
Abstract
The use of cardiopulmonary bypass (CPB) in cardiac surgery often leads to a systemic inflammatory response. Up to 25% of patients undergoing CPB for cardiac surgery are reported to develop vasoplegic syndrome in the acute postoperative period, in which the patients are refractory to vasopressors. The purpose of this study is to assess vitamin D deficiency as a risk factor for vasoplegia after using CPB. We performed a retrospective review of 1322 patients undergoing adult cardiac surgery requiring CPB. Forty-six patients with previously recorded 25-hydroxy vitamin D (25(OH)D) levels within 6 months of surgery met the conditions of this study. The mean level of 25(OH)D was 32.7 ng/mL (standard deviation [SD] = 15.1). The mean age of patients was 67 (SD = 10.1) years old, most were male (63%) and white (78%). Average CPB time was 140 ± 44 minutes. Postoperative vasopressor use was compared to individual preoperative 25(OH)D levels. As a secondary end point, postoperative vasopressor use and vasoplegia were analyzed between 3 groups: Vitamin D deficient defined as 25(OH)D ≤20 ng/mL (n = 7), vitamin D insufficient defined as 25(OH)D between 20 and 29 ng/mL (n = 15), and vitamin D sufficient defined as 25(OH)D ≥30 ng/mL (n = 24). There was no correlation between vitamin D levels and postoperative vasopressor use. The mean doses of postoperative vasopressor use were 0.088 µg/kg/min (standard error of the mean [SEM] = 0.032), 0.085 µg/kg/min (SEM = 0.037), and 0.072 µg/kg/min (SEM = 0.024) of norepinephrine equivalents for the vitamin D deficient, insufficient, and sufficient groups, respectively. Incidence of vasoplegia for each group was the following: 0.143 for vitamin D deficient, 0.067 for vitamin D insufficient, and 0.125 for vitamin D sufficient. In this pilot study, there does not appear to be a relationship between vitamin D and vasopressor use following cardiac surgery utilizing CPB; however, there appears to be a trend toward an increased vasopressor usage in patients with decreased vitamin D levels. A larger sample size and a prospective analysis are warranted to further assess the significance of the relationship between vasoplegia and vitamin D deficiency. With further investigation, vitamin D has the potential to become a low-cost, low-risk therapeutic for improving outcomes in CPB surgery.
Introduction
Cardiopulmonary bypass (CPB) in cardiac surgery is associated with a brief systemic inflammatory response that is likely due to blood contact with the artificial surfaces of the bypass machine. 1 –3 This intense inflammatory reaction can lead to pathologic vasodilation and induce a state of vasoplegia, in which patients are refractory to vasopressors. Up to 25% of patients undergoing CPB for cardiac surgery are reported to develop vasoplegic syndrome in the acute postoperative period. 4 Identifying risk factors that predispose patients to vasoplegia would likely reduce the incidence of vasoplegic syndrome and its associated morbidity and mortality. There is a growing body of support that suggests low vitamin D levels may be one of these risk factors. 5
There has been an increasing interest in the role of vitamin D in cardiovascular health. Graham et al observed that infants with lower levels of vitamin D after CPB required more inotropic agents postoperatively; therefore, concluding that vitamin D may play a role in cardiac contractility. 6 There was an effect of vitamin D associated with cardiac myocyte function; however, there may be a similar effect at the vascular level. That being said, Bukoski and Xue showed vitamin D supplementation in rats gave an increased vascular contractile response upon stimulation with vasopressors. 7
Vitamin D has been shown to have a role in related systemic inflammatory states namely sepsis. Sepsis has recently been shown to occur more often in vitamin D deficient individuals. 8 A full understanding of the role of vitamin D in the circulatory collapse seen in sepsis has not yet been determined; however, we hypothesize that vitamin D levels may play a role in the hypotensive state observed in the postoperative period.
The purpose of this study is to assess vitamin D deficiency as a risk factor for vasoplegia after cardiac surgery using CPB. We hypothesize that vitamin D deficiency leads to increased vasopressor use after CPB. We theorize that there is a decreased ability of the vasculature to respond to vasopressors. Our goal is to determine whether preoperative vitamin D levels contribute to increased postoperative vasopressor use in patients after CPB.
Methods
This is a retrospective review of patients undergoing elective or emergent cardiac surgery including coronary artery bypass grafting (CABG), valve replacement/repair, aortic aneurysm repair, and/or congenital adult heart surgery. The patient population is that of the Loyola University Medical Center in Maywood, Illinois. Patient records were reviewed in the electronic medical record. The study was approved by the institutional review board of Loyola University Stritch School of Medicine.
We reviewed 1322 patient files and found 54 patients with previously recorded 25-hydroxy vitamin D levels, 25(OH)D, within at least a 6 month period prior to surgery. Eight of these patients were excluded for one of the following criteria: previous cardiac surgery within the last 2 months, concurrent use of postoperative dobutamine and milrinone, insertion of intra-aortic balloon pump coming off CPB, postoperative cardiac tamponade, serotonin syndrome, or an incomplete chart.
Vitamin D Groups
For secondary analysis, patients were divided into groups defined by their 25(OH)D serum level measured within 6 months of cardiac surgery. The vitamin D deficient group includes patients with ≤20 ng/mL 25(OH)D. The vitamin D insufficient group includes patients with 20 to 29 ng/mL 25(OH)D. The vitamin D sufficient group includes patients with ≥30 ng/mL 25(OH)D. These groups were used to compare postoperative vasopressor use and incidence of vasoplegia.
Vasoplegia
Vasoplegia was defined as the use of multiple (≥2) intravenous (IV) vasopressors at high dose (epinephrine ≥4 µg/min, norepinephrine [NE] ≥4 µg/min, dopamine ≥5 µg/min, vasopressin ≥1 U/h) in the setting of preserved cardiac index seen following surgery. Dobutamine is commonly used in the postoperative setting to maintain an adequate cardiac index. Patients were assumed to have a preserved cardiac index, unless they required both dobutamine and milrinone. Patients receiving only dobutamine were included in the study.
Norepinephrine Equivalents
Brown et al reported a calculation to convert vasopressor doses for epinephrine, NE, vasopressin, dopamine, and phenylephrine into NE equivalents. 9 Of these vasopressors, only NE, epinephrine, and vasopressin were utilized in the postoperative window for the patients in this study. The average infusion rate of each vasopressor was determined and then converted into an NE equivalent rate. Briefly, 1 μg/kg/min of NE is equivalent to 1 μg/kg/min of NE equivalent, 1 μg/kg/min of epinephrine is equivalent to 1 μg/kg/min of NE equivalent, and 1 U/min of vasopressin is equivalent to 5 μg/kg/min of NE equivalent.
Statistical Methods
Prism 7 was used to run the statistical analysis. Chi-squared and analysis of variance were used for comparison of baseline characteristics. Analysis of variance was used for group analysis of the vitamin D groups using standard error of the mean (SEM), due to the small sample sizes. Linear regression was used to plot a line of best fit between 25(OH)D levels and the NE equivalents dosing rate; one outlier was eliminated from the linear regression data plot. Chi-squared was used for comparison of incidence of vasoplegia. Significance was defined as P < .05.
Results
The mean level of 25(OH)D in this cohort was 32.4 ng/mL (standard deviation [SD] = 15.1). The mean age of patients was 67 (SD = 10) years old, most were male (63%) and white (78%). The baseline characteristics and intraoperative factors of the 3 groups are shown in Table 1. Most of the baseline characteristics were shown to be similar between groups, which included sex, hypertension, angiotensin converting enzyme (ACE) inhibitor use, chronic kidney disease stage 3 or greater, current smoker, diabetes mellitus, and chronic obstructive pulmonary disease. Age and race were statistically different between groups; the vitamin D deficient group was younger and had a higher percentage of black or African American patients. The CPB time and aortic clamp time were not statistically significant between groups.
Baseline Characteristics and Intraoperative Factors.

Abbreviations: CKD, chronic kidney disease; COPD, chronic obstructive pulmonary disease; CPB, cardiopulmonary bypass; DM, diabetes mellitus; HTN, hypertension; SD, standard deviation.
Figure 1 shows that there is no correlation between 25(OH)D levels and rate of NE equivalents used (R2 = .001). The slope is not significantly nonzero (P = .83). Among these data, there does appear to be 2 separate groups of patients, regardless of 25(OH)D level—those with very little vasopressor requirements and those with larger vasopressor requirements.
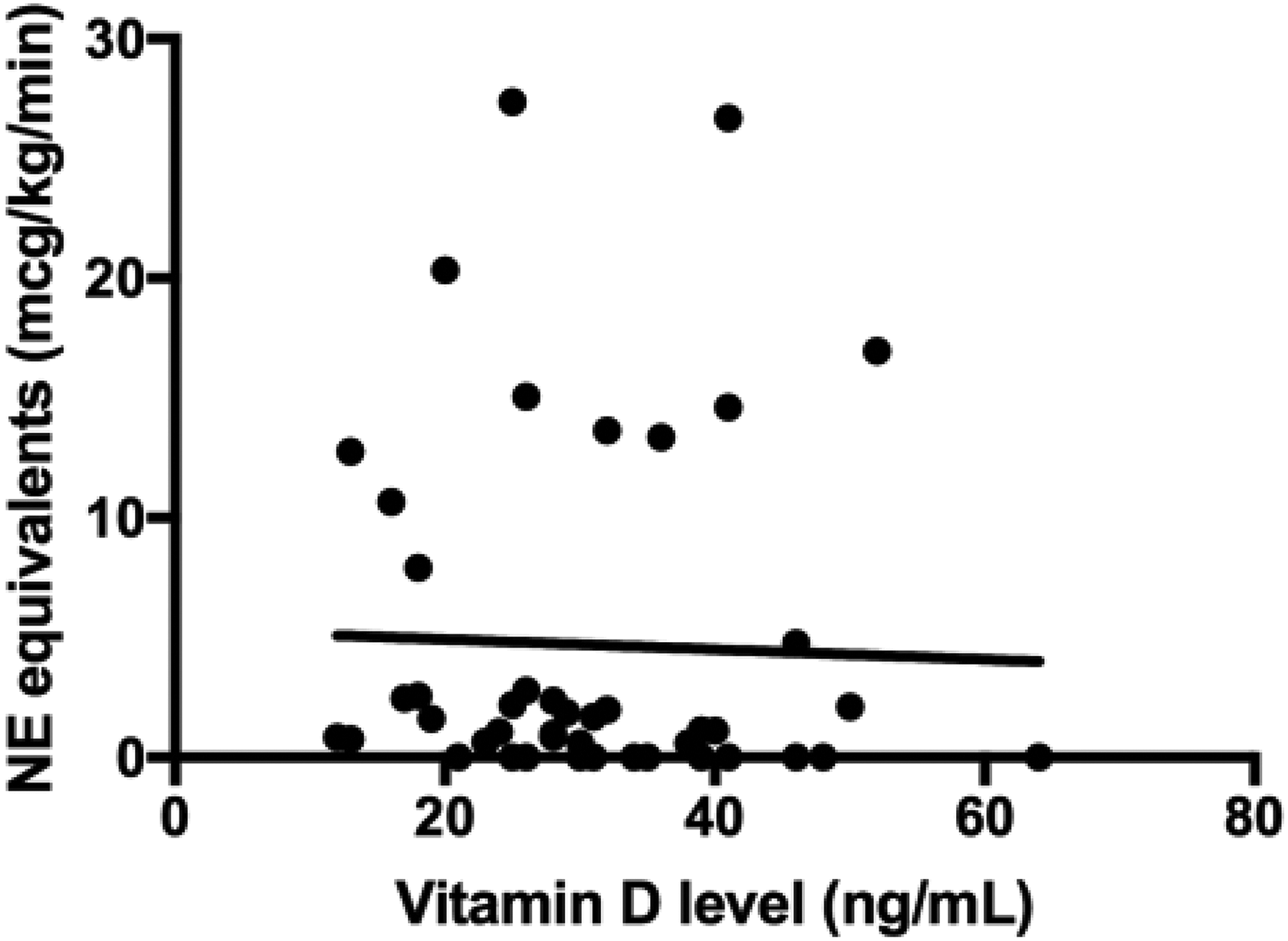
Linear Regression Between Vitamin D (25(OH)D) level and Norepinephrine Equivalent Dose.
Figure 2 shows the average NE equivalents used in each vitamin D group. The mean doses of postoperative vasopressor use for the 25(OH)D groups were 0.088 µg/kg/min (SEM = 0.032) of NE equivalents for the vitamin D deficient group, 0.085 µg/kg/min (SEM = 0.037) of NE equivalents for the vitamin D insufficient group, and 0.072 µg/kg/min (SEM = 0.024) of NE equivalents for the vitamin D sufficient group. The difference between groups was not statistically significant (p = .93).
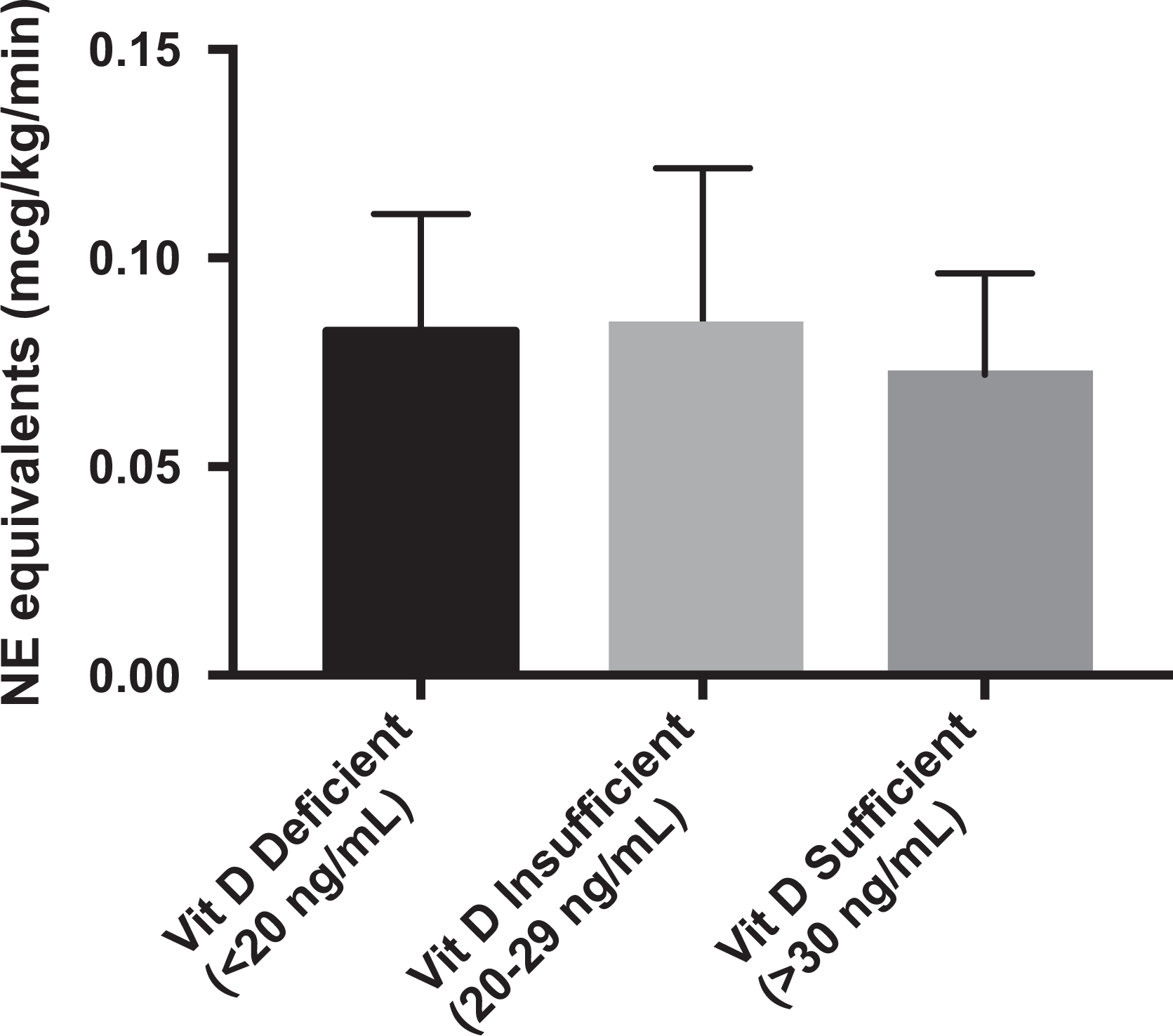
Vitamin D (25(OH)D) Group vs. Norepinephrine Equivalent Dose.
Incidence of vasoplegia between groups was not statistically significant (0.143 for vitamin D deficient, 0.067 for vitamin D insufficient, 0.125 for vitamin D sufficient; P = .82).
Discussion
This is a retrospective pilot study investigating the role of vitamin D deficiency as a risk factor for vasoplegia after CPB. Postoperative vasopressor dosing rate was used to quantify the severity of hypotension exhibited after CPB. This was used for 2 reasons: (1) Measuring the rate of vasopressors administered gave a quantitative number to compare between patients and (2) allowed an indirect way to measure vasoplegia. We found that determining the incidence of vasoplegia with a retrospective lens was not the most ideal and accurate way to assess this unique clinical scenario; therefore, postoperative vasopressor use became our primary outcome and an indirect way of quantifying the underlying nature of this syndrome, which is defined as a state of persistent hypotension with a decreased response to vasopressors in the setting of preserved cardiac output.
There have been many studies in recent years that have identified risk factors for vasoplegic syndrome following cardiac surgery. Levin et al described that a significant drop in mean arterial pressure after starting CPB was associated with a higher likelihood of postoperative vasoplegia. 10 Additionally, they found that procedure type, length of CPB, and European System for Cardiac Operative Risk Evaluation (EuroSCORE) were risk factors for vasoplegia as well. 10 Several studies have identified preoperative treatment with ACE inhibitors as a risk factor for vasoplegia. 11 –13 Other reported risk factors for vasoplegia are preoperative IV heparin use, higher adenosine plasma levels, preoperative ejection fraction <35%, on pump versus off pump CABG, and preexisting endothelial activation reflected by higher levels of von Willebrand factor propeptide and sP-selectin levels. 11,13 –17 The further identification of risk factors for vasoplegia would allow prophylactic measures to prevent this syndrome and decrease the morbidity and mortality associated with it.
Vitamin D deficiency was investigated in the present study as a potential risk factor for vasoplegia. Vitamin D deficiency is very prevalent, ranging from 30% to 50% of the population. 18 It is particularly more common in the elderly population, those with minimal sunlight exposure, and individuals of nonwhite ethnicities. 19 There has been an increasing interest in the role of vitamin D in cardiovascular health. The role of vitamin D in cardiovascular health can also be inferred from the presence of vitamin D receptors on many cell types in the body, including cardiac myocytes, vascular smooth muscle cells, and endothelial cells. 20 Analysis of National Health and Nutrition Examination Survey (NHANES) 2001 to 2004 data showed that vitamin D deficiency, defined by <30 ng/mL, was highly prevalent in US adults with cardiovascular diseases, especially those with coronary heart disease and heart failure. 21 The Framingham Offspring Study observed a greater incidence of cardiovascular disease in individuals with 25-hydroxy-D3 <15 ng/mL. 20 The potential role of vitamin D can be inferred from a study by Bukoski and Xue, which showed vitamin D supplementation in rats, gave an increased vascular contractile response upon stimulation with vasopressors. 7 The higher prevalence of vitamin D deficiency observed in patients with sepsis—a similar clinical picture of pathologic peripheral vasodilation—also supports the investigation of vitamin D deficiency as a risk factor for post-CPB vasoplegia.
In the present study, postoperative vasopressor use did not correlate with preoperative 25(OH)D levels. In subgroup analysis, postoperative vasopressor use was slightly higher in the vitamin D deficient and insufficient groups compared to the vitamin D sufficient group; however, this difference was not statistically significant. Incidence of vasoplegia between groups was also not statistically significant. Due to the study design, we lacked a significant number of patients to adequately test our hypothesis. Although most of the baseline characteristics and intraoperative factors were equal between groups, age and race were statistically different between groups and were likely confounding variables. Despite these limitations, there was a trend toward an increased vasopressor usage in patients with decreased vitamin D levels. This observation warrants further evaluation in a larger prospective cohort.
Treatment for vasoplegia has traditionally been the administration of high-dose vasopressors such as NE, vasopressin, and phenylephrine. The new literature supports the use of methylene blue, which interferes with nitric oxide metabolism, and terlipressin, a synthetic analog of vasopressin. 22 The prophylactic use of methylene blue and vasopressin has gained some recognition as a potential way to decrease postoperative vasoplegia. 23 –25 If vitamin D deficiency is proven to be a significant risk factor for vasoplegia, then preoperative vitamin D supplementation may decrease the incidence and/or severity of this pathologic state of vasodilation. Since vitamin D supplementation is relatively inexpensive and readily available, it could be a highly practical and beneficial resource for improving outcomes after cardiac surgery utilizing CPB.
This pilot study is limited by its retrospective analysis and by components of its study design, such as the 6-month window allowed for preoperative vitamin D levels, the assumption that patients’ vasopressors were titrated to the same blood pressure goals and the relatively small cohort size. Due to the relatively small cohort size, the groups were not matched according to the baseline characteristics that varied between groups, namely age and race. Furthermore, the evaluation of the clinical diagnosis of vasoplegia from a retrospective view may have over or underestimated its incidence.
Future studies on this subject should focus on prospective analysis of vitamin D and vasoplegia, which would allow for a more thorough assessment of vasoplegia incidence. A prospective analysis would also allow the measurement of vitamin D in the immediate preoperative period, allowing for a more accurate determination of vitamin D status heading into surgery. Lastly, both the carrier form of vitamin D, 25(OH)D, and the active form, 1,25-dihydroxycholecalciferol (1,25(OH)2D), should be measured, especially in the setting of renal disease.
Conclusions
In this pilot study, there does not appear to be a relationship between vitamin D and vasopressor use following cardiac surgery using CPB; however, there appears to be a trend toward an increased vasopressor usage in patients with decreased vitamin D levels. A larger sample size and a prospective analysis are warranted in order to further assess the significance of the relationship between vasoplegia and vitamin D deficiency. With further investigation, vitamin D has the potential to become a low-cost, low-risk therapeutic for improving outcomes in cardiac surgery using CPB.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.