
Abstract
Orosomucoid is an acute-phase serum protein that is upregulated in urine samples of patients with diabetic nephropathy. We assessed serum and urinary orosomucoid levels in children and adolescents with type 1 diabetes and their relation to microvascular complications and carotid intima–media thickness (CIMT). Sixty patients with type 1 diabetes were divided into 2 groups according to the presence of microvascular complications and compared with 60 healthy controls. High-sensitivity C-reactive protein (hs-CRP), hemoglobin A1c (HbA1c), urinary albumin–creatinine ratio (UACR), serum and urinary orosomucoid, and CIMT were assessed. Both serum and urinary orosomucoid levels were significantly increased in patients with and without microvascular complications compared with controls, and the highest levels were in patients with complications (P < .001). Serum and urinary orosomucoid were higher in patients with microalbuminuria than normoalbuminuric group (P < .001). The cutoff value of urinary orosomucoid at 2825 ng/mL could differentiate patients with and without microvascular complications. Serum and urinary orosomucoid were positively correlated. Multiple regression analysis showed that HbA1c, UACR, hs-CRP, and CIMT were independently related to orosomucoid. We suggest that orosomucoid is a significant independent factor for diabetic microvascular complications and can be considered as an early marker of renal injury. High orosomucoid levels in type 1 diabetes reflect endothelial dysfunction and subclinical atherosclerosis.
Introduction
Type 1 diabetes is the predominant form of diabetes during childhood and adolescence, accounting for about 90% of cases, although the growing epidemic of obesity has been associated with an increasing number of cases of childhood-onset type 2 diabetes. 1,2 Diabetes complications represent a huge burden for patients and health services. The fight against each single complication has led to significant improvements in diabetes care, especially for microvascular complications, yet macroangiopathy remains a major source of morbidity and mortality. A common approach for the prevention and treatment of diabetes complications relies on the understanding of their complex pathophysiology 3 and on the identification of disease markers.
Several inflammatory markers have been associated with the incidence of diabetes, including C-reactive protein (CRP), 4 sialic acid, white blood cells, 5 interleukin (IL) 6, 6 and orosomucoid. 5 As inflammation proceeds, the risk for vascular complications increases. 7
Diabetic nephropathy (DN) remains the most common cause of chronic kidney disease worldwide. Diabetic nephropathy is characterized by a long clinically silent period without signs or symptoms of disease. There is an urgent need for improved methods of detecting early mediators of renal injury to ultimately prevent the initiation and progression of DN. 8
The development of methods for comparing urinary proteomes has been demonstrated to identify proteins or protein patterns that may serve as biomarkers or identify new pathogenesis for DN and other renal diseases. 9 –11 One of these proteins is orosomucoid, also known as α1-acid glycoprotein (AGP). Orosomucoid is an acute-phase serum protein produced by the liver in response to inflammation and infection. 12 Orosomucoid plays an important role as an anti-inflammatory and immunomodulatory agent. 13,14 Furthermore, orosomucoid has shown promise as a therapeutic agent. 15 Orosomucoid has been found to be highly upregulated in urine samples of patients with DN. 11,16 Increased urinary orosomucoid excretion rate (UOER) was an independent, powerful predictor of cardiovascular mortality in normoalbuminuric patients with type 2 diabetes. 17,18
Carotid intima–media thickness (CIMT) testing is recognized as a valid method for the noninvasive assessment of atherosclerosis. In addition to its association with known cardiovascular risk factors and both prevalent and incident coronary heart disease, the rate of CIMT progression is directly related to the risk for future cardiovascular events. 19 Therefore, this study aimed to measure serum and urinary orosomucoid levels in young patients with type 1 diabetes and assessed their relation to inflammation, glycemic control, and microvascular complications as well as CIMT.
Materials and Methods
This cross-sectional study included 60 children and adolescents with type 1 diabetes attending the Pediatric Diabetes Clinic, Pediatric Hospital, Ain Shams University. Patients were defined according to the criteria of American Diabetes Association. 20 They included 28 males and 32 females with a male-to-female ratio of 1:1.1, and their ages ranged from 8 to 17 years with a mean of 12.8 ± 3.9 years. Another group of 60 age- and sex-matched healthy volunteers were enrolled as controls. An informed consent was obtained from each patient or control participant or their legal guardians before enrollment into the study. The study was approved by the local ethical committee of Ain Shams University.
Inclusion criteria were children and adolescents with type 1 diabetes ≤18 years with at least 5 years disease duration and on regular clinic visits and regular insulin therapy. Exclusion criteria were the presence of any clinical evidence of infection, history of allergies, rheumatoid arthritis, recent trauma, surgery, liver dysfunction, connective tissue disease, or other autoimmune disorders and any other conditions that could influence high-sensitivity C-reactive protein (hs-CRP). Patients with hs-CRP >10 mg/L were excluded.
Patients were divided into 2 groups according to the presence of microvascular complications: Group 1 (patients with complications) included 30 patients with type 1 diabetic microvascular complications. Patients included in this group had either one or more of these inclusion criteria: DN, retinopathy, or peripheral neuropathy. The presence of microvascular complications was investigated starting from the diagnosis of diabetes and further verified at the time of the study by clinical examination and investigations. Group 2 (patients without complications) included 30 children with type 1 diabetes who lacked the previously mentioned microvascular complications both at the study time and in their previous records.
The studied patients were subjected to detailed medical history and thorough clinical examination, with special emphasis on age of onset of diabetes, disease duration, insulin therapy, and chronic diabetic complications (nephropathy, peripheral neuropathy, retinopathy, or cardiovascular ischemic events). All patients were on insulin therapy using human insulin with a mean dose of 1.8 ± 0.38 IU/kg/d.
Anthropometric measurements were recorded, and body mass index (BMI) was calculated. Blood pressure was measured after a 5-minute rest in the seated position using mercury sphygmomanometer. If it was greater than 90th percentile for age and sex, the blood pressure was repeated twice for the validity of the reading.
Diabetic retinopathy was diagnosed by doing complete ocular examination including visual field testing, slit-lamp biomicroscopy, Volk lens, and indirect ophthalmoscopy. Fundus examination was performed through dilated pupils using 90-diopter Volk lens and biomicroscope. The presence and grading of diabetic retinopathy were based on the International Clinical Diabetic Retinopathy and Macular Edema Disease Severity Scale. 21 The simple rapid bedside neuropathy disability score (NDS) was adopted as a screening tool for diabetic peripheral neuropathy. The NDS was derived from examination of vibration perception (by means of a 128-Hz tuning fork), pinprick, temperature perceptions in the great toe, and the presence or absence of ankle reflexes. The sensory modalities were scored, and a score above 2 was defined as clinical diabetic peripheral neuropathy. 22 Results were confirmed by nerve conduction velocity to provide accurate diagnosis. 23
Laboratory Investigations
Liver and kidney function tests, fasting lipid profile, hs-CRP, and fasting blood glucose (FBG) levels were measured using Cobas Integra 800 (Roche Diagnostics, Mannheim, Germany). The FBG was assessed during regular clinic visits with calculations of the mean values during the last 6 months prior to the study including the level of a blood sample at the start of the study. Dyslipidemia was defined if at least one of the following was present: serum total cholesterol ≥200 mg/dL, low-density lipoprotein cholesterol ≥100 mg/dL, high-density lipoprotein cholesterol <40 mg/dL, or serum triglyceride ≥150 mg/dL. 24 Further analysis was done after controlling for age and pubertal stage to avoid differences in lipid values. 25 Assessment of the mean percentage hemoglobin A1c (HbA1c%) in the year preceding the study was performed using D-10 (BioRad, France). Urinary albumin excretion (as an indicator of nephropathy) was measured in an early morning urine sample as albumin-to-creatinine ratio by an immunonephelometric method. Microalbuminuria and macroalbuminuria were present if urinary albumin excretion in at least 2 out of 3 consecutive urine samples, 2 months apart was 30 to 299 mg/g creatinine and ≥300 mg/g creatinine, respectively. 26,27 Potential factors affecting urinary albumin excretion were excluded. 28 Determination of serum and urinary levels of orosomucoid was done by enzyme-linked immunosorbent assay (ELISA) using Quantikine human orosomucoid (AGP) immunoassay (R&D systems, Minneapolis, Minnesota) according to the manufacturer’s instructions.
Sampling
Peripheral blood samples were collected on ethylene diamine tetraacetic acid (1.2 mg/mL) for analysis of HbA1c. Serum obtained from clotted samples by centrifugation for 15 minutes at 1000g was used for chemical analysis and stored at −20°C till subsequent use in ELISA.
Measurement of CIMT
All of the carotid scans were done using carotid Doppler ultrasound scanner (Xario, Toshiba Ultrasonography machine, Tokyo, Japan) with a 10.0-MHz linear array transducer following a predetermined standardized scanning protocol. 29 The Doppler ultrasound studies were performed after an overnight fast and before the administration of morning insulin dose. Patients were placed in supine position having the neck in hyperextension. The left and right common carotid arteries were imaged in a standardized magnification (2 × 2 cm), with images of the posterior wall of the distal 10 mm of the common carotid artery just proximal to the carotid bulb. Images were captured when both the anterior and posterior wall margins were clearly seen to ensure the images were taken perpendicular to the vessel. A minimum of 4 images of each of the common carotid arteries were taken. All images were taken at end diastole, incident with the R-wave on a continuously recorded electrocardiogram and then digitally stored for later analysis. The 3 best quality images for each of the carotid arteries were selected and analyzed. Best quality was defined with those images that produced the most number of points for analysis. For each image, the greatest distance between the lumen–intima interface and media–adventitia interface (intima–media thickness [IMT]) was measured at a minimum of 100 points. The mean and maximum IMT of each image were then averaged to give the final result for each patient. All the ultrasonographic examinations were analyzed by a single experienced radiologist blinded to the group to which the patients belonged.
Statistical Analysis
Analysis of data was done using Statistical Program for Social Science version 15 (SPSS Inc, Chicago, Illinois). Quantitative variables were described in the form of mean, standard deviation, median, and interquartile range, and qualitative variables were described as number and percentage. In order to compare quantitative parametric variables between the 3 studied groups, analysis of variance test with post hoc test was used. Comparison of nonparametric variables was carried out using Kruskal-Wallis and Mann-Whitney U tests. Categorical variables were compared using χ2 test. Spearman rank correlation coefficient and stepwise multiple linear regression analysis were used to assess the relation between the studied markers and the clinical as well as laboratory variables. Logistic regression was used to examine the relation between orosomucoid and microvascular complications after adjustment of other variables: age, gender, and BMI. Receiver operating characteristic (ROC) curve was used to determine the best cutoff value of urinary and serum orosomucoid to detect microvascular complications. The area under the curve (AUC) was calculated for each plot. A P value < .05 was considered significant in all analyses.
Results
The clinical and laboratory data of patients are listed in Table 1. Age, sex, and BMI were consistent among all patients compared with controls and in each subgroup of patients when compared separately with the control group (P > .05). Serum creatinine was within the normal range. Urinary albumin–creatinine ratio (UACR) was assessed as an early predictor of nephropathy, and the most common microvascular complication encountered in the studied diabetic patients was microalbuminuria being in 20 (33.3%) patients followed by peripheral neuropathy (18.3%) and retinopathy (10%). Seven patients had more than 1 complication; 4 of them were within the microalbuminuric group (3 patients had peripheral neuropathy and 1 patient had retinopathy). None of the studied patients had macroalbuminuria or macrovascular complications.
Clinical and Laboratory Variables of Patients With Type 1 Diabetes and Healthy Controls.a
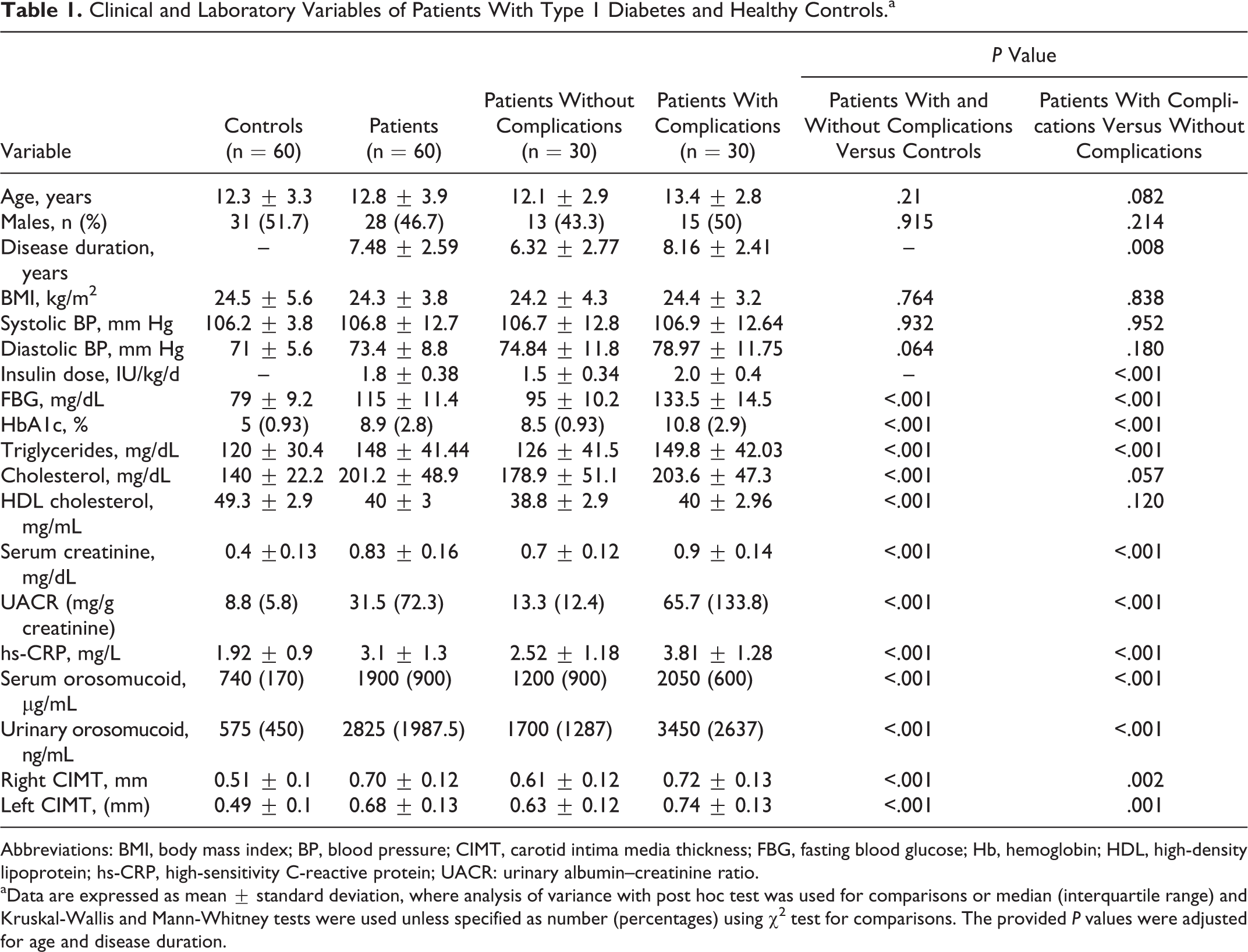
Abbreviations: BMI, body mass index; BP, blood pressure; CIMT, carotid intima media thickness; FBG, fasting blood glucose; Hb, hemoglobin; HDL, high-density lipoprotein; hs-CRP, high-sensitivity C-reactive protein; UACR: urinary albumin–creatinine ratio.
aData are expressed as mean ± standard deviation, where analysis of variance with post hoc test was used for comparisons or median (interquartile range) and Kruskal-Wallis and Mann-Whitney tests were used unless specified as number (percentages) using χ2 test for comparisons. The provided P values were adjusted for age and disease duration.
As shown in Table 1, patients with microvascular complications had longer disease duration and higher FBG, HbA1c, triglycerides, UACR, hs-CRP, and CIMT compared with patients without complications and healthy controls (P < .05). Moreover, FBG, HbA1c, triglycerides, total cholesterol, serum creatinine, UACR, hs-CRP, and orosomucoid levels in serum or urine as well as CIMT were significantly higher in patients without complications compared with controls (P < .001).
Both serum and urinary orosomucoid were elevated in all diabetic patients and in both groups with or without microvascular complications compared with healthy controls. The highest levels were observed among patients with microvascular complications (P < .001; Table 1). Analysis of serum and urinary orosomucoid in relation to each microvascular complication revealed a significant elevation in diabetic patients with microalbuminuria compared with normoalbuminuric group (2000 [800] ng/mL vs 1200 [900] ng/mL and 3250 [775] ng/mL vs 1675 [1175] ng/mL, respectively; P < .001; Figure 1).
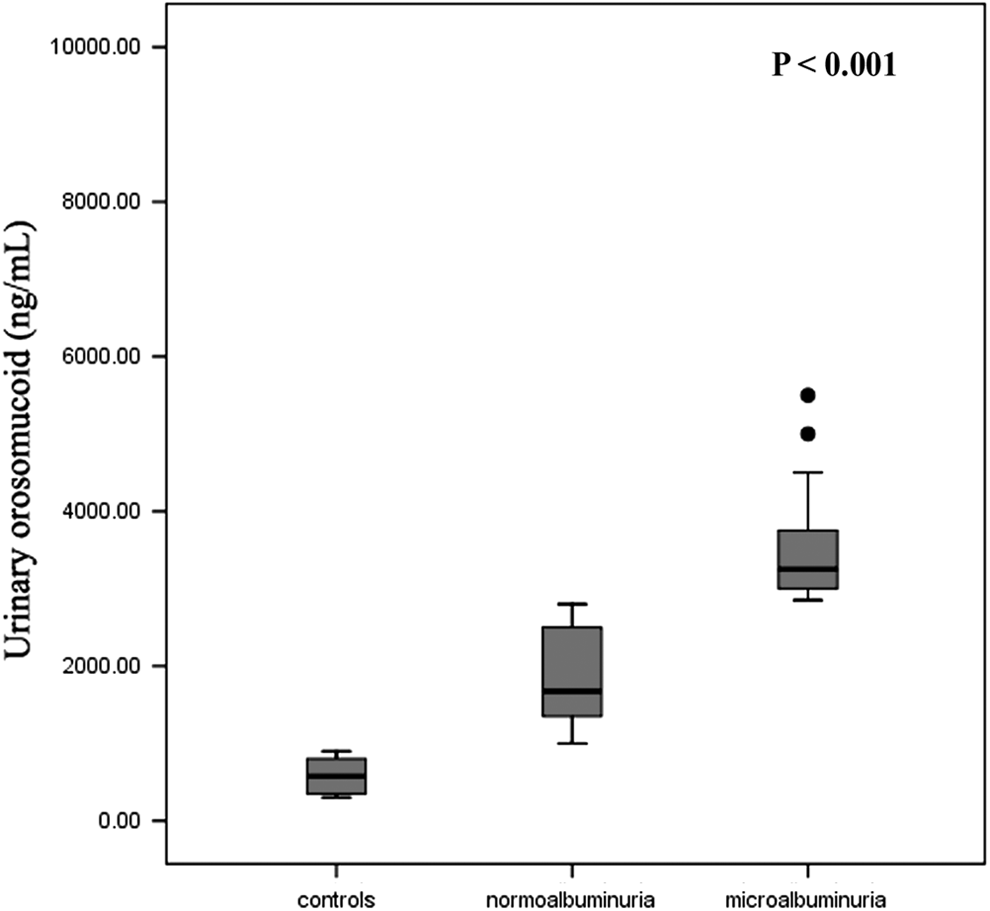
Urinary orosomucoid levels among diabetic patients in different albuminuric stages and controls.
The ROC curve analysis revealed that the cutoff value of urinary orosomucoid at 2825 ng/mL could differentiate diabetic patients with and without microvascular complications with a sensitivity and specificity of 90% (AUC: 0.899; 95% confidence interval [CI]: 0.811-0.988; P < .001). In addition, the cutoff value of serum orosomucoid at 1700 μg/mL could detect microvascular complications with a sensitivity of 76.5% and specificity of 76.9% (AUC: 0.792; 95% CI: 0.668-0.886; P < .001).
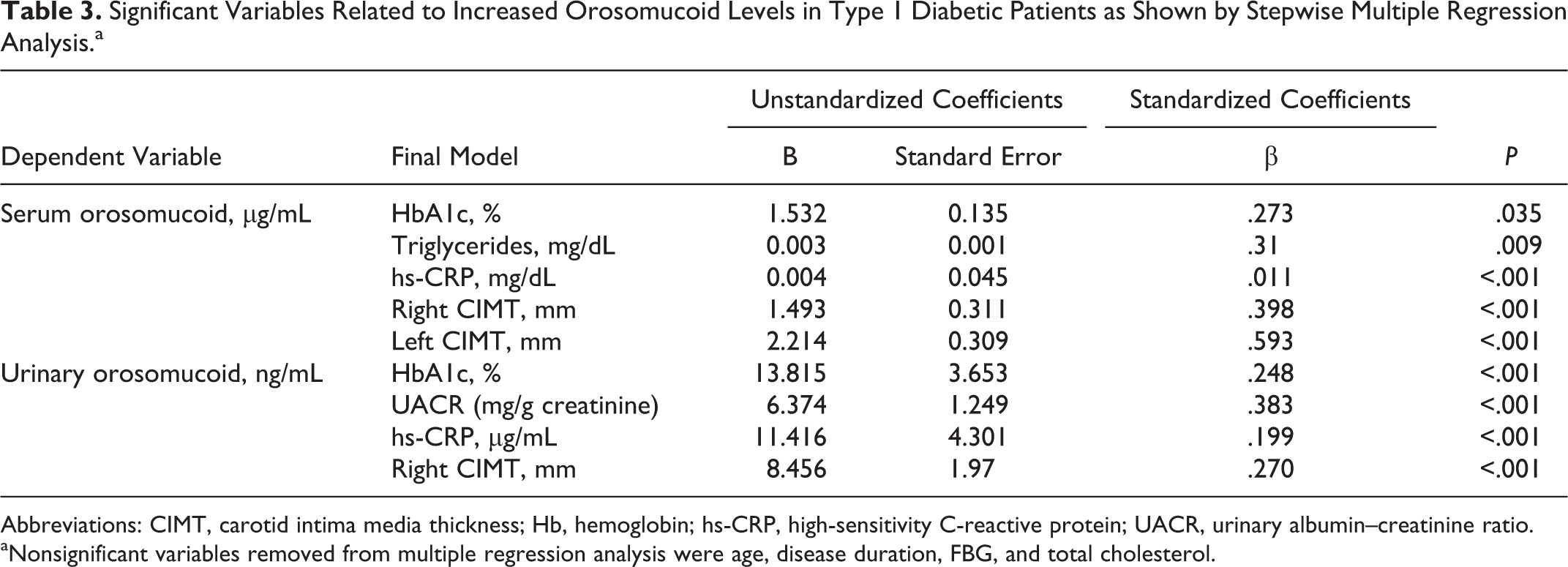
Both serum and urinary orosomucoid levels were positively correlated (r = .617, P < .001). Significant positive correlations were also observed between both markers and each of age, disease duration, FBG, HbA1c, triglycerides, total cholesterol, UACR, hs-CRP, and CIMT (P < 0.05; Table 2 and Figure 2). Stepwise multiple regression analysis included all the above correlated variables and showed that HbA1c, triglycerides, UACR, hs-CRP, and CIMT were independently related to serum and urinary orosomucoid (P < .001; Table 3). Logistic regression showed that orosomucoid was a significant independent factor for microvascular complications (odds ratio: 2.1, 95% CI: 1.72-2.81; P < .001).
Correlations Between Orosomucoid Levels in Serum or Urine and the Studied Clinical and Laboratory Parameters Among Patients With Type 1 Diabetes.
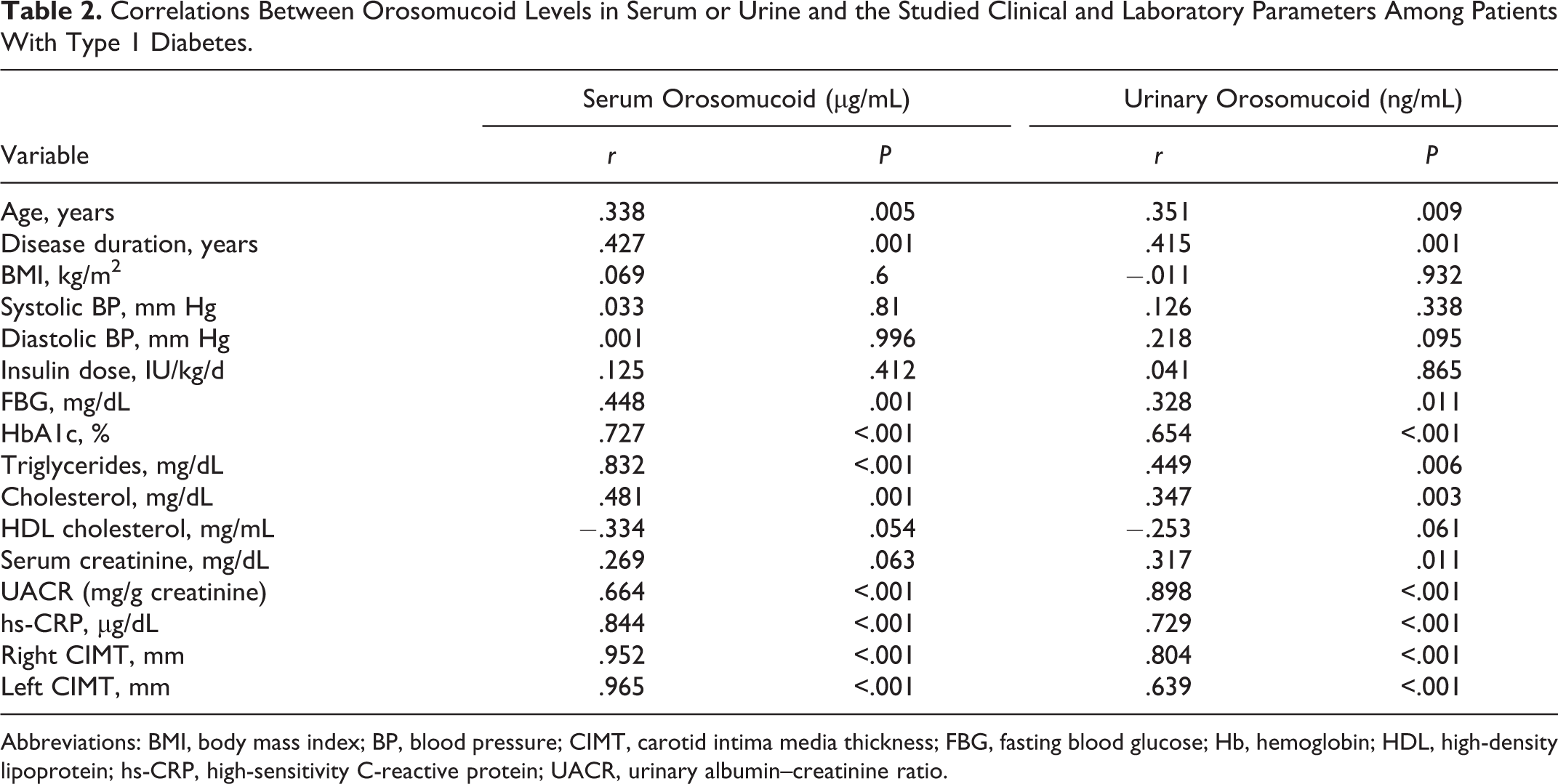
Abbreviations: BMI, body mass index; BP, blood pressure; CIMT, carotid intima media thickness; FBG, fasting blood glucose; Hb, hemoglobin; HDL, high-density lipoprotein; hs-CRP, high-sensitivity C-reactive protein; UACR, urinary albumin–creatinine ratio.
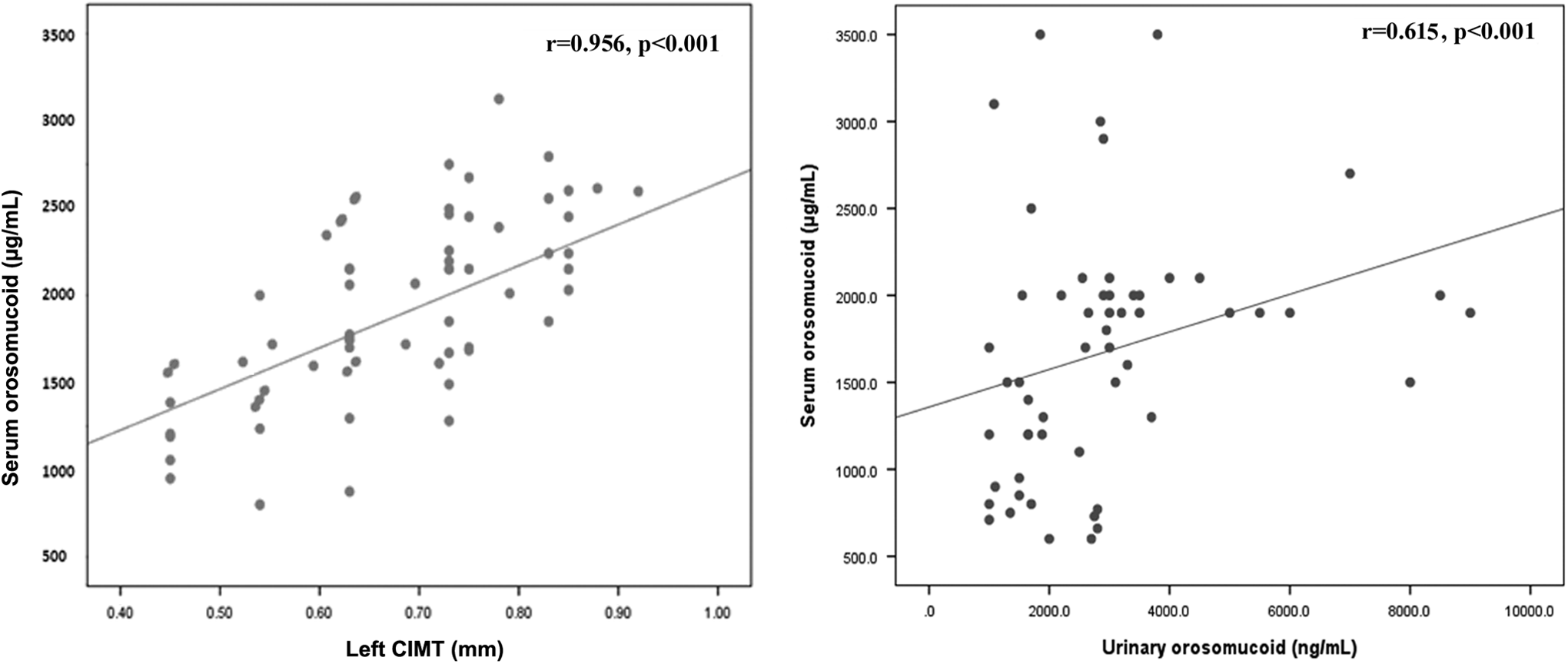
Positive correlations between serum orosomucoid and each of left carotid intima–media thickness (CIMT; A) and urinary orosomucoid (B) among patients with type 1 diabetes.
Significant Variables Related to Increased Orosomucoid Levels in Type 1 Diabetic Patients as Shown by Stepwise Multiple Regression Analysis.a
Abbreviations: CIMT, carotid intima media thickness; Hb, hemoglobin; hs-CRP, high-sensitivity C-reactive protein; UACR, urinary albumin–creatinine ratio.
aNonsignificant variables removed from multiple regression analysis were age, disease duration, FBG, and total cholesterol.
Discussion
Diabetes is associated with both microvascular and macrovascular diseases affecting several organs, including muscle, skin, heart, brain, and kidneys. A common etiology links the different types of diabetes-associated vascular disease. Mechanisms for vascular disease in diabetes include the pathologic effects of advanced glycation end-product accumulation, impaired vasodilatory response attributable to nitric oxide inhibition, smooth muscle cell dysfunction, overproduction of endothelial growth factors, chronic inflammation, hemodynamic dysregulation, impaired fibrinolytic ability, and enhanced platelet aggregation. 30
However, several studies have reported a nonsignificant relation between inflammation and incidence of diabetes. Negative or inconclusive results have been reported for CRP, haptoglobin, fibrinogen, white blood cells, and α1-antitrypsin. It is unclear whether the discrepancies among studies are related to differences with respect to inflammatory markers, study populations, or other factors. 31 Monitoring the urinary excretion of specific proteins in acute disease may provide information of clinical relevance, given future sufficient pathophysiologic insight and availability of appropriate technology. 32
In this study, patients with microvascular complications had longer disease duration than those without complications. Disease duration is an established risk factor affecting the frequency of complications where the risk of occurrence of complications is increased with the progression of disease duration. 33 In a series of 292 patients with type 1 diabetes who were followed for 20 to 40 years, the rate of development of macroalbuminuria peaked at about 2.5% per year at disease duration of 10 to 14 years and then gradually declined to 1% or less per year after 20 years. 34
The significantly higher FBG, HbA1c, UACR, and triglycerides observed in our patients with microvascular complications support previous reports with a significant association between diabetic complications, poor glycemic control, and dyslipidemia. 35 –37 Rossing et al 38 reported that the risk factors for progression of microalbuminuria to overt nephropathy in type 1 diabetic patients are duration of diabetes, urinary albumin excretion rate, and poor metabolic control. The increase in hs-CRP encountered in type 1 diabetic patients in this study, particularly those with microvascular complications, is similar to that reported by Coulon et al 39 who found that the levels of CRP were 3-fold greater in diabetic patients without complications compared to controls and 5-fold greater in diabetic patients with subclinical complications.
In the present study, serum and urinary orosomucoid levels were significantly elevated in all diabetic patients, particularly in those with microvascular complications compared with controls. Orosomucoid was also significantly increased in patients with nephropathy. The increase in inflammatory markers may have major implications on our understanding of the role of inflammation in vasculopathies related to diabetes. 40 It has been reported that orosomucoid is increased in urine to concentrations equal to or higher than albumin in proteinuria associated with acute inflammation. Monitoring of urinary excretion of orosomucoid and other specific proteins, expressed as protein–creatinine ratios, may provide a window for clinically relevant real-time observation of changes in acute inflammatory processes. Orosomucoid in urine may be a more informative marker than albumin for inflammation. 41
In agreement with our results, Jiang et al 11 identified orosomucoid by proteomic method in a Chinese Han population, 12 patients with DN (6 type 1 and 6 type 2 diabetic patients), and found that it was highly upregulated (>8-fold) in those patients. The data of immunoturbidimetric assay showed UOER was gradually increased in normoalbuminuria, microalbuminuria, and macroalbuminuria group versus controls. Meanwhile, their data indicated that there was no statistical difference in urinary orosomucoid between type 1 and type 2 diabetic patients. This indicated that UOER increased in early stage of DN and gradually increased with the development of DN, so increased UOER could have a predictive value for the risk of renal damage in type 1 and type 2 diabetic patients.
Our findings suggest that orosomucoid in serum or urine could serve as a biomarker for all microvascular complications in type 1 diabetes including DN. As microalbuminuria occurs relatively late in the disease process, evaluation of orosomucoid might become a useful test in the early stages of diabetes to identify normotensive and normoalbuminuric children and adolescents with type 1 diabetes at increased risk of developing diabetic kidney disease later in life, who might benefit from a timely and appropriate intervention. Interestingly, Narita et al 42 found that increased urinary excretions of several plasma proteins including orosomucoid precede the development of microalbuminuria in diabetic patients and increased in parallel with enhanced glomerular filtration rate after acute protein loading. Thus, albumin excretion rate may be a less sensitive marker to reflect changes in renal hemodynamics than excretion rates of orosomucoid.
To the best of our knowledge, this is the first study to provide a cutoff for orosomucoid levels in serum and urine as a marker for microvascular complications. Therefore, further prospective studies are needed to validate these thresholds before implementation in the therapeutic regimen.
In this study, multiple regression linear analysis showed that HbA1c, UACR, and hs-CRP were independently related to orosomucoid levels in type 1 diabetic patients. This suggests a link between poor metabolic control, low-grade inflammation, albuminuria level, and elevated orosomucoid. Although orosomucoid levels were positively correlated with disease duration, this variable was not a strong contributor to elevated orosomucoid levels in regression analysis. In line with these results, Jiang et al 11 found significant correlations between UOER and urinary albumin excretion rate, serum creatinine, and CRP in patients with DN.
The presence of positive correlation between both serum and urinary orosomucoid and hs-CRP in our work supports the role of orosomucoid in inflammation and vascular complications in type 1 diabetes. The relation between orosomucoid and CRP has been examined by Magid et al 41 who found that urinary excretion of orosomucoid increases and decreases in a temporal relationship to CRP. They did not perform simultaneous sampling of serum and urine and therefore were unable to determine whether increases in CRP and urinary orosomucoid coincide or whether one of these components precedes the other in time. Their observations suggest that monitoring of urinary excretion of orosomucoid, and possibly other specific proteins, may be as informative as CRP with regard to the assessment of acute inflammatory activity.
Cardiovascular screening should be offered to type 1 diabetic adolescents early in the disease, irrespective of the metabolic parameters. It has been suggested that inflammation contributes to the increased incidence of cardiovascular diseases among diabetic patients. 6 Therefore, we sought to examine the link between orosomucoid levels and CIMT as a simple noninvasive screening test for the assessment of atherosclerosis risk/prognosis. 43 There are limited studies evaluating the role of CIMT in type 1 diabetes mellitus in developing countries. 44 –46
Christiansen et al 17 investigated whether increased UOER was associated with cardiovascular risk factors such as inflammation, impaired left ventricular function, and endothelial dysfunction in patients with type 2 diabetes. They found that patients with diabetes and increased UOER had subclinically increased serum orosomucoid, CRP, IL-6, and other inflammatory markers compared with healthy controls and concluded that asymptomatic patients with type 2 diabetes and increased UOER displayed signs of chronic low-grade inflammation and endothelial dysfunction. Therefore, increased CIMT among our studied patients with and without microvascular complications than controls and its positive correlation with orosomucoid levels reflect the presence of subclinical atherosclerosis in those patients.
The occurrence and mechanisms of increased orosomucoid in patients with vascular complications still need to be explored. Pedersen and Sorenson 47 found a direct correlation between microalbuminuria and proinflammatory cytokines in malignancies, indicating a pathogenic relationship between inflammation and glomerular leakage of albumin. The glomerular membrane and the proximal tubuli both appear to be involved. Protein transport at these sites is incompletely understood and much debated, 48 and further research is needed to identify the causative factors of proteinuria associated with inflammation. 41
Jiang et al 11 assumed that the possible mechanisms of increased urinary orosomucoid in diabetic patients with DN may be as follows. First, enhanced glomerular filtration rate because of the elevation in urinary orosomucoid was closely associated with the increase in glomerular permeability. Second, as a marker of low-grade inflammation in patients with diabetes, 17 increased urinary orosomucoid may correlate with the inflammatory activation in patients with DN. Third, renal secretion of orosomucoid may cause the increased urinary levels. It has been shown that orosomucoid can be produced by glomerular endothelial cells. 11
Limitations of our study include the presence of a relatively small number of patients, particularly in the subgroups with a single complication. Further longitudinal prospective analysis including larger number of patients for each complication is needed.
In conclusion, the significant elevation in serum and urinary orosomucoid in children and adolescents with type 1 diabetes, particularly those with microvascular complication, and their correlation with CIMT may reflect low-grade inflammation, endothelial dysfunction, and the presence of subclinical atherosclerosis and represent a link between diabetic microangiopathy and macroangiopathy in juvenile-onset type 1 diabetes. Orosomucoid could be considered as an early marker of renal injury in type 1 diabetes. Assessment of CIMT and regular measurement of orosomucoid in serum or urine of young patients with type 1 diabetes, even in the absence of vascular complications or signs of subclinical atherosclerosis, would identify those at high risk of developing renal and cardiovascular disease later in life; however, this should be confirmed in larger longitudinal studies. As high orosomucoid levels were associated with increased lipids, poor glycemic control, vascular dysfunction, and renal injury, studies preintervention and postintervention targeting these factors are merited.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.