
Abstract
Background:
The slow coronary flow (SCF) is characterized by angiographically normal or near-normal coronary arteries with delayed progression of the contrast agent into distal vasculature. We aimed to investigate neutrophil-to-lymphocyte (N/L) ratio and the carotid intima-media thickness (CIMT) value in patients with SCF compared to patients with newly diagnosed coronary artery disease (CAD) and normal patients.
Materials and Methods:
We enrolled 60 consecutive patients with SCF, 68 patients with CAD, and 72 normal patients. The association between thrombolysis in myocardial infarction frame count, CIMT, and N/L ratio and other clinical and laboratory parameters were evaluated.
Results:
The N/L ratio was significantly higher not only in patients with SCF but also in patients with CAD, compared to those of controls. The N/L ratio was positively and moderately correlated with CIMT in the whole study population.
Conclusions:
The NL ratio is significantly associated with reduced coronary blood flow, and elevated N/L ratio might be an independent predictor for the presence of SCF.
Introduction
The slow coronary flow (SCF) phenomenon is an angiographic definition, which is characterized by angiographically normal or near-normal coronary arteries with delayed progression of the contrast agent into distal vasculature. It was first reported in 1972 by Tambe. 1 Etiopathogenesis of SCF is not exactly known. Several studies have investigated the relationship between coronary slow flow and endothelial dysfunction as a probable etiology. On the other hand, upon intravascular ultrasonography investigation, the common finding was longitudinally extended to massive calcification throughout the epicardial coronary arteries in most of the patients with SCF. These results support the theory that SCF is the result of coronary atherosclerosis, which is a part of systemic involvement. 2
Carotid intima-media thickness (CIMT) is a marker of systemic inflammation, and it is widely used as a prominent marker for cardiovascular diseases. 3 Among several atherosclerotic surrogates, increased CIMT was positively related to coronary artery severity and cardiovascular event; therefore, it was regarded as an early indicator of overall atherosclerosis. On the other hand, CIMT was significantly increased in patients with SCF than in controls. Besides, CIMT was significantly correlated with coronary intima-media thickness (IMT). Thrombolysis in myocardial infarction (TIMI) frame counts (TFCs) were positively correlated with CIMT and coronary intimal thickness. 2
The total white blood cell (WBC) count and its subtypes, neutrophil-to-lymphocyte (N/L) ratio, can be an indicator of systemic inflammation. 4 The N/L ratio has also been demonstrated to have the greatest predictive power for death, myocardial infarction, and high risk of coronary artery disease (CAD). 5 High N/L ratio is independently related to increased cardiovascular events. These findings were supported by other studies. 6,7 In patients submitted to angioplasty, N/L ratio is an independent predictor for long-term mortality. 8 These studies have shown a possible relationship between N/L ratio and systemic inflammation.
To the best of our knowledge, there is no study regarding the assessment of N/L ratio and CIMT in patients with SCF in the English literature. From that point of view, we aimed to evaluate the levels of N/L ratio in patients with SCF and compare it to patients with CAD and normal control patients. We also investigated the relationship between CIMT and N/L ratio based on the inflammatory activity.
Materials and Methods
Patients Selection
Between January 2010 and August 2012, 204 patients undergoing coronary angiography were enrolled into the study. They were divided into 3 groups. The SCF group consisted of 60 patients (33 men; mean age, 48.76 ± 4.97 years). The diagnosis of SCF was based on TFC. The CAD group consisted of 68 patients (36 men, mean age; 50.70 ± 6.17 years) with newly diagnosed CAD (at least stenotic lesions ≥ 50%). The control group consisted of 72 age- and sex-matched individuals (41 men; mean age, 50.47 ± 7.73 years) who were selected from the patients with angiographically normal coronary arteries during the same study period. The indication for coronary angiography was either the presence of typical angina or the positive or equivocal results of noninvasive screening tests for myocardial ischemia in all the groups. The institutional ethics committee approved the study protocol, and the study was conducted in accordance with the Declaration of Helsinki. All patients were evaluated by detailed medical history, physical examination, and biochemical analysis. Special emphasis was put on cardiovascular risk factors and diseases. All patients were questioned for any cardiovascular drug use, smoking habit, and alcohol consumption and underwent transthoracic echocardiography for structural heart disease. Image acquisition was performed in the left lateral decubitus position position using a Philips iE33 (6.0; Philips, Andover, Massachusetts) equipped with a 2.5-MHz transducer.
Exclusion criteria were defined as refusal to participate in the study, uncontrolled arterial hypertension, presence of anemia, uncontrolled diabetes mellitus, malignancy, left ventricular dysfunction (left ventricular ejection fraction <50%) or hypertrophy, acute coronary syndromes, valvular heart disease, congenital heart disease, any abnormality in thyroid function tests, renal or hepatic dysfunction (creatinine > 1.5 mg/dL, aspartate aminotransferase and alanine transaminase more than twice the upper limit of normal, respectively), local or systemic infection, previous history of infection (<3 months), inflammatory diseases, and any medication that can potentially interfere with measurement of N/L ratio. Also, erythrocyte sedimentation rate, WBC count, and fibrinogen levels were normal in the 3 groups.
Cardiac Catheterization and Documentation of TFC
Coronary angiograms were performed with a femoral approach using the Judkins technique without the use of nitroglycerin, adenosine, or a calcium channel blocker. All patients in the study population underwent elective coronary artery angiography using Siemens Axiom Artis DFC (Siemens Medical Solutions, Erlangen, Germany) following appropriate patient preparation. Injection of contrast medium (Iopromide, Ultravist-370; Schering AG, Berlin, Germany) was carried out by an automatic injector, at a speed of 3 to 4 mL/s for left coronary artery and 2 to 3 mL/s for right coronary arteriographies which were recorded at a speed of 25 frames/s. All angiograms were evaluated by 2 experienced physicians who were blind to the study using the corrected TFC method. The first frame was defined by a column of contrast extending across >70% of the arterial lumen anterograde motion. 9 The normal frame counts for the left anterior descending (LAD) coronary artery is 36 ± 2.3 frames, and the mean for the left circumflex coronary artery is 22.2 ± 3.8 frames. Hence, the longer LAD frame counts are corrected by dividing by 1.7 to derive the corrected TFC as described earlier. The normal frame counts for the corrected LAD coronary artery was 21.1 ± 1.3 frames. The right coronary artery is 21.7 ± 2.8 frames. 9
Coronary angiograms were judged with regard to smooth appearance, luminal wall irregularities, epicardial local or diffuse caliber reduction, and stenosis. Coronary arteries were classified as normal on the basis of visual assessment of the absence of any luminal irregularities. To exclude the possibility of coronary artery vasospasm, during coronary arteriography in patients with normal coronary artery underwent a hyperventilation test, which was performed by asking the patients to breathe quickly and deeply for 5 minutes.
Definition of SCF
All patients with a corrected TFC greater than 2 standard deviations from the normal published range for the particular vessel were accepted as having SCF, while those whose corrected TFC fell within the standard deviation of the published normal range were considered to have normal coronary flow. 10 After assessment of coronary flow in the coronary arteries using the corrected TFC method, the mean corrected TFC, which is the mean value of the frame count in the LAD, left circumflex coronary artery, and right coronary artery, was obtained from the patients with SCF. Intra- and interobserver variability for TFC was 0.966 and 0.943, respectively.
Biochemical Measurements
Blood samples were drawn without stasis at 7 to 8 o'clock in the morning after 20 minutes of supine rest, following a fasting period of 12 hours. Total plasma cholesterol, triglyceride, and high-density lipoprotein cholesterol were measured by an enzymatic calorimetric method with the Olympus AU 600 autoanalyzer using reagent from Olympus Diagnostics GmbH (Hamburg, Germany). Low-density lipoprotein cholesterol levels were calculated by Friedwald formula. Blood glucose was measured by the glucose oxidase method. A fasting peripheral venous blood sample was obtained from all patients in 3 groups for the measurement of N/L ratio. These blood samples were analyzed within 2 hours after vein puncture using Abbott Cell-Dyne 4000 cell counter (Abbott Laboratories, Abbott Park, Illinois). Hematological parameters, including hemoglobin, WBC count, and platelet count, were also analyzed by standard methods.
Carotid Ultrasonography
All patients were evaluated by high-resolution ultrasound using the Philips iE33 (6.0; Philips) equipped with a L 11-3 broadband linear array transducer. The transducer was manipulated so that the near and far walls of the common carotid artery (CCA) were parallel to the transducer footprint, and the lumen diameter was maximized in the longitudinal plane. A region 1 cm proximal to the carotid bifurcation was identified, and the CIMT of the far wall was evaluated as the distance between the lumen–intima interface and the media–adventitia interface. The CIMT measurement was obtained from 4 contiguous sites at 1-mm intervals, and the average of the 4 measurements was used for the analyses. Then, the measurements were taken from both right and left CCA, the average of both the values was calculated. All measurements were made manually on still images obtained during the sonographic scanning. The carotid plaques were excluded while measuring IMT. The intraobserver variability of ultrasonographic measurements was <7%, and all examinations were performed by a single experienced examiner who was blinded to the clinical and biochemical data.
Statistical Analyses
Continuous variables were given as mean
Results
The main characteristics of the study population are given in Table 1. Age, body mass index, lipid profiles, and fasting levels of glucose were not different between the 3 groups. Laboratory characteristics of all the groups were not statistically significant (Table 1). The leukocyte counts were not significantly different among the 3 groups (Table 2). There was not any significant difference in N/L ratios between SCF group and CAD group (P = .409; Figure 1). The N/L ratio was significantly higher in patients in both the SCF and the CAD groups, compared to the control group (P < .01; Figure 1). There was no significant difference in the CIMT levels between SCF group and CAD group (P = .355; Figure 2). The CIMT levels were also significantly higher in patients in both the SCF and the CAD groups, compared to the control group (P < .01; Figure 2). On the other hand, it was found that TFC for each major epicardial coronary artery was significantly higher in SCF group compared to both CAD and control groups (Table 1; P < .01). Significant positive correlations were detected between CIMT and N/L ratio (P < .01, r = .865; Figure 3). However, we found no significant correlation between CIMT or N/L ratio and mean TFCs.
The Comparison of Baseline Demographic, Clinical, Biochemichal, Platelet Activation Parameters, and TIMI Frame Counts of All the Groups.a
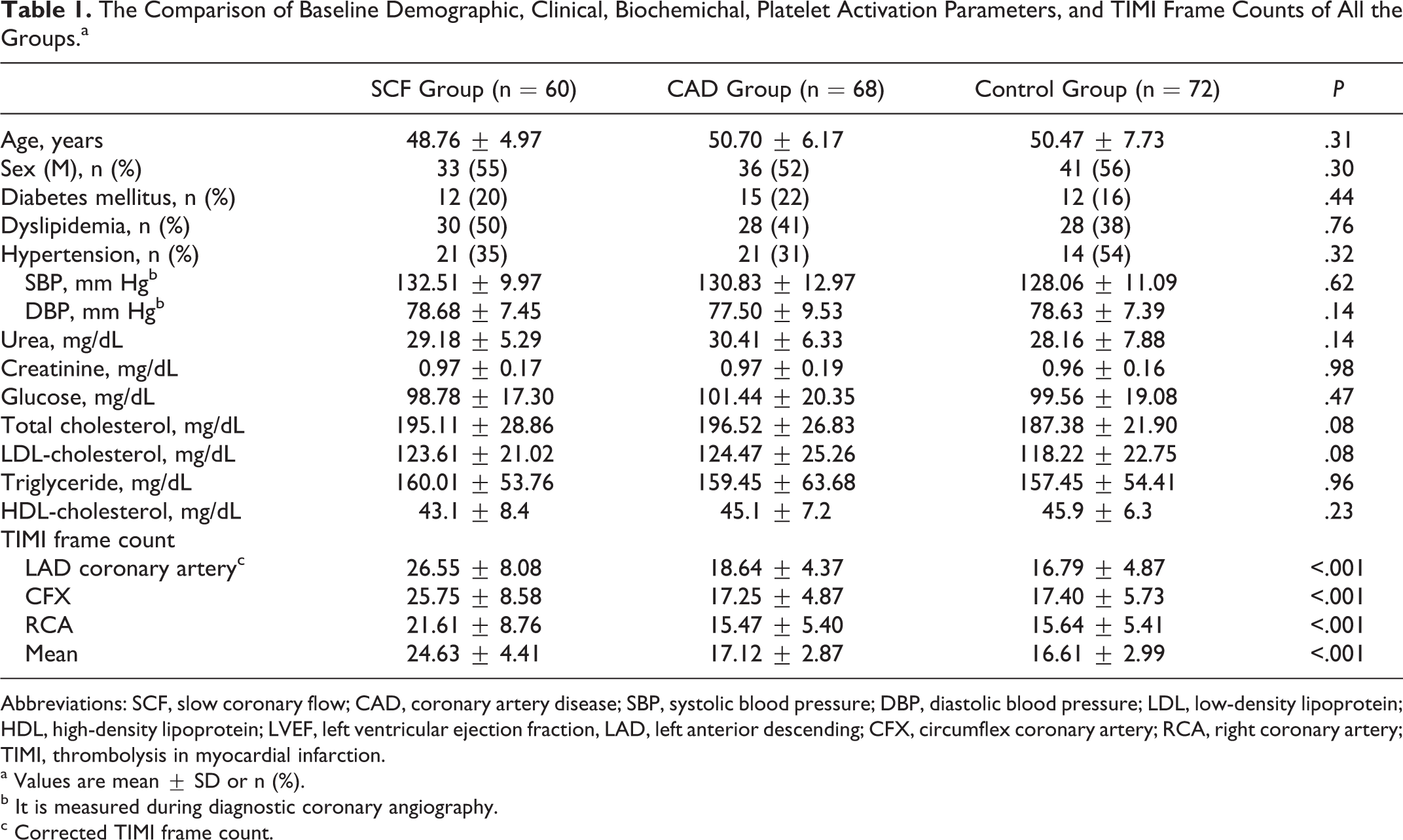
Abbreviations: SCF, slow coronary flow; CAD, coronary artery disease; SBP, systolic blood pressure; DBP, diastolic blood pressure; LDL, low-density lipoprotein; HDL, high-density lipoprotein; LVEF, left ventricular ejection fraction, LAD, left anterior descending; CFX, circumflex coronary artery; RCA, right coronary artery; TIMI, thrombolysis in myocardial infarction.
a Values are mean ± SD or n (%).
b It is measured during diagnostic coronary angiography.
c Corrected TIMI frame count.
Comparison of the Neutrophils/to Lymphocytes Ratio and Carotid Intima-Media Thickness Among the Study Groups.a
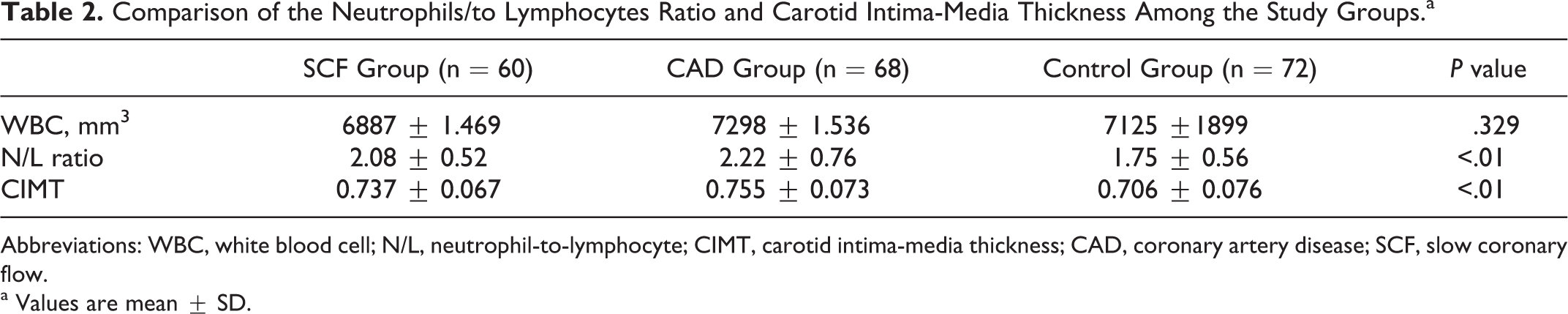
Abbreviations: WBC, white blood cell; N/L, neutrophil-to-lymphocyte; CIMT, carotid intima-media thickness; CAD, coronary artery disease; SCF, slow coronary flow.
a Values are mean ± SD.
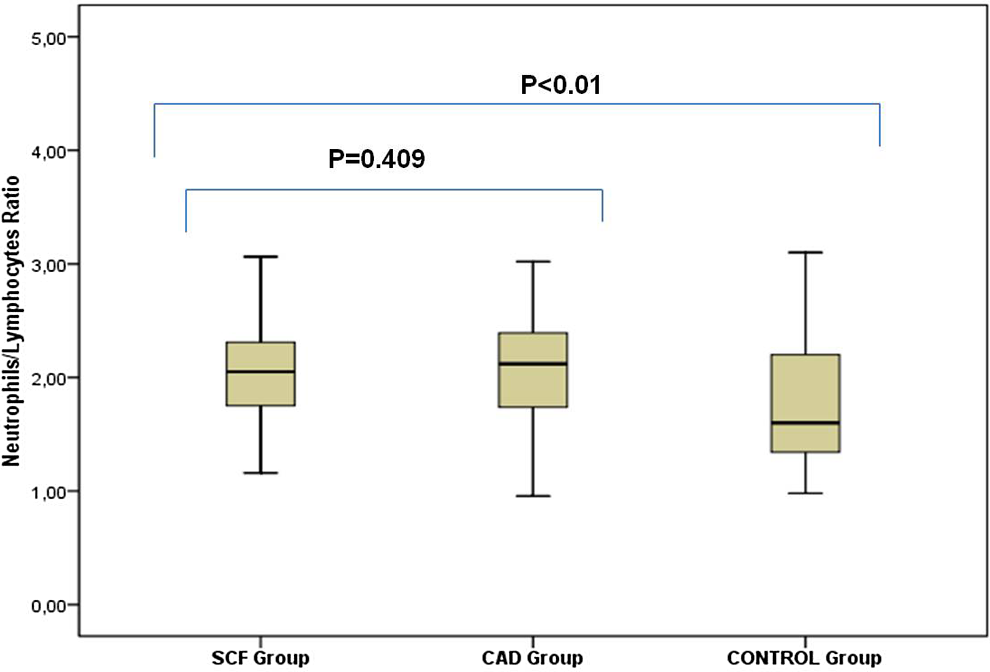
Neutrophil-to-lymphocyte (N/L) ratio was significantly higher in patients in both the SCF and the CAD groups, compared to the control group (P < .01). There was no significant difference in N/L ratios between SCF group and CAD group (P = .409). CAD indicates coronary artery disease; SCF, slow coronary flow.
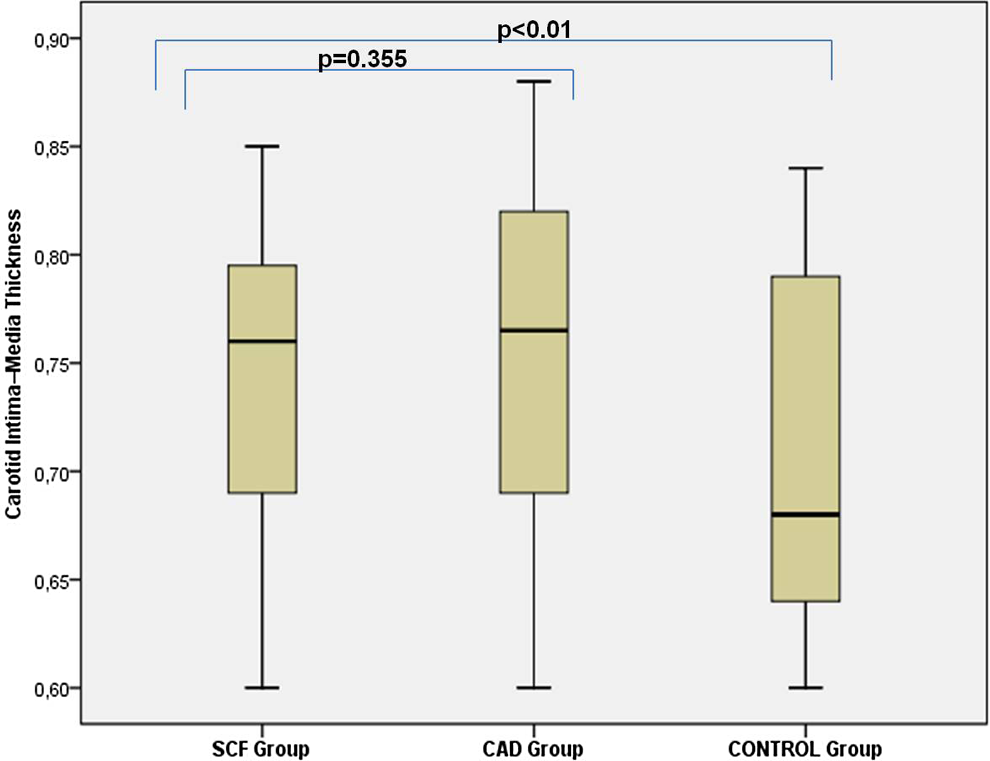
Carotid intima-media thickness (CIMT) levels were higher in patients in both the SCF and the CAD groups, compared to the control group (P < .01). There was no significant difference in CIMT levels between SCF group and CAD group (P = .355). CAD indicates coronary artery disease; SCF, slow coronary flow.
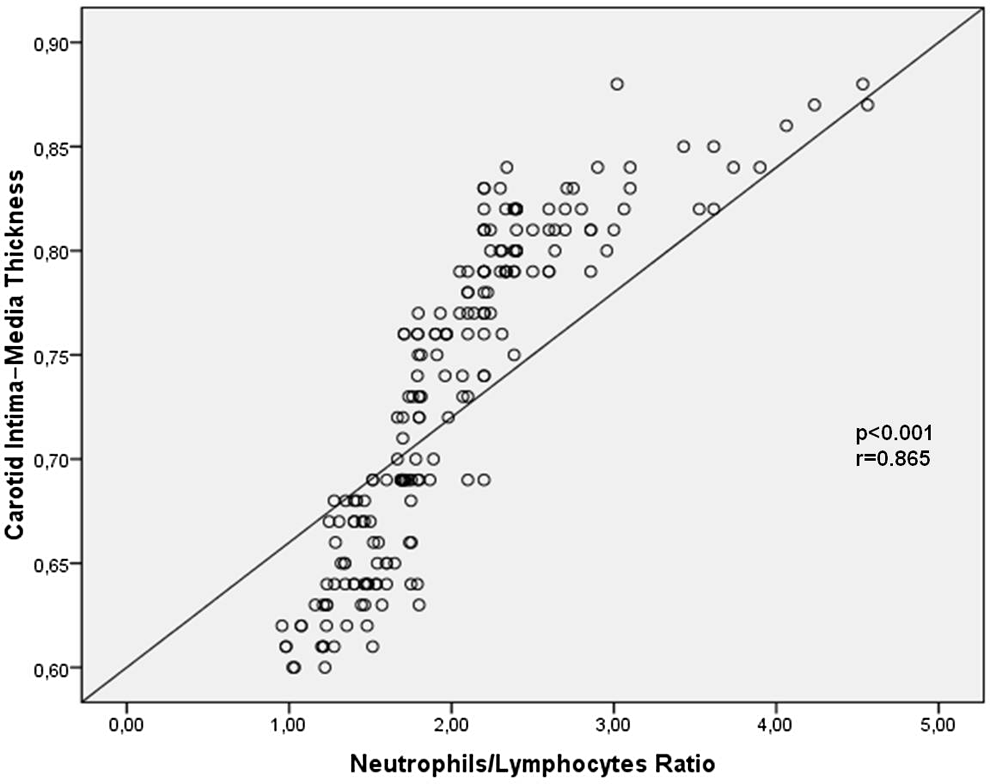
Significant positive correlations were detected between carotid intima-media thickness (CIMT) and neutrophil-to-lymphocyte (N/L) ratio (P < .01, r = .865).
Discussion
In the present study, we have found that N/L ratio levels were significantly increased not only in patients with SCF but also in patients with CAD compared to those in control patients. These results may indicate that elevated serum N/L ratio levels may be associated with the atherosclerotic process, inflammation, and endothelial dysfunction of SCF. The CIMT levels were significantly increased in patients with SCF compared to control group. There were also significantly positive correlations between CIMT and plasma level of N/L ratio in our study.
Although the etiologic mechanisms of SCF remain unknown, several hypotheses have been suggested as the pathophysiology of SCF, such as occlusive disease of small coronary arteries, 11 diffuse atherosclerosis, and endothelial dysfunction. 12 –14 Based on this hypothesis, SCF phenomenon may be a form of early phase of atherosclerosis in some patients. 14 Recent studies have displayed that elevated levels of inflammatory molecules are markers of atherosclerotic disease activity and also indicate an increased risk of the progression of atherosclerosis. 15 The pathogenesis of atherosclerosis is multifactorial; however, the effector roles of inflammatory cells for plaque formation are clear. 16 Endothelial dysfunction is the first stage in atherosclerosis. The regenerative capacity of endothelium provides protection against atherosclerosis. Failure of the endothelial repair initiates atherosclerotic inflammation and lesion formation, so-called plaque, especially in nonlaminar flow stress points in vascular bed. 17 From those, C-reactive protein (CRP) has been evaluated in many studies as an inflammatory marker and has been the most applicable one in clinical practice. 18 Increased CRP levels suggest that inflammation may be associated with pathogenesis of atherosclerosis or at least in part contributes to SCF pathogenesis. Increased high-sensitivity CRP (hs-CRP) level may also be an early marker of impaired coronary blood flow. The authors aimed to determine the role of inflammation in pathogenesis of SCF in a previous study. Serum hs-CRP concentration was significantly higher in SCF compared to the control patients in this study. Correlation analysis showed a positive correlation between hs-CRP level and TFC for each artery in patients with impaired coronary blood flow. 19 Moreover, the mechanism of the imbalance between vasoconstrictor and vasodilatory factors has also been proposed for SCF. Asymmetric dimethylarginine (ADMA), an endogenous inhibitor of nitric oxide synthesis, levels are associated with an increased risk of endothelial dysfunction and atherosclerosis. The ADMA levels may be increased by homocysteine. Plasma nitric oxide concentrations were significantly lower in the SCF group than in the control group. Plasma ADMA concentrations and plasma homocysteine concentrations were significantly higher in the SCF group than in the control group. These results suggest that the etiology of SCF may indicate impaired coronary blood flow as an endothelial injury. 9 Recently published studies have highlighted the imbalance between endothelin 1 and nitric oxide release in patients with SCF when compared to controls with normal coronary flow. 20,21 Measurements of CIMT using ultrasound assess the extent and the severity of systemic atherosclerosis. It has been shown that there is a direct relationship between CIMT and clinical cardiovascular disease. 22 A previous study showed that patients with SCF had a significantly increased CIMT compared to those with normal coronary flow. 23 Due to these data, CIMT assessment, which is a strong inflammatory marker, can be used to document regression or progression of atherosclerosis, and it can be used to correlate with the other newly inflammatory markers such as N/L ratio. 3 It still remains to be determined whether either microvascular or epicardial diffuse atherosclerotic disease is related to slow flow. The CIMT was significantly increased in patients with SCF than in controls. The SCF is the result of coronary atherosclerosis, which is the part of systemic involvement. 2 The CIMT values increased in patients with coronary slow flow in a previous study. These findings allow us to conclude that the CIMT values in patients with coronary slow flow may have a role in the etiopathogenesis of this phenomenon by causing generalized atherosclerosis. 23
Until now, the association between N/L ratio and atherosclerosis in the general population has been poorly understood. The relationship between N/L ratio and SCF is exactly unknown, and systemic factors such as inflammation and oxidative stress likely play a role. We considered that inflammation has been shown to be associated with endothelial dysfunction and silently atherosclerosis in patients with SCF. The WBC count is one of the useful inflammatory biomarkers in clinical practice. Leukocyte subtype and N/L ratio are also indicators of systemic inflammation. 6,7,24 These markers have prognostic importance in cardiovascular disease. The relation between atherosclerosis progression and leukocyte subtype was evaluated in a previous study. The progression rate was significantly high in patients with high N/L ratio, and it was a predictor for the progression of atherosclerosis. 25 More recently, N/L ratio has been proposed as a useful biomarker to predict cardiovascular risk. 26,27 Zazula et al investigated the relationship between the N/L ratio and the patient with suspicion of acute coronary syndrome. The N/L ratio was found to be significantly higher in patients with unstable angina, ST-segment elevation myocardial infarction (STEMI), and non-STEMI groups compared to the patients diagnosed with noncardiac chest pain. 28 On the other hand, N/L ratio has been associated with poor outcomes in patients who underwent coronary angiography. The maximum N/L ratio value may be a useful marker to predict the subsequent mortality in patients admitted for STEMI. 29 In a previous study, Arbel et al 30 evaluated whether N/L ratio adds additional information beyond that provided by conventional risk factors and biomarkers for CAD severity and adverse outcome, in a large cohort of consecutive patients referred for coronary angiography. The N/L ratio is independently associated with CAD severity and 3-year follow-up outcomes. The N/L ratio may appear additive to conventional risk factors and commonly used biomarkers. Inflammation plays a crucial role in the pathogenesis of in-stent restenosis. In a previous study, Turak et al 31 investigated the N/L ratio in patients undergoing coronary stent implantation. The authors found higher N/L ratio in patients with a high rate of stent restenosis compared to patients with a low rate of stent restenosis. Although WBCs are in normal range, subtypes of WBCs may predict cardiovascular mortality. The N/L ratio is also an inflammatory marker of major adverse cardiac events (MACEs) in both acute coronary syndromes and stable CAD. The lowest N/L ratio had fewer MACEs compared with the highest N/L ratio. 32 The N/L ratio was a strong independent predictor of long-term mortality after STEMI treated with very early revascularization. 33 In-hospital MACEs were significantly higher in patients with no reflow, and there was a significant and positive correlation between hs-CRP and N/L ratio. 34 Gibson at al investigated leukocyte subtypes such as the N/L ratio in patients undergoing CABG. An elevated N/L ratio is associated with a poor survival after CABG. 35 Hartaigh et al 36 investigated the relation between N/L ratio and cardiovascular mortality. The authors found a significant relationship between N/L ratio and cardiovascular deaths. It is therefore possible that specific subtypes such as the N/L ratio may contribute to the prediction of cardiovascular outcomes.
Because of all of these interactions, etiology of the relationship between N/L ratio and SCF may be the inflammation and silent atherosclerosis. Therefore, we aimed to investigate the N/L ratio in patients with SCF compared to patients with CAD and normal patients. In the present study, N/L ratio and CIMT were significantly increased in patients with SCF. There were significantly positive correlations between CIMT and plasma level of N/L ratio in our study. Hence, N/L ratio was used in routine clinical practice as an inflammatory marker. 37,38 It suggests that endothelial dysfunction may modulate the effect of SCF risk factors.
Study Limitations
The main limitation of our study was the relatively small sample size of the study population. Another limitation was the possibility of any underlying coronary artery spasm in patients with SCF, which was ruled out by a hyperventilation test despite the superiority of the ergonovine test. Finally, the intravascular ultrasound (IVUS) provides more precise values about the presence and distribution of atherosclerosis in vessel lumen and throughout the wall. We did not have the opportunity to perform IVUS in this study, despite IVUS being a more sensitive technique than coronary angiography for detecting coronary atherosclerosis.
Conclusion
Our findings show that patients with SCF have significantly increased N/L ratio levels. We have shown for the first time that patients with SCF and CAD have higher N/L ratio compared to the controls with normal coronary angiograms. These data suggest that N/L ratio is higher in patients with SCF and CAD compared to patients with otherwise normal coronary angiograms. The relation between cardiac syndrome X and higher N/L ratio level suggest that, besides endothelial dysfunction, presence of atherosclerosis may also contribute to the etiopathogenesis of the SCF phenomenon. We believe that further studies are needed to clarify the role of N/L ratio in SCF-complicated CAD, especially in relation to angiographic and clinical parameters. We conclude that N/L ratio may be used as a follow-up marker during the management of relevant patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.