
Abstract
Identification of pulmonary thromboembolism (PTE), as a cause of syncope, is important and may be life saving. We prospectively analyzed data on 335 patients with acute PTE. Relationships between syncope secondary to acute PTE and clinical findings, risk factors, and imaging modalities were analyzed. Of the 335 patients, 36 (10.7%) had syncope at presentation. Compared to patients without syncope, those with syncope had a higher frequency of right ventricular (RV) dysfunction (94.3% vs 72.1%, respectively; P value = .004) and saddle embolism (24.2% vs 10.9%, respectively; P value = .044). Frequency of RV dysfunction was similar between patients with and without saddle embolism. Although not significant, more patients with syncope had a history of previous PTE (P value = .086). By multivariable analysis, RV dysfunction and saddle embolism were independent correlates of syncope in patients with PTE. In-hospital mortality was not significantly different between the groups. In conclusion, among patients with PTE, RV dysfunction and saddle embolism were the independent correlates of syncope.
Introduction
Pulmonary thromboembolism (PTE) is a potentially fatal disease with clinical presentations ranging from a hemodynamically unstable state to a silent disease. 1 The signs and symptoms of PTE vary widely, 2 with the most common presenting symptoms being dyspnea, chest pain, and syncope. 1 The prevalence of syncope as a presenting symptom in patients with PTE ranges from 2.2% to 40%. 3 The different mechanisms of syncope associated with PTE have been described, including acute right ventricular (RV) failure leading to arterial hypotension, cerebral hypoperfusion, arrhythmia, and vasovagal reflex. The presence of syncope is deemed by some as an inclusion criterion for more invasive therapies, 4,5 but some other authors do not regard it as a poor prognostic factor. 6
Pulmonary thromboembolism is a potentially fatal disorder and its identification and appropriate treatment may prove life saving. In addition, syncope is a relatively common cause of hospital admission, and it may be difficult to assign a specific etiology to it. Taken together, the identification of PTE as a cause of syncope is of great importance and may prevent loss of life.
In the present study, we reviewed clinical and diagnostic testing parameters of patients with PTE and investigated factors with significant contribution in the occurrence of syncope in these patients.
Method
We prospectively studied 335 consecutive patients with a diagnosis of acute PTE admitted to our hospital, a tertiary care teaching hospital, between September 2007 and September 2012. Patients who developed PTE during their hospitalization in our center were not included. The study was approved by the local institutional review board.
Pulmonary thromboembolism diagnosis was confirmed via pulmonary spiral computed tomography angiography (CTA) scan by the demonstration of partial or complete filling defects in the pulmonary circulation in the majority of the patients. Otherwise, the diagnosis was confirmed by ventilation perfusion scan. 7 The classification of PTE based on pulmonary spiral CTA scan was comprised of saddle PTE (if the thrombus was lodged at the level of the bifurcation of the pulmonary trunk and extended into both main pulmonary arteries), central PTE (if the thrombus involved the main branches through the segmental branches), and peripheral PTE (if the thrombus involved the segmental and subsegmental branches). Patients who had clinical contraindications to pulmonary spiral CTA scan underwent ventilation perfusion scan.
Two-dimensional and Doppler echocardiographic examinations were performed within 48 hours of admission by experienced operators. All the quantifications were performed in accordance with the recommendations of the American Society of Echocardiography Committee. 8 The RV dilation was defined as an RV diameter >34 mm, and RV systolic dysfunction was defined as tricuspid annular plane systolic excursion <16 mm or pulsed Doppler peak velocity at the tricuspid annulus <10 cm/s. 8 The term “RV dysfunction” was defined as the dilation of the RV or the presence of RV systolic dysfunction.
The presence of deep vein thrombosis (DVT) was evaluated by the venous ultrasound of the leg veins in clinically suspected patients. 7 Hypotension was defined as a systolic arterial pressure <90 mm Hg on presentation. Syncope was defined as the temporary loss of consciousness with spontaneous recovery.
Statistical Analysis
The continuous variables are expressed as mean ± standard deviation or median (range or interquartile range) and were compared using the Student t test or the Mann-Whitney U test, as appropriate. The normality of the continuous variables was checked using the Kolmogorov-Smirnov test. The discrete variables are expressed as frequencies and percentages and were compared using the chi-square or the Fischer exact test, as required. A multivariate logistic regression model with a backward elimination method was performed to identify the independent predictors of syncope in the patients with PTE. Factors with considerable differences between the patients with and without syncope (P value < .10 in the univariate analysis) were allowed to enter the multivariate analysis. The associations are presented as odds ratios (ORs) with 95% confidence intervals (CIs). Model discrimination was measured using the area under the receiver–operating characteristic (ROC) curve. A P value ≤ .05 was considered statistically significant. The statistical analyses were conducted using SPSS software, version 13.1, (SPSS Inc, Chicago, Illinois).
Results
The study population consisted of 335 patients with a mean age of 60.36 ± 16.77 years. The majority of the patients were male (188 patients, 56.1%). At the time of presentation, 121 (57.1%) patients had at least 1 risk factor for PTE. These factors were comprised of obesity, history of cerebrovascular accident, history of cancer, surgery during the recent 4 weeks, history of immobilization more than 3 days, and history of previous DVT and PTE. The most common risk factor in our patients was bed rest for more than 3 days (27.8%). At presentation, 320 (95.5%) patients experienced at least 1 symptom of dyspnea, cough, chest pain, palpitation, or hemoptysis. The most common presenting symptom was dyspnea in 297 (88.7%) patients. Eight (2.4%) patients had altered mental status and were lethargic. Syncope was the presenting symptom of PTE in 36 (10.7%) patients.
The patients were divided into 2 groups based on the presence of syncope at presentation. Fewer patients with syncope experienced pleuritic chest pain than did those without syncope (16.7% vs 33.8%; P value = .037). Other signs, symptoms, and electrocardiographic findings did not significantly differ between the 2 groups (Tables 1 and 2). A total of 97 (29.0%) patients received thrombolytic therapy (using streptokinase); 12 (33.3%) of the patients with syncope and 85 (28.4%) of those without syncope, with no significant difference.
Characteristic of 335 Admitted Patients due to Pulmonary Thrombotic Emboli.
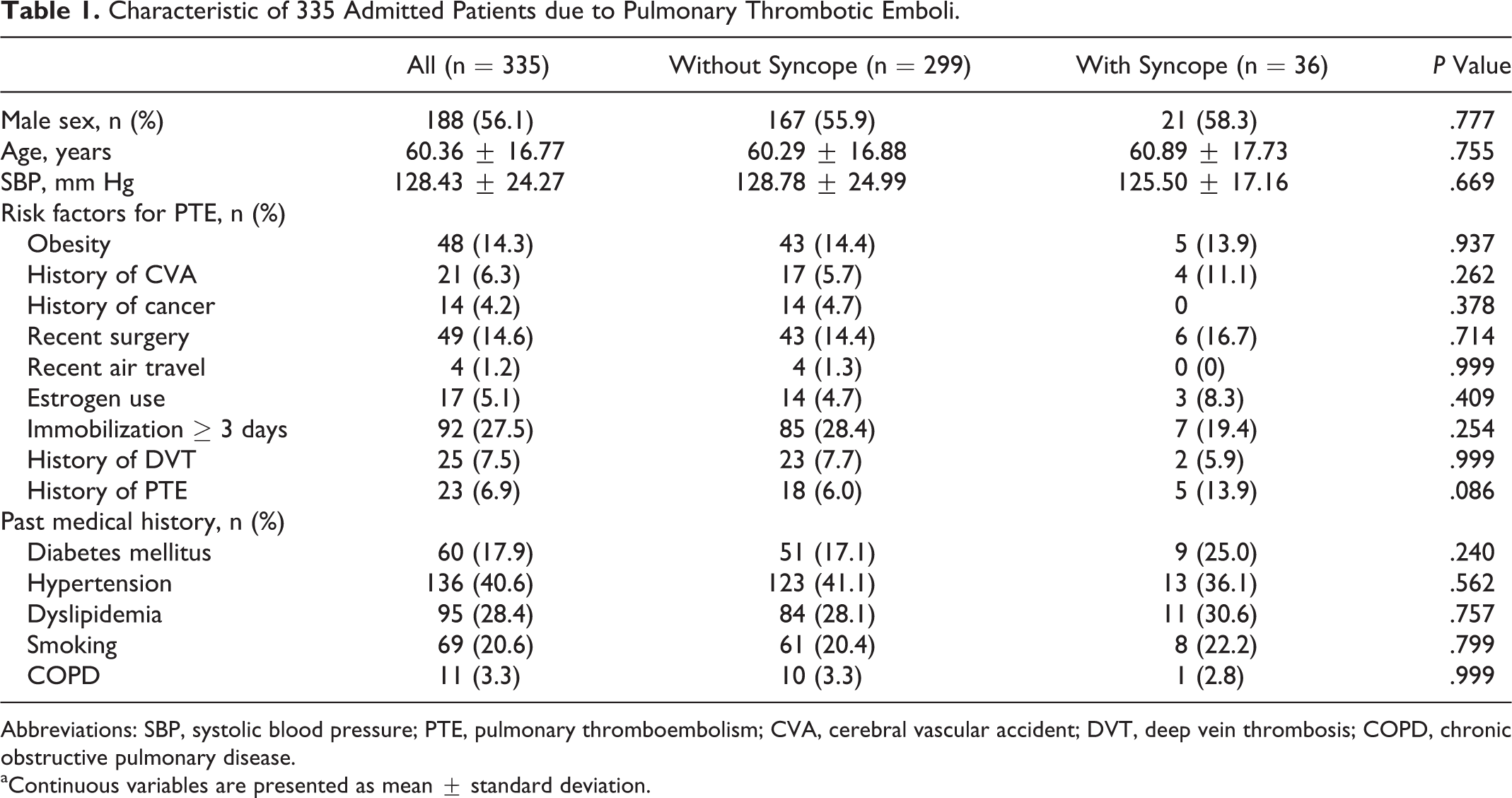
Abbreviations: SBP, systolic blood pressure; PTE, pulmonary thromboembolism; CVA, cerebral vascular accident; DVT, deep vein thrombosis; COPD, chronic obstructive pulmonary disease.
aContinuous variables are presented as mean ± standard deviation.
Clinical Characteristic of 335 Patients With Pulmonary Thrombotic Emboli.
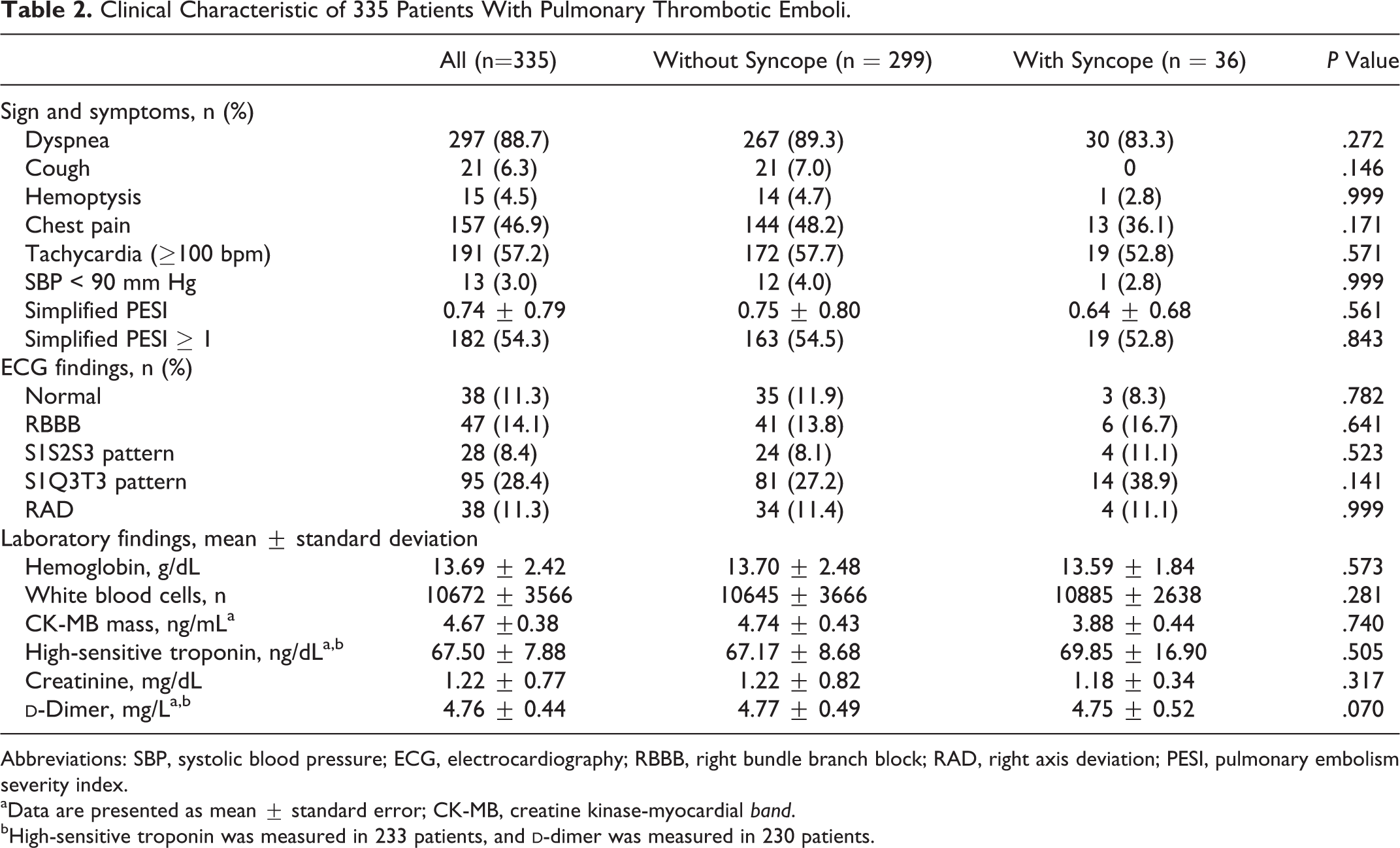
Abbreviations: SBP, systolic blood pressure; ECG, electrocardiography; RBBB, right bundle branch block; RAD, right axis deviation; PESI, pulmonary embolism severity index.
aData are presented as mean ± standard error; CK-MB, creatine kinase-myocardial band.
bHigh-sensitive troponin was measured in 233 patients, and
Previously known risk factors for PTE were not significantly different between the 2 groups (Table 1). Immobilization ≥3 days was the most common risk factor in both the groups, without significant difference. Among the 335 patients, 92 had immobilization ≥3 days due to recent surgery (40.2%), physical disability including lower extremity fracture and casting (31.5%), recent admission secondary to general diseases (5.4%), neurologic disorders including cerebrovascular accident (10.9%), and other causes (12.0%). Compared to the patients without syncope, those with syncope had more than a 2-fold higher rate of history of PTE, although the difference was not significant (P value = .086).
Imaging diagnostic assessment was performed for the patients as follows: echocardiography for 318 patients, spiral CTA for 300, ventilation perfusion scan for 35, and color Doppler sonography for 218 patients. Table 3 compares the imaging findings between the patients with and without syncope. The presence of DVT or its location (proximal or distal involvement) was not associated with syncope. There were 9 patients with DVT and syncope, 5 of these patients had proximal lower extremity DVT (70%). In contrast, in the other group, 58 (67.0%) patients of 86 without syncope had proximal lower extremity DVT. This difference, however, did not constitute statistical significance. Echocardiography within the first 48 hours after admission showed a significantly higher rate of RV dysfunction among the patients with syncope (94.3% vs 72.1%; P value = .04).
Imaging Findings of Patients with Pulmonary Thrombotic Emboli.
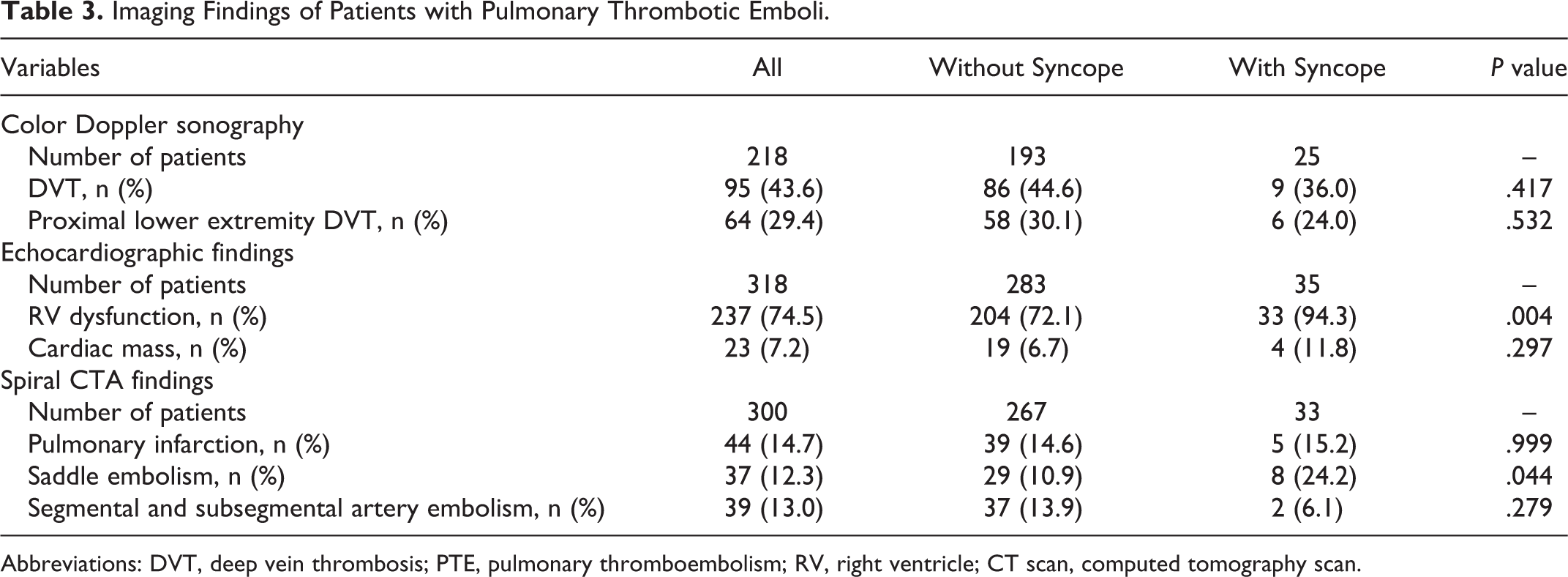
Abbreviations: DVT, deep vein thrombosis; PTE, pulmonary thromboembolism; RV, right ventricle; CT scan, computed tomography scan.
Pulmonary thromboembolism was confirmed by spiral CTA in 300 patients. The patients with syncope were less likely to have pleural effusion (3.7% vs 17.3%; P value = .037). Thrombi were limited to the segmental and subsegmental pulmonary arteries in 39 (13.0%) patients and saddle PTE in 37 (12.3%) patients. The frequency of RV dysfunction was not different between the patients with and without saddle emboli (86% vs 73.3%, respectively; P value = .097). The presence of saddle emboli was significantly higher in the patients with syncope (24.2% vs 10.9%; P value = .044; Table 3).
During hospitalization, 24 (7.2%) patients died; 22 (7.4%) patients among those without syncope and 2 (5.6%) patients in the group with syncope. There was no significant difference between the 3 groups with regard to in-hospital mortality (P value = .999).
To determine the independent factors associated with the presence of syncope in the patients with PTE, the following variables were entered into the multivariate analysis: saddle emboli, RV dysfunction, and previous PTE. According to the results of the analysis, RV dysfunction (OR: 11.17, CI: 1.49-83.60; P value = .019) and saddle emboli (OR: 2.36, CI: 0.95-5.84; P value = .064) were the independent correlates of the occurrence of syncope in the patients with PTE. The final model had a P value of .358 for the Hosmer-Lemeshow test and an area under the curve of 0.670 (CI: 0.579-0.761) with a P value of .002.
Discussion
In this study, the prevalence of syncope was 10.7%. The previously known risk factors for PTE were not significantly different between the 2 groups. The patients with syncope had higher rates of RV dysfunction, saddle embolism, and previous history of PTE. Among them, RV dysfunction, followed by saddle emboli, was the strongest correlate of syncope in the patients with PTE.
The prevalence of syncope in this study is close to the findings of Calvo-Romero et al 9 but is lower than the findings of some other studies. 10 –12 The reason is that many patients tend to regard syncope as a neurologic rather than a cardiologic symptom and, thus, refer to general hospitals and not subspecialty cardiac centers.
It has been shown that systolic blood pressure and RV dysfunction are the major known determinants of risk stratification at presentation. 13 –15 In our study population, RV dysfunction was independently associated with the occurrence of syncope in the patients with PTE while systolic blood pressure at presentation did not correlate with syncope. In the earlier studies, hypotension was more commonly seen in patients presenting with syncope, 6,16,17 but it seems that the prevalence of hypotension in patients with PTE presenting with syncope has progressively decreased over time because in earlier studies PTE was probably only suspected in patients with unstable hemodynamics on presentation. However, Castelli et al 16 found no higher frequency of RV dysfunction in patients presenting with syncope and PTE. In addition, the impact of age on the clinical presentation of PTE has been studied, 18 and it has been concluded that the clinical presentation of PE could be subtle or atypical in the elderly patients. This could emerge as a high clinical suspicion in order to prevent delays in the diagnostic workup and the initiation of appropriate treatment. However, in the present study, we did not observe a significant difference in terms of age between the patients with and without syncope.
In the present study, both saddle embolism and RV dysfunction were independently associated with syncope presentation. Saddle embolism in spiral CTA indicates a large thrombus burden, which is responsible for the occurrence of PTE. A large thrombus in the pulmonary artery and its main branches can trigger syncope via vasovagal reflex. Acute RV failure due to acute central pulmonary vascular occlusion with the resultant impaired left ventricular filling and reduced cerebral flow is another major mechanism for syncope in patients with PTE, and the greater prevalence of RV dysfunction in our patients with syncope supports this mechanism. Be that as it may, the time delay between syncope and admission, between admission and PTE diagnosis, and between diagnosis and performing echocardiography may influence the actual frequency of acute RV dysfunction.
Although the prognostic value of syncope has not been specifically focused on, the presence of syncope has generally been considered a poor prognostic factor 19 among patients with PTE. In addition, the prognostic significance of the clot burden in the pulmonary embolism is still controversial. 20,21 In the present study, we found no significant correlation between syncope and in-hospital mortality and simplified pulmonary embolism severity index score. Similar to our study, Calvo-Romero et al 9 reported that in-hospital mortality did not differ between patients with syncope and patients without syncope and concluded that syncope did not seem to determine a poor prognosis. The recognition of low-risk patients eligible to early hospital discharge is possible with current risk stratification schemes along with selected prognostic parameters. 22 Syncope presentation may not increase in-hospital mortality, but its significant association with RV dysfunction renders the early discharge and outpatient treatment of these patients unacceptable.
Limitations
One of the limitations in this study was its relatively small sample size, leading to the inclusion of a small number of patients in the syncope group, which may influence the results. In addition, patients in severe conditions who died prior to admission or before confirmed PTE diagnosis were not included in the study. Another drawback of note is that pulmonary spiral CTA scan was not performed for all the patients. Moreover, immediate echocardiographic and hemodynamic evaluations after syncope were not possible.
Conclusion
The presentation of syncope in our patients with PTE was significantly associated with RV dysfunction and to some degree with saddle embolism confirmed by pulmonary spiral CTA. Nonetheless, we did not observe a significant correlation between syncope and other clinical and imaging modality (echocardiography and color Doppler sonography) findings.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.