatelet response. In our study, we aimed to show the prevalence of AR and its relationship between high-risk carotid images in young patients with ST-segment elevated myocardial infarction (STEMI). In our study, we included 112 patients younger than 45 years with STEMI. Aspirin response test was evaluated 1 hour after aspirin intake using multiplate platelet function analyzer, and carotid ultrasonography has been performed to determine carotid intima–media thickness (CIMT) and the presence of carotid plaque. We identified 30.3% AR in young patients with STEMI. Carotid intima–media thickness (P = .002), carotid plaque (P = .012), and high-risk carotid image (P = .015) values are significantly high in patients who have AR. Independent of other risk factors, the presence of carotid plaque and being in the high-risk carotid group were associated with 3.7 times and 3.2 times increased odds for AR, respectively. In young patients with STEMI, physicians should be careful about AR, especially in patients who have carotid plaque and thicker CIMT.
Keywords
Introduction
Despite technological improvements, new drugs, and an increasing level of awareness, acute coronary syndrome (ACS) is considered to be the most important cause of death throughout the world, especially in Western countries. 1 In addition, younger age heart attacks are not uncommon in developing countries.
It has been found that aspirin treatment inhibits primary and secondary cardiovascular and cerebrovascular disease in approximately 1 of every 10 patients. 2 In patients with coronary artery disease (CAD), the antiplatelet therapy is recommended in European guidelines. 3 However, some patients do not have antiplatelet effect, and this is called clinical aspirin resistance (AR).
Increasing evidence suggests that AR has been shown at varying rates in patients who are at risk of atherothrombotic complications and who use aspirin. Kim et al showed that in individuals with CAD and ischemic stroke, AR rate was 14%. 4 In other studies, researchers found AR incidence was 53.3% for post-op patients who had off-pump coronary artery bypass surgery 5 and 29.9% for unstable angina pectoris patients. 6 Moreover, the reflection of this biochemically detected AR to cardiovascular adverse events has been found in different studies. 7 –9
Carotid intima–media thickness (CIMT), which is measured by B mode ultrasonography (USG), has been shown to be predictive in cardiac diseases and stroke by epidemiologic proofs. 10 Carotid artery monitoring and CIMT measurements have been used to show the degree of atherosclerosis in wide observational studies, and also many cross-sectional and social studies have found that CIMT increase and carotid plaque were related to the prevalence of cardiovascular diseases. 11 In addition, a history of both CAD and carotid artery disease had a higher immature platelet cells, suggesting that rapid platelet turnover may, in part, contribute to the heightened AR. Also, plaques formed in carotid arteries may cause turbulent flow which in turn may lead to platelet activation by increasing shear stress. This can lead to poor antiplatelet response.
Aspirin resistance has been studied in different groups of patients, and the factors affecting AR have been investigated several times. However, there are insufficient data about aspirin response in the younger Myocardial infarction group. As far as we see, no study evaluated the relationship between AR and carotid imaging. Consequently, the prevalence of AR and the relationship of AR with the thickness of the carotid intima media and the presence of carotid plaque will be assessed in our study of young patients with ST-elevated myocardial infarction (STEMI) who underwent primary percutaneous coronary intervention (PCI).
Materials and Methods
Study Participants
A total of 112 patients who came to the outpatient clinic after a mean of 18 months (14-22 months) after STEMI (mean age 39.6 ± 3.9) were included in the study. Patients with regular Acetylsalicylic acid (ASA) 75 to 150 mg medication use for at least 7 days were included in the study. Carotis USG and ambulatory blood pressure monitorization test were performed for patients who meet the inclusion criteria.
We excluded patients who have the following conditions: history of ACS within 6 months, history of hemorrhage, usage of Non steroidal anti-inflammatory drugs (NSAID), or any antiplatelet or anticoagulant except aspirin, previous treatment with glycoprotein IIb/IIIa inhibitors within 10 days, diagnosis of ACS in the last 6 months, active malignancy, chronic inflammatory conditions, hemorrhagic diathesis, thrombolytic treatment within the last month, liver disease, and platelet counts< 100 000/mm3.
Patients’ demographics, medical charts, and laboratory parameters were recorded. Patients who smoked within the previous month were regarded as smokers. Hypertension was accepted as systolic blood pressure (SBP) above 140 mm Hg and diastolic blood pressure (DBP) above 90 mm Hg or having used antihypertensive drugs for longer than 2 weeks. Hypercholesterolemia was accepted as a low-density lipoprotein (LDL) level above 130 mg/dL or usage of antihyperlipidemic drugs before primer PCI. Diabetes mellitus was accepted as fasting glucose level above 125 mg/dL or usage of antidiabetic drugs. Informed consent was taken from all patients, along with approval from the local ethical committee. The study is appropriate for the Helsinki Declaration.
Study Design
In this cross-sectional study, the study population was divided into 2 groups according to the presence of AR, responders (n = 78, mean age 39.4 ± 4.3) and nonresponders (n = 34, mean age 40.1 ± 3,8). All patients underwent carotid USG to quantify CIMT and the presence of plaques. Patients who had CIMT ≥0.9 mm and/or carotid plaques were classified as high-risk carotid profile according to the previous studies and 10,11 otherwise classified as a low-risk carotid profile. Besides, Carotid intima–media thickness and the presence of carotid plaque addressing increased AR were evaluated separately and together.
Evaluation of ASA Resistance
Whole blood aggregation was performed using the multiplate platelet function analyzer (Multiplate; Dynabarte GmbH, Munich, Germany), an impedance aggregometer that is based on the principle that activated platelets expose receptors on their surface that allow them to attach to artificial surfaces. After 1 hour of aspirin ingestion, whole blood samples were collected in test tubes containing hirudin (25 µg/mL) as an anticoagulant. Arachidonic acid was used as the aggregation agonist, and all samples were analyzed within 2 hours of collection. The incubation lasted 3 minutes, and the results were obtained after 6 minutes. The aggregation measured using this device is quantified as area under the curve, aggregation degree, and aggregation velocity. Platelet aggregation results were presented as aggregation unit (AU) × minute, and values over 300 AU × minute were accepted as AR. 12
Evaluation of Carotid Images
Carotid USG was performed in all patients for CIMT measurements and carotid plaque detection. The protocol approved by the American Society of Echocardiography and The Society of Vascular Medicine was used. 13 Ultrasonography was performed as the patients lay supine, neck extended, and chin opposing the other side. The scanning was performed by 1 vascular radiologist who is certificated for duplex scan procedures. Carotid arteries were measured by LOGIQ E9 ultrasound system (GE Healthcare, Milwaukee, Wisconsin) and 9 MHz wide-band linear transducer. All the measurements were performed from the right and left side of common carotid arteries 10 to 20 mm proximal of the carotid bifurcation. Carotid intima–media thickness was obtained by measuring between the medial–adventitial surface and luminal–intimal surface. The manual measurements were performed from 3 different places of the thickest ones, and the maximum values were obtained without including the plaques. The last CIMT values were obtained by calculating the means of right and left carotid arteries. All images were recorded at the same time with electrocardiography following 3 cardiac cycles, and the vision of the end-diastolic moment was used for CIMT measurement. Carotid plaque was defined as the increase in focal intima–media thickness more than 50% or CIMT >1.5 mm focally. Finally, the high-risk carotid profile (having plaques or CIMT ≥0.9 mm) and the low-risk carotid profiles were obtained in light of the findings of previous studies. 10,11
Ambulatory Blood Pressure Monitoring
The 24-hour ambulatory blood pressure monitoring (ABMP) measurement was performed using a portable compact digital recorder (Tonoport V; GE Healthcare, Milwaukee, Wisconsin) and an analyzer using customized analytical software programmed to measure blood pressures at 30-minute intervals, from 07:00 until 23:00, and at 60-minute intervals from 23:00 until 07:00. Daytime was defined as the time between the hours of 07:00 and 23:00, and nighttime was defined as the time between the hours of 23:00 and 07:00. The patients were instructed to perform their usual daily activities but to stay inactive during the measurements. Recordings were accepted if more than 80% of the raw data were valid. Nondippers were defined as those with a nocturnal decrease in SBP of <10% compared to daytime, and dippers were defined as those with a 10% or larger decline in SBP during the nocturnal period of diurnal blood pressure. 14
Statistical Analysis
Continuous variables are presented as means and standard deviations (SDs). The categorical variables are expressed as numbers and percentages. One-way analysis of variance or Kruskal-Wallis test was used for comparisons as appropriate. Bonferroni correction was employed to adjust for multiple comparisons. Categorical data were compared with a χ2 test. For predicting AR-independent risk factors, logistic regression was used. A P value <.10 was employed for potential variable selection in multivariate analysis. Nagelkerke r2 values for logistic regression were recorded. Receiver–operating characteristics (ROC) curves for CIMT to distinguish AR were drawn. Youden index was used to derive the best cutoffs. The area under the ROC curves (AUC) was recorded. P values below .05 were considered statistically significant. Statistical analyses were performed using the SPSS software version 18.0 for Windows (SPSS Inc, Chicago, Illinois).
Results
After excluding inappropriate cases, a total of 112 patients were included. One of the authors received information about drug use by talking face-to-face with patients who underwent successful primary PCI. The prevalence of AR was 30.3%. Other than hematocrit, creatinine level, and platelet aggregation results, the baseline characteristics between the 2 groups did not differ (Table 1). In ambulatory blood pressure measurement test, mean SBP, daytime SBP, night SBP, and night DBP were statistically higher in the AR group (Table 2).
Baseline Characteristics of Study Population.a
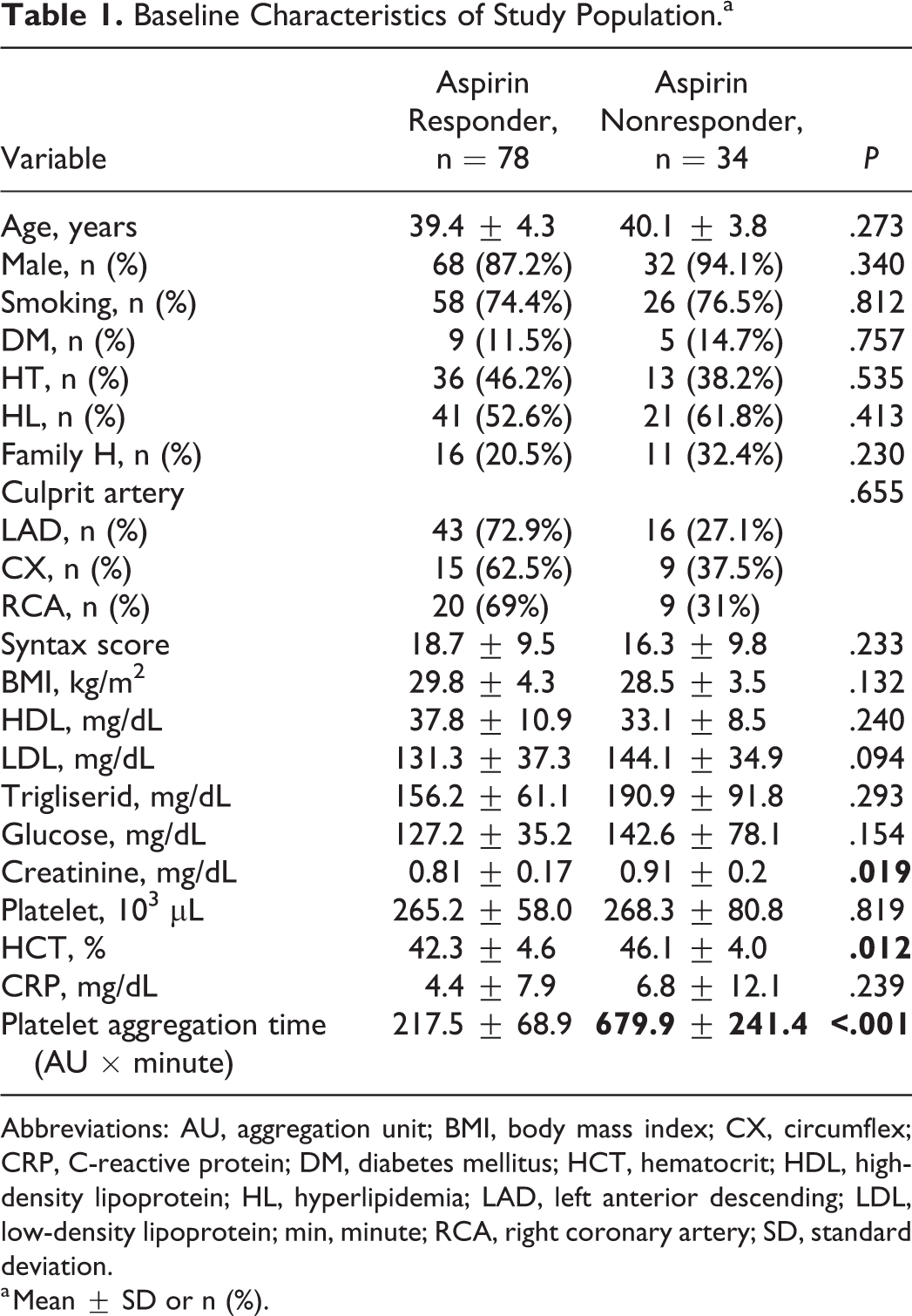
Abbreviations: AU, aggregation unit; BMI, body mass index; CX, circumflex; CRP, C-reactive protein; DM, diabetes mellitus; HCT, hematocrit; HDL, high-density lipoprotein; HL, hyperlipidemia; LAD, left anterior descending; LDL, low-density lipoprotein; min, minute; RCA, right coronary artery; SD, standard deviation.
a Mean ± SD or n (%).
Comparison of Ambulatory Blood Pressure Measurements According to the Presence of Aspirin Resistance.a
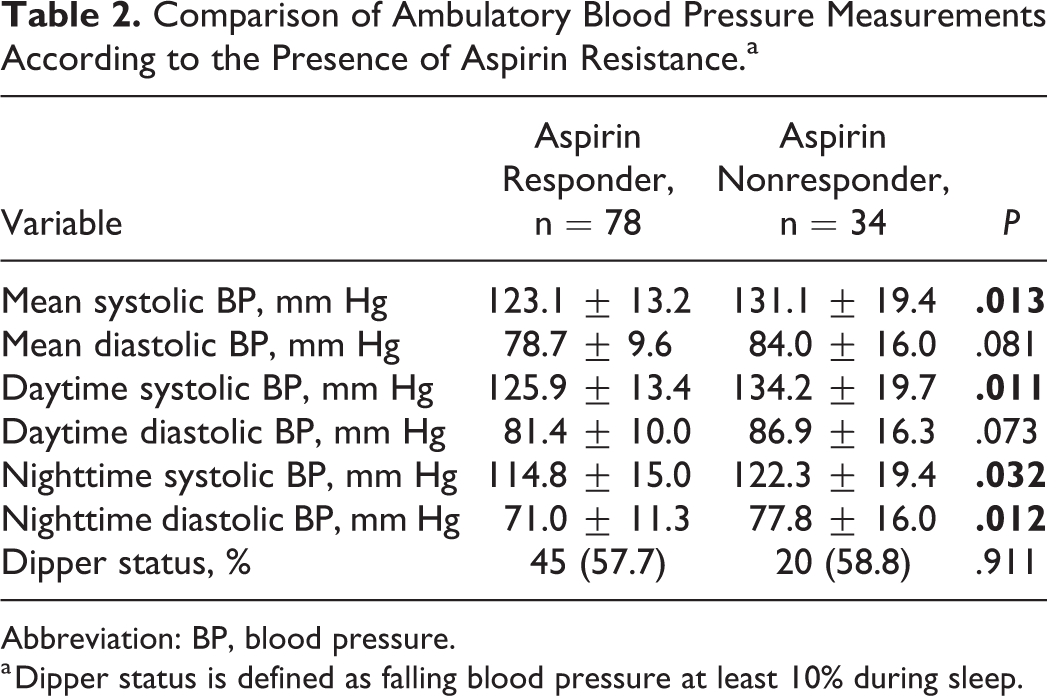
Abbreviation: BP, blood pressure.
a Dipper status is defined as falling blood pressure at least 10% during sleep.
Patients in AR group had a 19.7% increased CIMT compared to patients in responder group. Parallel to that, the high-risk carotid profile was 2.5 times prevalent in AR group compared to another one (Figure 1).
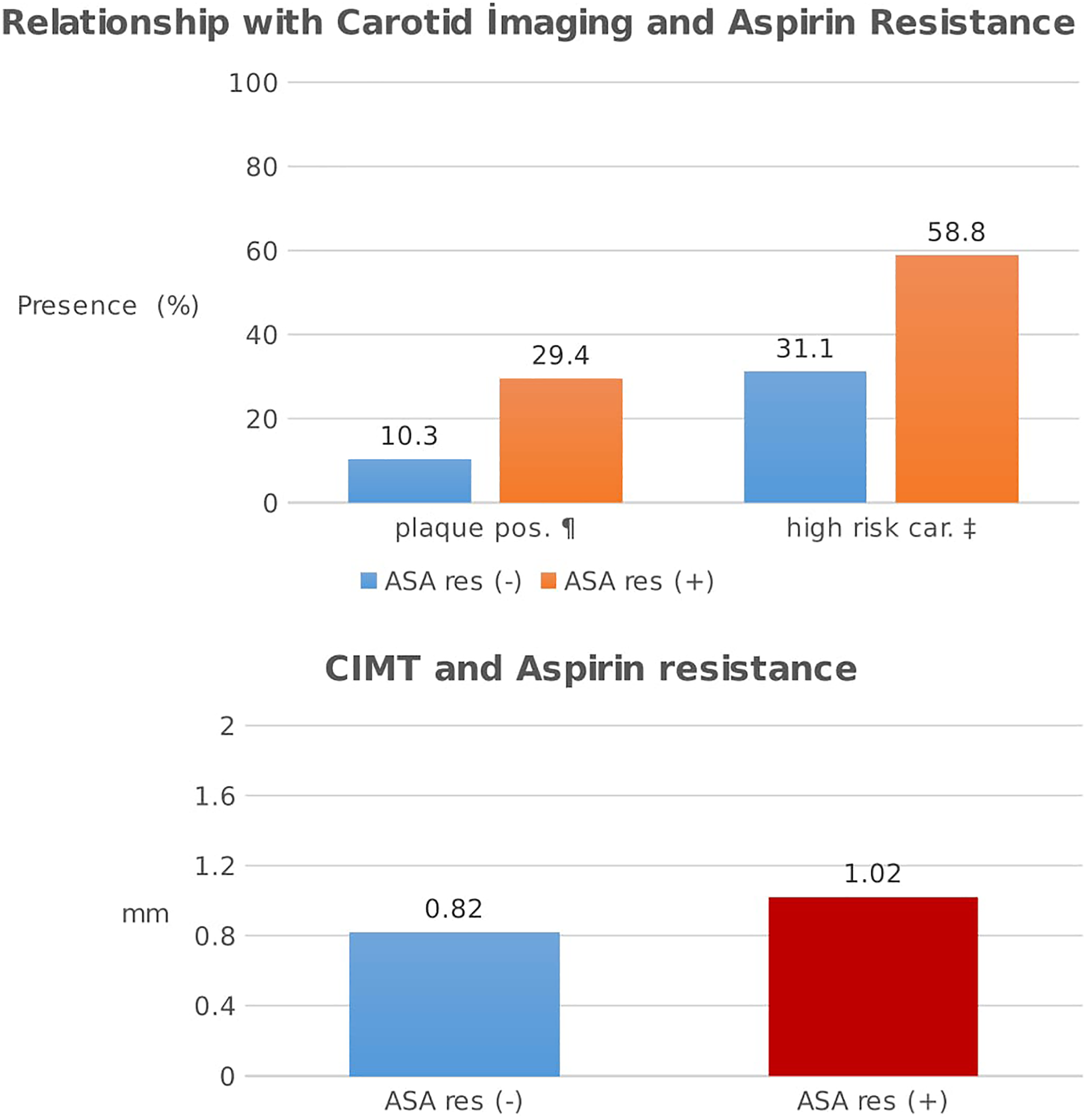
Bar graph showing the mean carotid intima–media thicknesses, plaque positivity, and high-risk carotid image presence in the groups according to aspirin response. High-risk carotid image is defined as plaque positivity and/or CIMT ≥0.9 mm. car denotes carotid images; CIMT, carotid intima–media thickness; mm, milimeter; OR, odds ratio; pos, positivity; res, resistance. ¶Aspirin resistance in patients with plaque positivity, OR: 3.646 (1.090-10.343). ‡Aspirin resistance in patients with high-risk carotid image, OR: 3.029 (1.318-6.961).
Independent from other risk factors, 1-mm increase in CIMT was associated with 25% increased odds for AR. In addition, presence of carotid plaque was associated with 3.7 times increased odds for AR. When the high-risk carotid imaging, consisting of the combination of two parameters mentioned above, was investigated to be an independent predictor of AR, high-risk carotid images were found to increase AR by 3.2 times compared to low-risk carotid patients (Table 3). Furthermore, a CIMT cutoff ≥0.8 mm had AUC of 0.688 for distinguishing AR with a 70.5% sensitivity and 57.6% specificity showed in ROC analysis (Figure 2).
Multivariate Logistic Regression Analysis for Potential Predictors of Aspirin Resistance.a
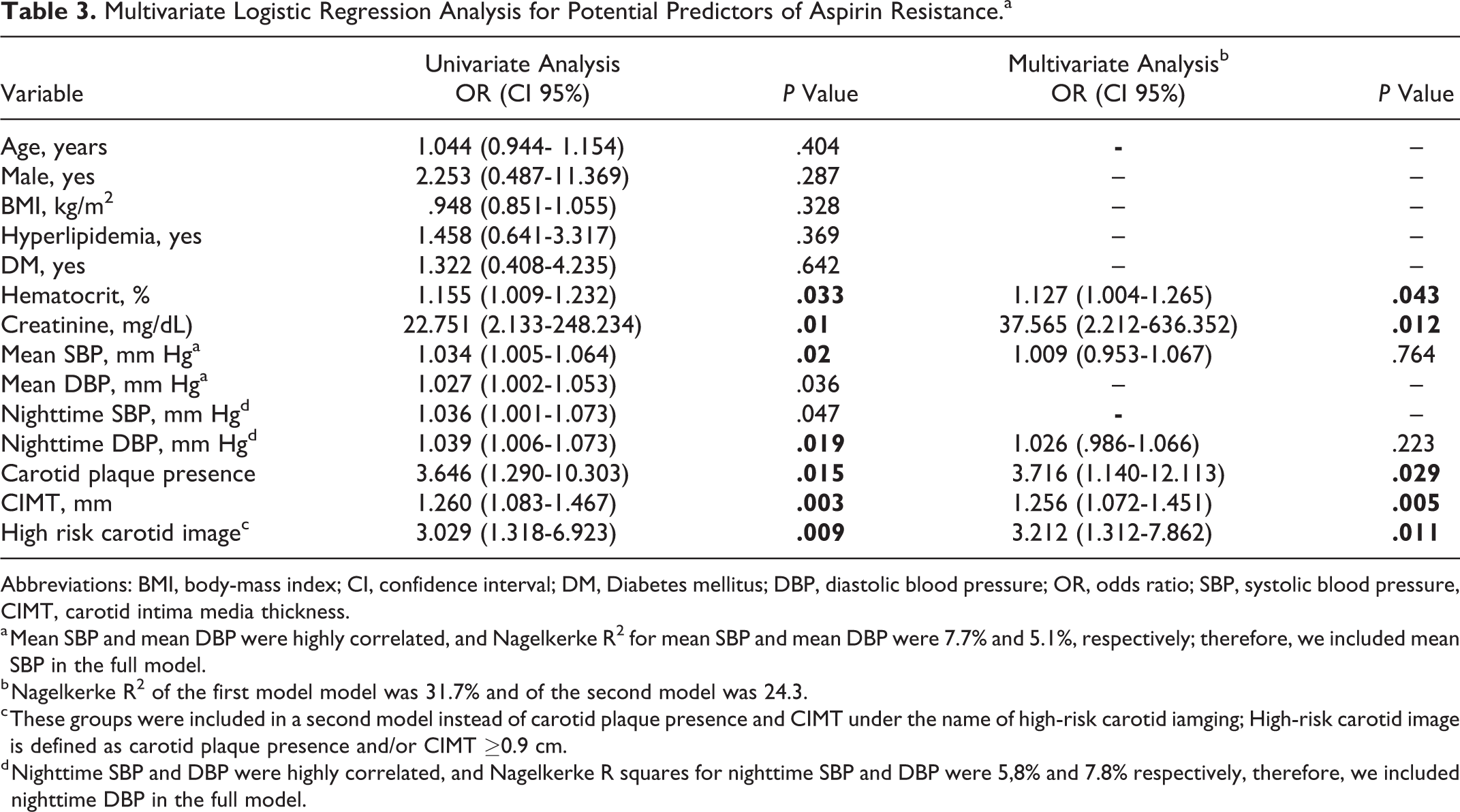
Abbreviations: BMI, body-mass index; CI, confidence interval; DM, Diabetes mellitus; DBP, diastolic blood pressure; OR, odds ratio; SBP, systolic blood pressure, CIMT, carotid intima media thickness.
a Mean SBP and mean DBP were highly correlated, and Nagelkerke R2 for mean SBP and mean DBP were 7.7% and 5.1%, respectively; therefore, we included mean SBP in the full model.
b Nagelkerke R2 of the first model model was 31.7% and of the second model was 24.3.
c These groups were included in a second model instead of carotid plaque presence and CIMT under the name of high-risk carotid iamging; High-risk carotid image is defined as carotid plaque presence and/or CIMT ≥0.9 cm.
d Nighttime SBP and DBP were highly correlated, and Nagelkerke R squares for nighttime SBP and DBP were 5,8% and 7.8% respectively, therefore, we included nighttime DBP in the full model.
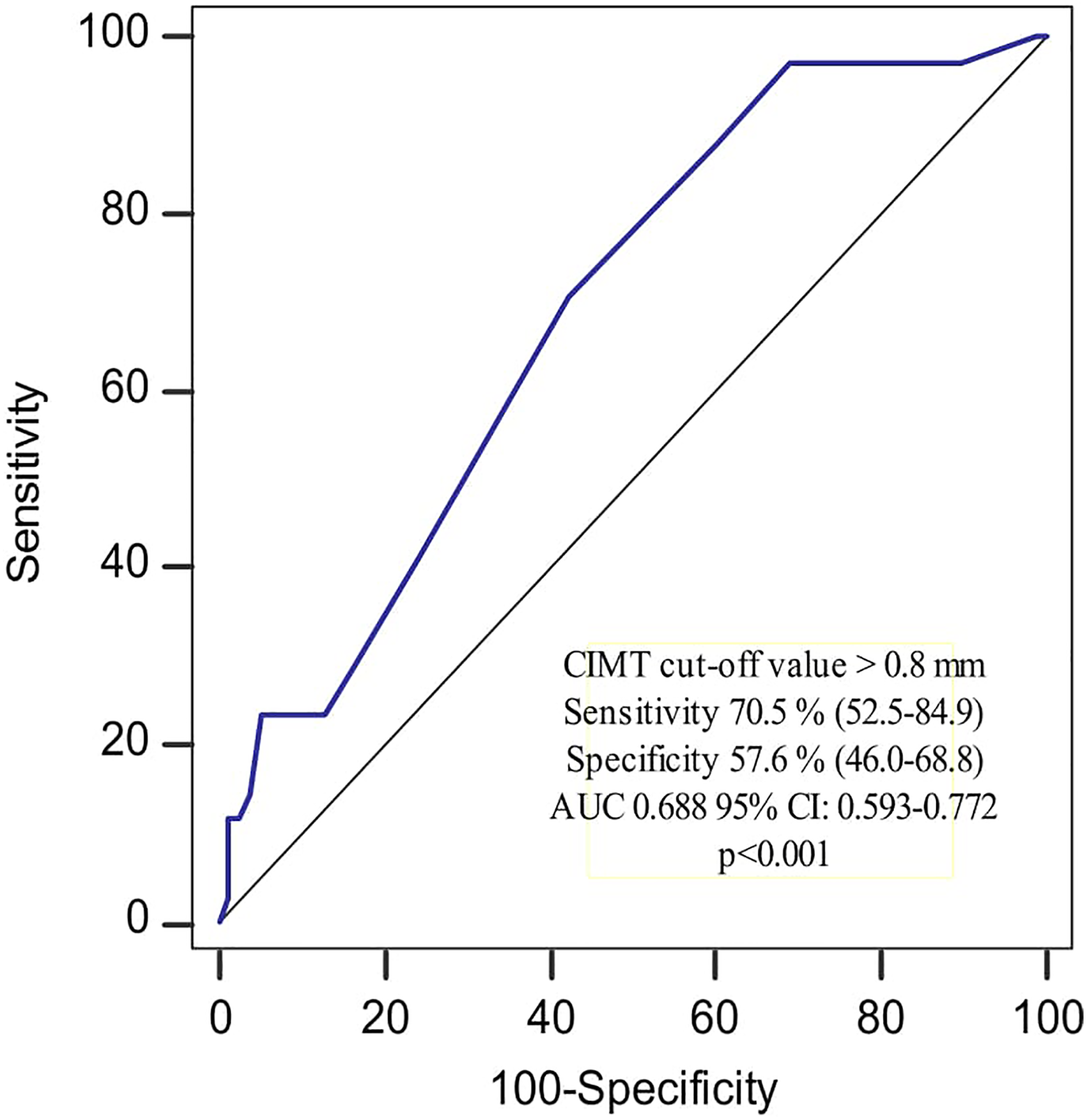
Receiver–operating characteristics curve showing the distinguishing ability of CIMT for the presence of aspirin resistance. AUC denotes area under the ROC curve; CI, confidence interval; CIMT, carotid intima media thickness; ROC, receiver-operating characteristics.
Discussion
In our study, AR was detected in 30.3% of young patients with STEMI. When the patients were divided into 2 groups according to the presence of AR, patients with AR showed a statistically significant increase in CIMT and carotid plaque presence. In regression analysis, hematocrit and creatinine level as well as high-risk carotid image which is the combination of CIMT and carotid plaque presence were found to be independent predictors for AR in young patients with STEMI.
Aspirin resistance is a multifactorial phenomenon that has been studied in many different populations with different methods. Therefore, the presence of variable results in the literature makes it difficult to compare our results with those of other studies. However, the absence of any previous studies in young patients with STEMI and an association between AR and carotid imaging makes this study unique and valuable.
Young patients with STEMI were enrolled in our study, with single-vessel underwent primary percutaneous intervention, and without lesions on other vessels. In general, young patients with STEMI mostly have a single vascular disease caused by plaque rupture rather than widespread vascular disease. In this study, we aimed to investigate whether carotid arteriosclerosis is associated with poor response to aspirin in young patients with STEMI; thus, we aimed to compare AR in young patients with only coronary artery disease and with both coronary and carotid artery disease.
There is no single way to initiate thrombotic events; therefore, inhibition of a single receptor does not prevent all thrombotic complications. In addition, in some patients, the sensitivity of aspirin is low, resulting in clinical complications. In a meta-analysis of 1813 patients with 12 studies examining the effect of AR on prognosis, the mean biochemical AR was reported as 27%, and major adverse cardiovascular events were found to be odds ratio 3.8 (95% confidence interval [CI]: 2.3-6.1) in patients with AR. 7 In another meta-analysis of 2930 patients, AR was detected in 28% of patients, and in AR patients, 41% had cardiovascular events (OR 3.85, 95% CI: 3.08-4.80), 5.7% had mortality (OR 5.99, 95% CI: 2.28-15.72), and 39.4% had ACS (OR 4.06, 95% CI: 2.96-5.56). 8 In another study on patients with symptomatic peripheral artery disease, AR was found as an independent predictor of adverse cardiovascular events with 2.48 hazard ratio. 9 Since our study was not planned in a prospective manner, the prognostic assessment was not performed in patients with AR. However, similar to the above mentioned studies, we found that 30.3% of our patients were resistant to aspirin. From the above-mentioned meta-analyses, it can be speculated that patients with AR are at a higher risk of future adverse cardiovascular events for our study too. In addition, long-lasting aspirin treatment is required in young patients with MI who constitute the population of our study; that is why AR is even more important in terms of major adverse cardiovascular events.
Several possible causes are evident in the formation of AR. These include variability in aspirin blood flow, irregular drug use, inadequate dosing, associated NSAID withdrawal, variability in platelet function, accelerated platelet turnover, increased sensitivity of arachidonic acid and collagen, cyclooxygenase and glycoprotein 2b/3a polymorphism, and interactions of platelets with other blood cells or cell-derived products. Aspirin resistance may not only be due to platelet-poor inhibition but also be due to the inadequate direct effect of aspirin on the endothelium. Besides, a weak effect on the platelet may be related to endothelial dysfunction and oxidative stress. In parallel with these hypotheses, in a study of young healthy individuals, AR was found more frequently in patients with endothelial dysfunction demonstrated by flow-mediated vasodilatation. 15 Moreover, it was found that CIMT referred hypertensive medial hypertrophy and reflected as an adaption to blood flow and wall tension 13 which may be associated with endothelial dysfunction and oxidative stress. Another important hypothesis is that turbulent flow occurs due to atherosclerotic plaques, and this leads to increased shear stress and platelet activation. As a result, the processes in the formation of carotid plaques and increase in CIMT may be similar to the process leading to AR. Confirming with this, Lewzsuk et al. found a possible coexistence of unstable plaques and resistance to aspirin in patients undergoing carotid endarterectomy. 16 In a different population—young patients with MI —we established a hypothesis similar to the one above and investigated a relationship between carotid plaques presence, increased the thickness of the carotid intima media, and AR. Consequently, in our study, we have shown that the presence of high-risk carotid imaging which consists CIMT increase and/or carotid plaque presence is a sign of the presence of AR in younger patients with MI.
There are contradictory studies on the relation of aspirin with hypertension in the literature. In 2 separate studies—in newly diagnosed patients and patients with chronic hypertension—there was no relationship between AR and hypertension, 17,18 whereas the presence of hypertension in patients with stable coronary artery was found as predictive of AR. 19 In our study, ABPM was performed in all patients, and mean/daytime/nighttime SBP and night time DBP was higher in patients with AR. However, none of them was considered one of the independent predictors of AR.
Other factors that may affect ASA resistance were also studied. Similar to many studies, we found no relationship between AR and the sex of patients. We have also not found any relationship between age and AR as shown in most of the studies. 20 Similar to Zytkiewicz et al, 21 we did not find a relationship between increased body mass index and AR. However, in some studies, it has been found that AR is higher in obese individuals. 22,23 A significant portion of the studies has established a relationship between AR and whole blood. 24,25 In our study, hematocrit was statistically significantly higher in the ASA-resistant group but not in the white blood cell and platelet counts. In many studies, the relationship between chronic renal failure and AR has been established. 26,27 We also found that the creatinine level was one of the independent predictors of AR (OR: 37.565; 95% CI: 2.21-636.35; P = .012). In vivo and in vitro studies have shown the effect of hyperlipidemia on AR. 28 It is assumed that the increase in cholesterol deposition on the platelet membrane may reduce membrane permeability, which may cause AR. 29 It has also been found that there may be a decrease in the resistance to aspirin with statin therapy. 30,31 In our study, more AR was detected in patients with hyperlipidemia, but no significant difference was found. A significant proportion (87.4%) of patients using statin therapy were considered to be one of the possible causes of this situation. In addition, patients with AR were found to have higher LDL and lower high-density lipoprotein, but no statistically significant difference was found.
Biochemical AR can be shown by inhibiting the production of thromboxane A2 from platelet, indicating that thromboxane production is reduced in vitro. Several laboratory methods have been used to detect platelet function and AR. Clinical utility of the multiplate analyzer test used in our study was shown in different patient groups. 32,33 In different cardiovascular diseases, AR has been reported to be 5% to 45%, and parallel to this, rates of 15% to 40% have been found in whole blood studies. 34 In our study, the whole blood method was used, and the AR was 30.3% in patients with MI younger than 45 years. Moreover, it has been shown that there is a decrease in the platelet aggregation degree after 48 hours compared to the value at the time of the event, 35 and the C-reactive protein value after ACS is an independent predictor of AR. 36 In the light of these studies, we can assume that the aspirin response test may be more valuable when there is less inflammation. In our study, this information was taken into consideration and the test was applied in stable patients after approximately 18 months after STEMI .
Could it be possible to overcome AR by increasing the dose of medicine in our patient group? In some trials, increasing the dose of aspirin has allowed some reduction in AR rates, but no dose in 5% to 10% of patients is sufficient to overcome AR. In addition, gastrointestinal hemorrhage and other side effects may increase when the dose is increased in these patients. In addition, high doses of aspirin can reduce the production of prostacyclin, an important vasodilator and endogenous antiplatelet, by inhibiting Cyclooxygenase2. For these reasons, it is open to investigating whether high-dose aspirin is beneficial in patients with AR in young patients with MI.
Study Limitations
This study has some limitations. First of all, this study was carried out in a single-centered and relatively small group. In addition, there are no long-term results in our study. This has prevented us from reaching clinical evidence of how the presence of biochemical AR will result. Another limitation is that, in the literature it was stated that more than one measurement of aspirin sensitivity test more reliable, but in our study, it was measured once. Furthermore, when heterogeneous results of different studies are considered, the use of a single laboratory method constitutes one of the important limits of the study. However, the multiple platelet function analysis method reduces the risk of laboratory errors because it is faster, less troublesome, and does not require specific preparation than conventional optical aggregometry. Finally, aspirin serum levels were not measured, but the medical history was taken by interviewing patients in a one-to-one correspondence and patients with irregular aspirin uptake were excluded from the study.
Conclusion
Although there are many studies in the literature on different groups of AR, many questions still remain unanswered. There is still no consensus on the definition, cause, risk factors, and clinical manifestation of AR. In our study, we found AR in a significant proportion (30.3%) in young patients with MI, and we have shown that this risk increases in patients with high-risk carotid images formed increased CIMT thickness and/or carotid plaque presence. As these group of patients are expected to use lifelong aspirin and are candidates for poor cardiovascular events, if we can not reach the AR test, we can make an assumption about the likelihood of AR by carotid USG in the light of the findings of our study. If we detect an increase in CIMT and/or carotid plaque, we may need to monitor these patients more closely and reexamine their antiplatelet therapy.
Footnotes
Acknowledgments
We are really grateful to biostatistics and biochemistry department of Mehmet Akif Ersoy Thoracic and Cardiovascular Surgery Center, Training and Research Hospital for giving the study such attention and time.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.