
Abstract
The activity of the enzyme methylenetetrahydrofolate reductase (MTHFR) determines homocysteine (Hcy) levels, and polymorphisms in its gene affect the activity of the enzyme. Changes in the enzyme’s activity may lead to a higher susceptibility to develop arterial and venous thromboembolic disease. The aim was to analyze the relationship between the C677T and A1298C polymorphisms of MTHFR, Hcy levels, and prothrombotic biomarkers in pulmonary embolism (PE) and acute myocardial ischemia (AMI). Clinical files of patients with thromboembolic diseases having complete data and whose doctor had requested an assay to determine the polymorphisms of the MTHFR gene, Hcy levels, and prothrombotic biomarkers were studied to search for the correlation between mutations of the MTHFR gene and Hcy levels in the different diseases. We included 334 files: 158 were from women and 176 from men (51 [19 SD] years). Sixty-three percent have had thrombosis, 8% AMI, and 31% PE. Patients with thrombosis had elevated frequency of the C677T polymorphism. The CC genotype was higher than the TT genotype (P = .003) and CT versus the TT (P = .009). In patients with PE, the CC genotype was higher than the TT genotype (P = .038). Pulmonary embolism with massive and submassive events had predominant genotypes 677 TT (P = .003) and the AA 1298 (P = .017). Elevated Hcy levels in the presence of the T allele in the C677T gene and of the A allele in the A1298C gene are associated with AMI and massive and submassive PE.
Introduction
Venous thromboembolic disease (VTD) includes deep vein thrombosis (DVT) and pulmonary embolism (PE). It is the third most common cause of cardiovascular disease having an incidence of 100 to 200 per 100 000 inhabitants. Although VTD and PE may be fatal in their acute or chronic phases, they can be prevented. 1 Smoking 2 and other endovascular and coagulation risk factors are associated with these diseases. 3 Polymorphisms of the gene encoding for the methylenetetrahydrofolate reductase (MTHFR) have also been related to an increased susceptibility to develop VTD.
Methylenetetrahydrofolate reductase regulates homocysteine (Hcy) levels. 4 Homocysteine is an intermediate amino acid containing a sulfhydryl group that comes from methionine methylation. 5 A transference of a methyl group of the 5-methyltetrahydrofolate to Hcy by MTHFR is required during Hcy metabolism. 6 For this reason, it has been proposed that metabolic alterations in the enzyme’s activity could lead to total homocysteine (tHcy) accumulation and lead to the appearance of some pathologies such as rheumatoid arthritis, cancer, 7,8 or vascular occlusive diseases. 9,10
Polymorphisms of the MTHFR gene could affect the enzyme’s activity. The C677T polymorphism has been associated with an increase in Hcy. 11 Homozygote individuals with the C677T polymorphism have increased plasma tHcy concentrations and this mutation is prevalent in coronary artery disease. 11 –18 A meta-analysis in an English population concluded that C677T and A1298C polymorphisms were associated with elevated plasma Hcy in acute myocardial ischemia (AMI), cerebral vascular events, DVT, and PE. 19 Other studies showed that homozygous 677TT patients have a higher risk of heart disease than homozygous 677CC individuals. 20 There are few studies analyzing the frequency of C677T and/or A1298C polymorphisms in coronary disease, PE, and their association with DVT.
The analysis of the risk factors associated with these polymorphisms through retrospective studies could lead to a better knowledge of factors prevalent in affected patients. Based on this fact, the aim of the present study was to evaluate the relationship between the C677T and A1298C polymorphisms of MTHFR enzyme, different prothrombotic biomarkers, and Hcy levels in patients who have had PE and AMI.
Patients and Material and Methods
This was a retrospective study done between March 2011 and December 2016. Six hundred fifty-five studies of the C677T and A1298C gene polymorphisms of the MTHFR gene on patients having had coronary, pulmonary, or other location arterial thrombosis and on whom Hcy, anti-B2 glycoprotein 1, anticardiolipin, and C and S protein had been measured were analyzed. Only 334 files from patients having complete data were included. Patients with missing data were excluded. The determinations of the C677T and A1298C gene polymorphisms of MTHFR were done by PCR with analysis of melting–fusion curves. For the determination of the C677T and A1298C polymorphism, the “LightMix Kit MTHFR” from Roche (Barcelona, Spain) was employed. The antithrombin activity was determined using the Berichrom kit that determines its plasmatic activity through automatic analyzers. The in vitro coagulometric Siemens kit (España) was used to determine factors II and VIII. FVIII antigen levels were measured at screening by enzyme immunoassay using the Asserachrom VIII:Ag kit (Stago, Asnières sur Seine, France) in all analyzed patients. Factor V: The activity of FV was determined to each of the samples.The assay was processed by coagulometric method in an STArt semiautomatic coagulometer (Diagnostica Stago SAS, Asnières sur Seine, France), which was used for the mechanical method detection. The reagents used for the measurement of FV were STA-Unicalibrator, Owren buffer pH 7.35, STA-Preciclot Plus I, STA-Factor V, and STA-Neoplastin (Diagnostica Stago SAS).
Plasma D-dimer levels were evaluated using an automated latex-enhanced quantitative immunoturbidimetric assay, performed with a Sysmex CA-1500 instrument (Sysmex Corporation, Kobe, Japan). The Innovance D-Dimer kit and its quality control materials and calibrators were produced by Siemens AG (Munich, Germany). According to the manufacturer’s instructions, a value of 0.5 mg/L fibrinogen equivalent units was selected as the threshold for excluding thromboembolic diseases. The patients were segregated on the basis of their serum.
Detection of binding to cardiolipin by modified (serum-free) ELISA: In order to eliminate β2GPI from a standard CL ELISA, antibody combinations were first expressed in a serum-free postelectroporation medium containing Ultroser G (Gibco, Paisley, United Kingdom) in place of fetal calf serum (FCS). A modified CL ELISA was performed by replacing 10% FCS with 10% Bovine Serum Albumin (BSA) (Sigma, Poole, United Kingdom) in each relevant step. The method was otherwise identical to the standard CL ELISA.
Free protein S levels were determined using the Asserachrom Free Protein S immunoassay (Diagnostica Stago), which utilizes a monoclonal antibody sandwich technique. High-sensitivity C-reactive protein (hs-CRP) concentration was determined by immunonephelometry (Cardiophase hs-CRP; Siemens Healthcare Diagnostics Products GmbH, Marburg, Germany) on a BN ProSpec nephelometer according to the manufacturer’s procedures. Inter and intra-assay coefficients of variation were less than 6%.
Statistical Analysis
Excel software and SPSS version 19 were used. Nominal and dichotomic variables were reported as percentages and quantitative variables having a normal distribution were reported as mean and standard deviation. Correlation analysis was done with the Spearman correlation test. A significant statistical difference was considered when a P > .05 value was reached.
Results
Files from 655 individuals were obtained; however, only 334 had the complete set of data. One hundred fifty-eight (47%) files were from women and 176 (53%) were from men. The average age was of 51 (19) years. Determination of the other prothrombotic biomarkers and thrombosis was present in 63% of these reports. Of the 334 individuals with complete data, 212 patients have had thrombosis, and out of these, 16 patients (8%) have had AMI and 65 patients (31%) have had PE.
The clinical characteristics of the patients divided by gender are shown in Table 1. There were significant differences in age (P = .02), total cholesterol (P = .01), high-density lipoprotein cholesterol (P = .0001), and smoking habits (P = .08). The distribution of thrombophilic biomarkers in patients with and without thrombosis, AMI, and PE is shown in Table 2. In patients with AMI, the frequency of high Hcy levels (>12.4) was statistically higher than in patients without it. Additionally, in patients with PE or DVT, the presence of positive anticardiolipin and elevated D-dimer and of mutations on Leiden factor V was higher than in patients without these diseases (P ≤ .05). The distribution of the genotypes according to the presence of thrombosis, to its type, and to the presence of AMI, in both the C677T and the A1298C polymorphisms, is shown in Table 3. In the C677T polymorphism, there was a statistically significant difference in the CC genotype against the TT genotype (P = .003) and in the CT genotype versus the TT genotype (P = .009), as well as in the allele T (P = .003) in patients with thrombosis. In patients having pulmonary thromboembolism (PTE), there was a statistical difference between the CC genotype and the TT genotype (P = .038). Regarding the A1298C polymorphism, the highest frequency was found in the AA genotype in comparison to the AC and CC genotypes; however, there were no statistically significant allelic or genotypic differences between groups.
Demographic Characteristics of Patients.a
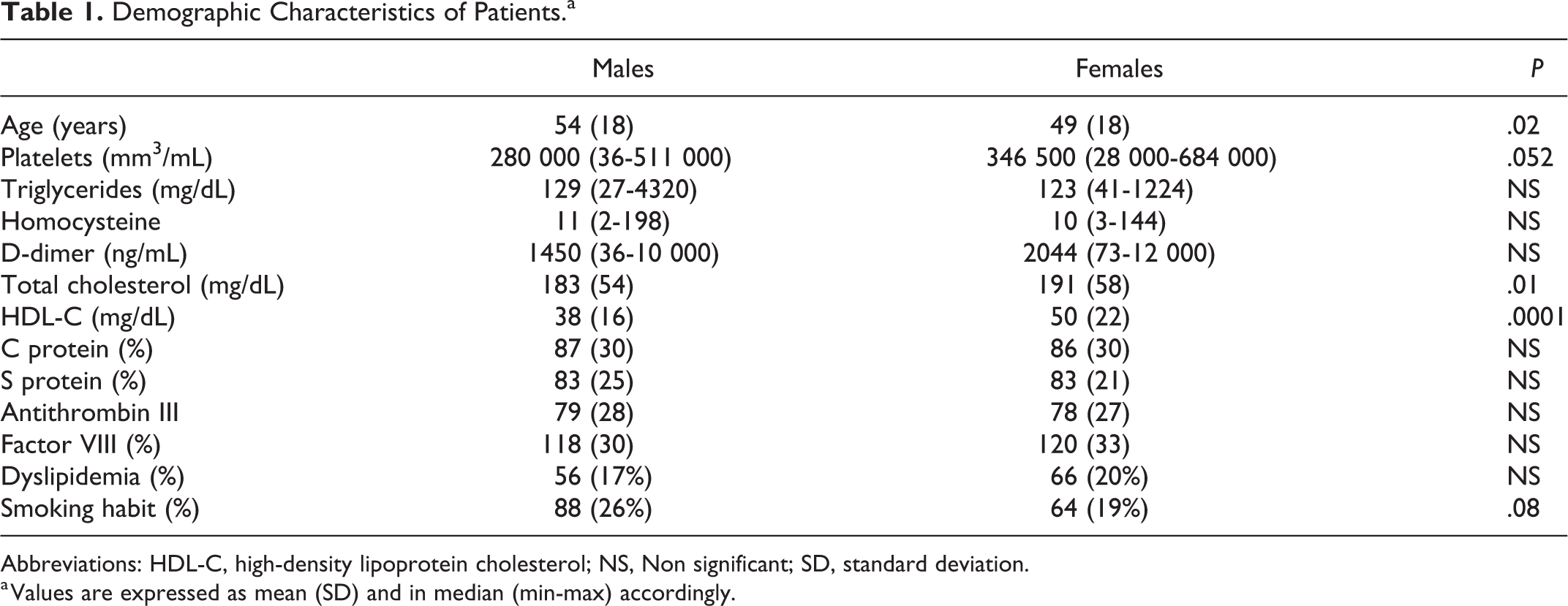
Abbreviations: HDL-C, high-density lipoprotein cholesterol; NS, Non significant; SD, standard deviation.
a Values are expressed as mean (SD) and in median (min-max) accordingly.
Distribution of Thrombophilia Biomarkers in Patients With and Without General Thrombosis, Acute Myocardial Ischemia, and Pulmonary Thromboembolism.

Abbreviations: AMI, acute myocardial ischemia; DVT, deep venous thrombosis; PTE, pulmonary thromboembolic; NS, Non significant.
Genotypic and Allelic Frequencies of the C677T and A1298C Gene According to the Type of Disease.

Abbreviations: AMI, acute myocardial ischemia; DVT, deep venous thrombosis; PTE, pulmonary thromboembolism.
a 0.05 compared between groups allel vs C.
b P < .05. Compared between groups with and without lesion between the same genotypes or alleles.
The results from the evaluation of the association between seric Hcy concentration, the MTHFR polymorphisms studied, and the different types of thrombosis are shown in Table 4. There were significant differences in patients having MTHFR C677T against the total population in the CC genotype against the TT genotype (P = .004) and the C versus T allele (P = .044). In patients having thrombosis versus the MTHFR genotypes, a difference between the CC genotype and the CT and TT genotypes was present (P = .009 and .003, respectively) in the T allele (P = .047). Furthermore, in PTE, there was a difference in CT genotype and the TT genotype (P = .038). Regarding MTHFR A1298C, there were no statistically significant differences in any of the lesions studied.
Total Seric Homocysteine Concentration According to the Genotype MTHFR C677T and MTHFR A1298C.

Abbreviations: AMI, acute myocardial ischemia; DVT, deep venous thrombosis; PTE, pulmonary thromboembolism; Seric Hcy, Seric homocysteine.
a P ≤ .05.
When the analysis between the genotypic frequencies according to the type of thromboembolism and the levels of Hcy was done, there was an increase in Hcy and massive and submassive thromboembolism when compared to segmentary and subsegmentary thromboembolism in C677T TT (P = .003) and in AA 1298 (P = .017; Table 5).
Relation Between the Genotype and the Type of Pulmonary Thromboembolism According to the Levels of Homocysteine.
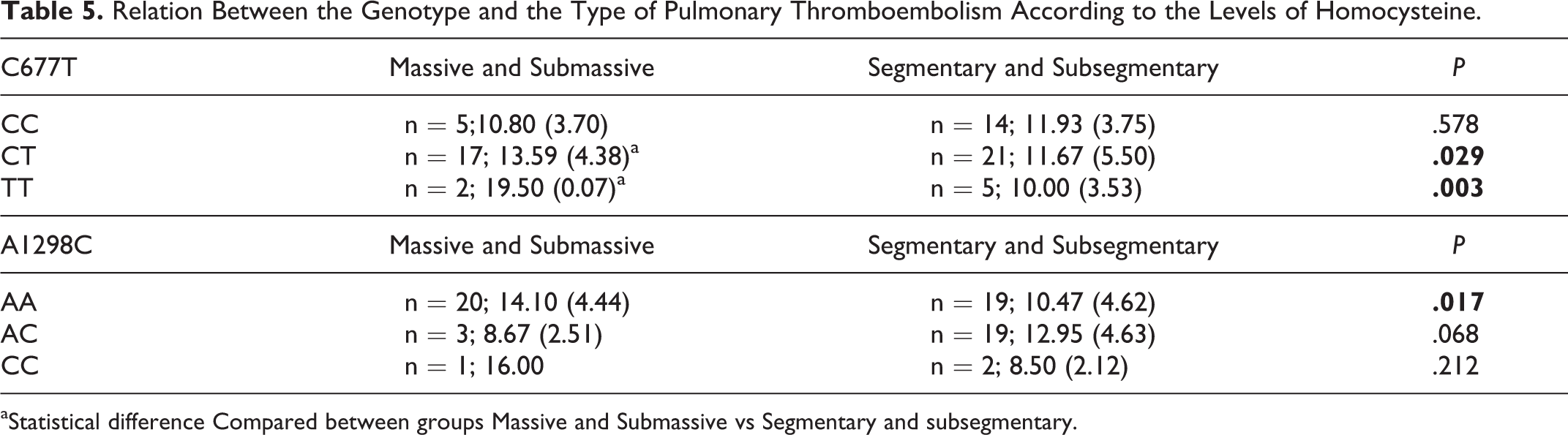
aStatistical difference Compared between groups Massive and Submassive vs Segmentary and subsegmentary.
Gestational losses happened in 8 (2%) women and the Hcy levels were 7 (4). Only in 2 women, there were recurrent losses and the Hcy levels were 12 and 10.
In this study, 20 patients had autoimmune diseases and 9 had neoplastic diseases. Out of the patients with cancer, there was thrombosis at different locations in 5. There was AMI and PTE in only 1 case. From the patients having cancer, 1 had endometrial cancer and all of them had elevated Hcy levels. All cases having thrombosis in other places than the myocardium or lungs were homozygous for the AA allele of the A1298C polymorphism and heterozygous for the CT in the C677T polymorphism. The cases having AMI or PE were homozygous for the AA of the A1298C gene and homozygous for the CC allele of the C677T (Table 6).
Neoplasic and Autoimmunity Diseases, Genotype of MTHFR Gene and Thrombosis Site.
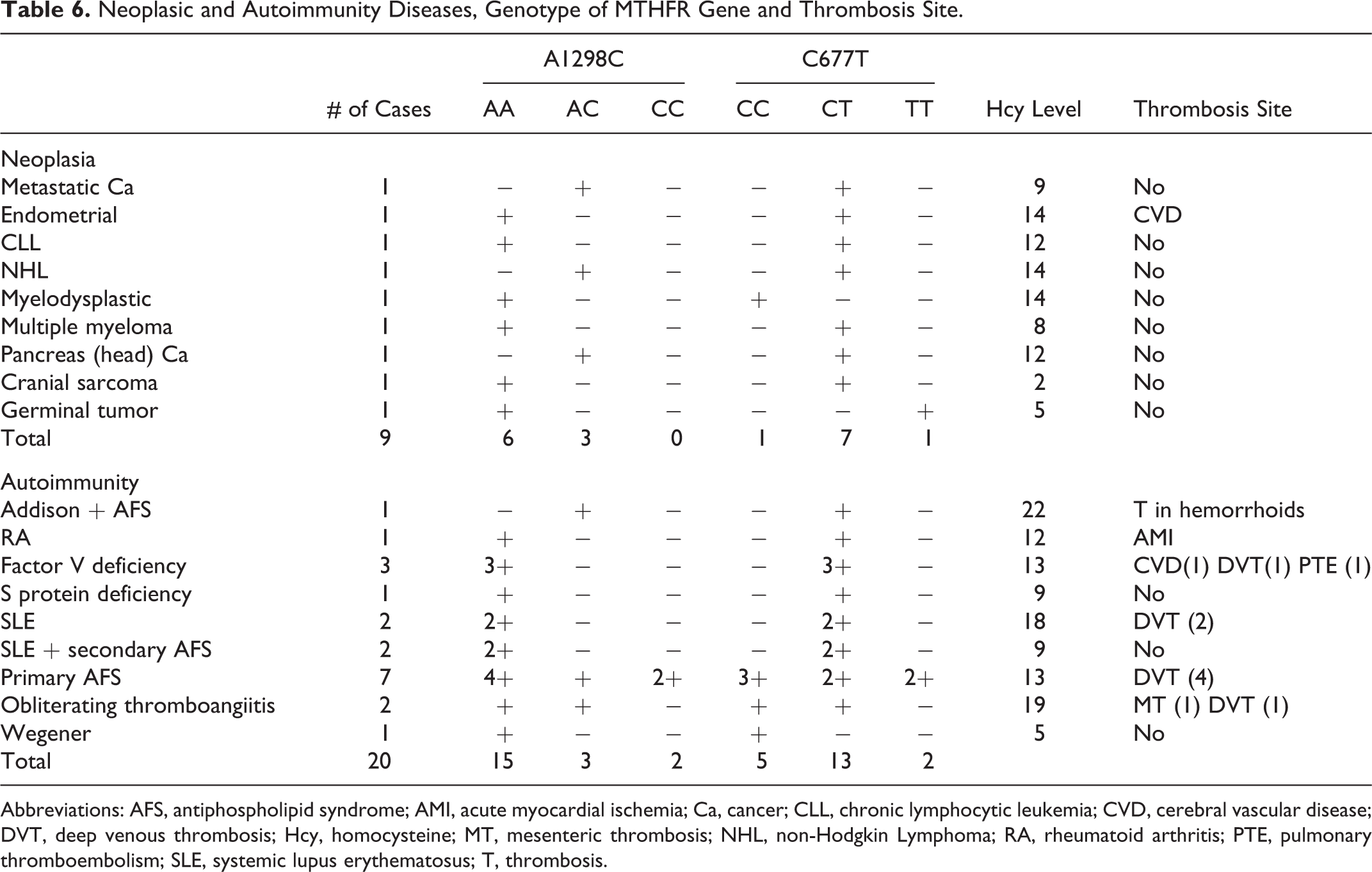
Abbreviations: AFS, antiphospholipid syndrome; AMI, acute myocardial ischemia; Ca, cancer; CLL, chronic lymphocytic leukemia; CVD, cerebral vascular disease; DVT, deep venous thrombosis; Hcy, homocysteine; MT, mesenteric thrombosis; NHL, non-Hodgkin Lymphoma; RA, rheumatoid arthritis; PTE, pulmonary thromboembolism; SLE, systemic lupus erythematosus; T, thrombosis.
There were brain vascular ischemic events or brain hemorrhagic events in 36 cases out of the 115 cases studied: 3 were homozygous in the A1298C gene, 1 in the C677T, and 6 and 12 were heterozygous, respectively. Thrombosis recurrence in the same or another location happened in 40 (12%) patients.
Discussion
Methylenetetrahydrofolate reductase plays an important role in the regulation of the Hcy levels. An increase in Hcy has been associated with ischemic pathology, Alzheimer, dementia, osteoporosis, and psychiatric disorders. 21 –23
In the present study, the increases in Hcy levels were associated with the presence of the genotype 677TT and with the T allele in the general population and there was a significant difference in patients having thrombosis. This association had been previously reported and the Hcy elevation seemed to have a marked influence upon every disease. 24
Information regarding the prevalence of polymorphisms of the thermolabile variant of MTHFR differs greatly from one paper to another. The substitution of 677 C>T results in an amino acid change from alanine to valine in the 225 codon. This substitution diminishes the enzyme’s activity in 35% of patients having the 677CT variant and in 50% to 70% of patients having the 677TT variant. 25 This increase is related to elevated Hcy levels and to a higher thrombotic and cardiovascular risk in the Mexican population and in other ethnic groups. 26 –30
Patients with 677TT and 1298CC polymorphisms have elevated Hcy levels, independently of whether they have thrombosis or not. 31 These findings are in agreement with our results on the T allele in patients with high seric Hcy levels. In these patients, there was a tendency to elevate Hcy levels in the presence of the 677T polymorphism independently of their thrombotic condition. Recent studies in patients with DVT or PE have shown that there is an increased risk of arterial disease and an important risk of PE in heterozygous patients with the genic polymorphism C677T of MTHFR where the cytosine is substituted by thymidine in the 677 nucleotide of the gene (C677T). This is also true in other thrombotic diseases such as congenital heart disease. 32 Furthermore, it is in accordance with the data found in the present study. A high frequency of the C677T polymorphism has been found in Mexico varying from 44% to 58%, but the implication on cardiovascular risk had not been previously reported. 26 –30
An association of elevated Hcy in the presence of thrombosis was confirmed by this study. The A1298C and C677T polymorphisms of the MTHFR gene are associated with a higher risk of venous thromboembolism. 33 In our series, this combination was present in patients having non-Hodgkin lymphoma and this finding would deserve to be further investigated. 34
In this series of patients, those having autoimmune diseases or neoplasms had elevated Hcy levels. The frequency of autoimmunity was 6%, and in these patients, there was thrombosis in different locations. However, one patient had AMI and another PE and both were homozygous for A in the A1298C gene and homozygous for the allele C of C677T. Out of the patients having cancer, only 1 patient developed thrombosis manifesting as VDT.
Another clinical aspect associated with thrombosis and increased Hcy levels is recurrent pregnancy losses and infertility. 35 –38 In this series, 8 women experienced fetal losses, out of whom 5 (62%) had a mutation in C677T and 2 had recurrent abortions. In the remaining 3, there was a mutation in A1298C and elevated Hcy levels. This result is similar to the one reported in the Hindu population, although in that study alterations in the plasminogen activator factor plasminogen activator inhibitor-1 PAI-1 were also found. 39 In this series, infertility was present in only 3 women who also had miomatosis and elevated Hcy levels. Elevated Hcy levels in infertility and gestational losses had already been previously found. 40
In patients with primary antiphospholipid syndrome who have moderately high Hcy levels, the heterozygous point mutations in C677T and A1298C of the MTHFR gene have been proposed as the possible causes for the thrombotic disease and also as the cause of the presence of generalized brain lesions and idiopathic hypoparathyroidism. 41 This situation was not found in our cases and could be due to ethnicity and/or to a folate deficiency in the diet.
Recurrence in thrombosis was present in 11% of the cases. Out of these patients, the majority (7%) corresponded to DVT and the remaining 4% corresponded to brain vascular disease, alterations in the retina, and mesenteric artery.
Limitations of the Study
This retrospective revision did not allow for the obtainment of laboratory data on other complementary prothrombotic biomarkers in the cases where the genomic determination had been done. Nevertheless, the number of cases included was enough to report significant data. Another limitation of the present study was that we could not determine the ingestion of folates and B12 vitamin. It is a retrospective study that of course assumes selection bias and therefore the risks cannot be calculated according to each type of thrombosis. Because the lifestyle cannot be planned in the selected individuals we do not know if there is coparticipation of a diet deficit in the food that an individual consumes. We could not analyze the influence of these cofactors that may have an association with the results. Therefore, other controlled assays are required.
Conclusion
Venous thromboembolic disease is associated with the presence of polymorphisms in the gene encoding for the MTHFR enzyme and with elevated Hcy levels. The increase in the Hcy levels in presence of the T allele in the C677T gene and of the A allele in the A1298C gene is associated with AMI and massive and submassive PTE. Multicentric, prospective studies considering ethnicity, cardiovascular risk factors, nutritional habits, lifestyle, and a specific search for the participation of dietary folates are required and should be proposed to determine the relevance of these findings.
Footnotes
Authors’ Note
Eulo Lupi-Herrera and María Elena Soto contributed to the conception and design of the study, drafting the article or revising it critically for important intellectual content, acquisition of data, analysis and interpretation of data, and final approval of the version to be submitted. María Elena Soto, Antonio de Jesús Lugo-Dimas, and Marcela Elizabeth Núñez-Martínez contributed to acquisition of data, drafting the article, translation and revision of the language in English, and revising it critically for important intellectual content.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.