
Abstract
Introduction:
Lipid oxidation is a definite feature of atherosclerosis, and oxidized low-density lipoprotein (oxLDL) is not only highly immunogenic but toxic to several cell types. Beta-2-glycoprotein-I (β2GPI) dampens oxLDL toxicity by forming binary oxLDL/β2GPI complexes. We evaluated whether circulating oxLDL/β2GPI complexes are associated to atherosclerosis-related events (ARE) and to venous thromboembolism (VTE).
Methods:
In a cross-sectional case–control study, cases were (a) 57 consecutive patients (male/female [M/F] 33/24, mean age 57 [10] years) attending a thrombosis unit for ARE (myocardial infarction [MI] n = 20, peripheral vascular disease n = 7, and ischemic strokes n = 30); (b) 52 consecutive patients (M/F 22/30, mean age 55 [17] years) attending the same unit for unprovoked (VTE); (c) normal controls comprised 90 participants (M/F 35/55, mean age 41 [15] years); and (d) oxLDL/β2GPI complexes were measured by immunoassay and resulting levels divided into quartiles.
Results:
The odds ratio (OR) of ARE was greater in the fourth and second quartiles than in the first quartile (8.5 and 6.0, respectively); the OR of developing MI was greatest in the fourth quartile (17.8). By multivariable analysis with age, sex, smoking, lipid status, statin, and ARE phenotypes as independent variables and oxLDL/β2GPI as the dependent variable, only MI predicted oxLDL/β2GPI (P < .0001).
Conclusions:
OxLDL/β2GPI may be regarded as a marker of ARE, in particular of MI.
Keywords
Introduction
The notion that oxidized low-density lipoprotein (oxLDL) plays a pathogenic role in early atherosclerosis 1 was followed by the discovery that oxLDL binds in vitro to beta-2-glycoprotein-I (β2GPI) forming stable (nondissociable) but similarly pathogenic oxLDL/β2GPI binary complexes 2 ; indeed, these complexes primarily formed in atherosclerotic lesions are released into the circulation where can be measured reliably. Plasma levels of oxLDL/β2GPI complexes have been shown to predict adverse outcomes and severity of coronary artery disease. 3 The pathogenic role of oxLDL/β2GPI complexes is further supported by their presence in atherosclerotic lesions by in vivo imaging techniques, 4 where they co-localize with immune-inflammatory mononuclear cells and CD4+ lymphocytes. 2 The intracellular accumulation of these complexes by mononuclear cells is mediated by scavenger and specific antibodies via Fcγ receptors. 5,6 These findings support not only a role of these complexes in the initiation but, importantly, in the progression of atherothrombotic disease. The oxLDL/β2GPI complexes have been described in arterial disease in the autoimmune 6,7 and in the nonautoimmune settings, 3,8,9 though there are very scanty data on venous thromboembolism (VTE). 8 To expand on the topic, we evaluated oxLDL/β2GPI complexes in patients with different types of atherosclerosis-related events (ARE) and VTE; because the study was carried out in a hospital-based thrombosis unit where homocysteine (HC) was measured as part of the thrombophilia screen, we also evaluate whether oxLDL/β2GPI bore any relation to plasma HC, known to favor LDL oxidation, 10 and to the activated partial thromboplastin time ratio (aPTTr).
Method
Study Type and Patients
This was a cross-sectional case–control study. Cases were consecutive patients attending the Haemostasis Clinic and the Internal Medicine wards of the Ospedale Riuniti di Foggia for ARE and spontaneous VTE. Inclusion criteria were thrombotic occlusion in any vascular district, peripheral vascular disease, cardiovascular disease, and cerebrovascular disease: In the case of acute occlusions, thrombophilia screening and other specific tests were performed between 3 and 6 months from the event to account for an acute-phase state, whereas blood samples were taken at the time of attendance if an acute event was excluded. Exclusion criteria were active or historical cancer, acute and chronic infectious, inflammatory and autoimmune disorders, acute and chronic renal, hepatic and respiratory disorders, primary/secondary antiphospholipid syndrome, insulin dependent and independent diabetes mellitus, and pregnancy. Controls were of 2 types: (1) hospital controls, participants attending the hospital for various symptoms and diagnosed with minor ailments and (2) healthy controls, patients attending the hemostasis clinic as part of family or personal thrombophilia screening for various reasons. Both control groups underwent the same exclusion criteria as patients. Consecutive patients and controls were invited to participate; consenting patients were enrolled in the study that was carried out according to the declaration of Helsinki and approved by the Ethics Committee of the Ospedale Riuniti of Foggia (Foggia, Italy; (99/CE/2015).
Blood Sampling
All participants were seen between 8.00 and 11.00
Thrombophilia Screening
In all participants, the following were measured: aPTTr, antithrombin, protein C (chromogenic assay, Behring, Marburg, Germany), free protein S antigen (enzyme-linked immunosorbent assay [ELISA]; Diagnostica Stago, Asnieres, France), and plasma HC (Bio-Rad, Oslo, Norway). Normal plasma obtained from 65 blood donors (male/female [M/F] 30/35, mean age 45 [16] years) served as control plasma for aPTTr and natural anticoagulants and to generate reference ranges (mean [2 standard deviation]). The dilute Russel viper venom time (screen and confirm) and the aPTT (with Hemosil RecombiPlasTin 2G as activator) were performed an ACLTOP500 coagulometer (all from Instrumentation Laboratory, Monza, Italy). Immunoglobulin G (IgG) anticardiolipin antibodies were measured by ELISA (Byk Gulden, Italy). Plasma HC was measured by ELISA, where free HC is obtained by hydrolysis of protein-bound HC and then enzymatically converted to S-adenolsyl-
Lipid Profile
The lipid profile was laboratory grade and included total cholesterol (CHO), high-density lipoprotein (HDL), and triglycerides with LDL calculated according to Friedewald equation; an abnormal lipid profile was defined as CHO >200 mg/dL, LDL above 130 mg/dL, HDL <40 mg/dL for men, <50 mg/dL for women, and triglycerides >200 mg/dL or a combination of them.
oxLDL/β2GPI Immunoassay
Plasma oxLDL/β2GPI complexes were measured as previously described. 9 Briefly, IgG2b murine monoclonal antibody (3H3) specific for human β2GPI was coated onto 96-microwell plates and used to capture oxLDL/β2GPI complexes via its reactivity with β2GPI. Diluted patient sample was added to the appropriate microwells for incubation at room temperature for 1 hour. After washing, biotinylated 2E10 antibody (IgG murine monoclonal antihuman Apo B-100) was added to the microwells and incubated for 30 minutes, followed by Streptavidin–horseradish peroxidase for 30 minutes. Color was developed with tetramethylbenzidine/H2O2 for 30 minutes and the reaction stopped with 0.36 N sulphuric acid. Optical density was read at a wavelength of 450 nm (650 nm reference). The oxLDL/β2GPI complex concentration (expressed in U/mL) was calculated against a reference curve built with 3-fold serial dilutions of a reference preparation.
Diagnosis of ARE and VTE
Both ARE and VTE were diagnosed by angiography, magnetic resonance imaging (MRI) and angio-MRI, electrocardiography, and serial cardiac markers measurements as indicated; VTE was diagnosed by Doppler ultrasound, computed tomography (CT) scan, and/or CT angiography as required.
Statistical Analysis
For categorical variables, χ2 test or Fisher exact test was used; for continuous variables, paired t test and Wilcoxon signed rank sum test (when applicable) were used. Association between variables was assessed by univariate analysis (Pearson ρ) and the assumptions of the univariate analysis were tested by multivariable regression. Cochran-Armitage Trend test was used to determine the trend between oxLDL/β2GPI quartiles and odds ratio (OR). Statistical analysis was performed using the JMP 11.2.0 program from SAS Institute Inc, North Carolina.
Results
Participants
The demographics of the patient population are shown in Table 1. The patients with ARE were divided into 3 groups: (1) those with myocardial infarction (MI; n = 20, of which 16 MI proper [twice in 3 patients] and 4 non-ST segment elevation MIs; (2) those with chronic peripheral vascular diseases with an acute occlusion (n = 5) and acute renal artery occlusions (n = 2); and (3) those with ischaemic strokes (n = 30; twice in 1 patient). The patients with VTE had been diagnosed with unprovoked occlusions in the following sites: above knee (n = 29), inferior vena cava (n = 2), central retinal vein (n = 3), cerebral sinuses (n = 3), pulmonary artery (n = 9; twice in 1 patient), pulmonary artery + femoral vein (n = 4), and portal vein (n = 2).
Demographics and Laboratory Parameters of All Participants.
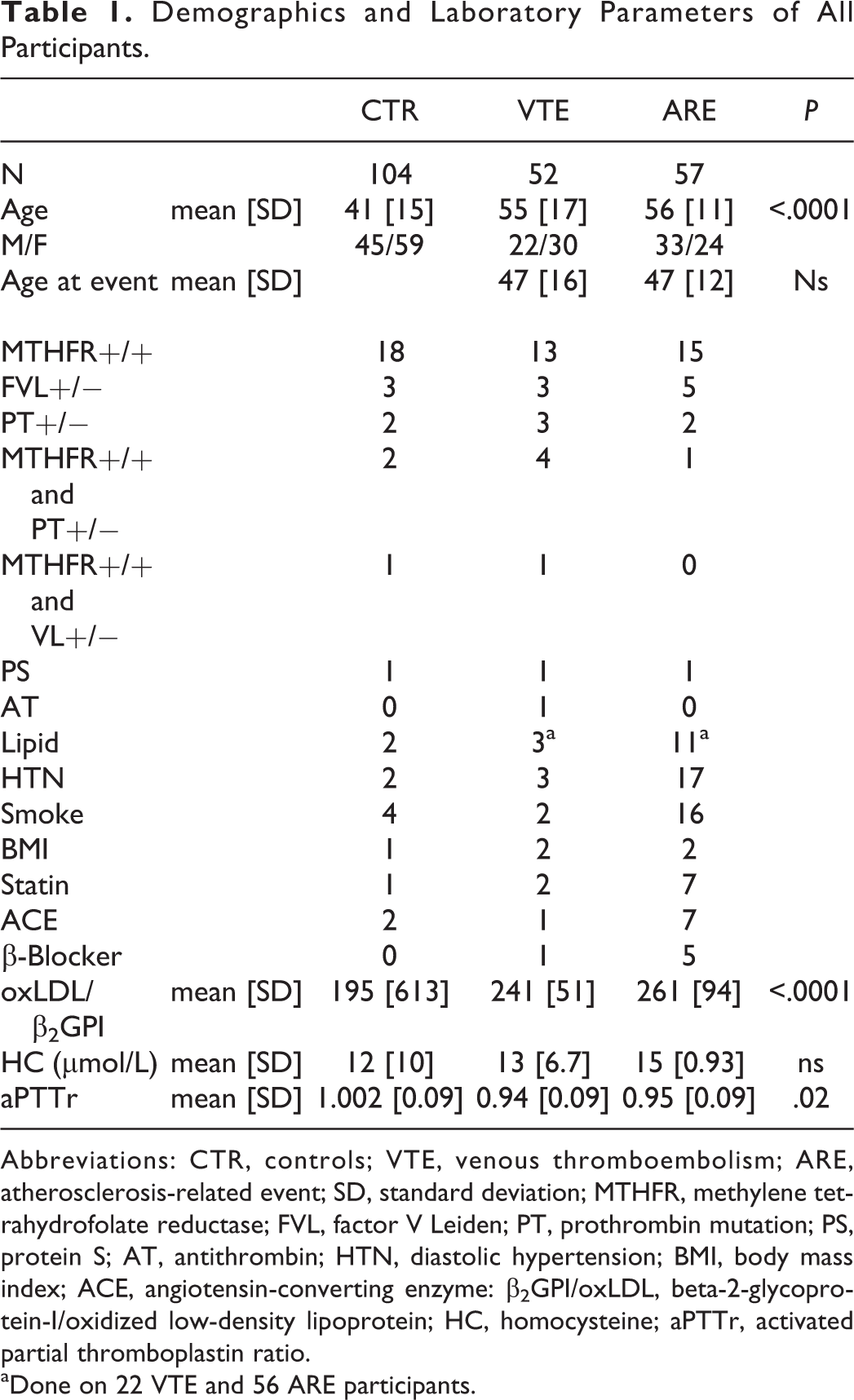
Abbreviations: CTR, controls; VTE, venous thromboembolism; ARE, atherosclerosis-related event; SD, standard deviation; MTHFR, methylene tetrahydrofolate reductase; FVL, factor V Leiden; PT, prothrombin mutation; PS, protein S; AT, antithrombin; HTN, diastolic hypertension; BMI, body mass index; ACE, angiotensin-converting enzyme: β2GPI/oxLDL, beta-2-glycoprotein-I/oxidized low-density lipoprotein; HC, homocysteine; aPTTr, activated partial thromboplastin ratio.
aDone on 22 VTE and 56 ARE participants.
The hospital and normal controls were merged in 1 group (Table 1). The hospital controls included 55 participants (M/F 22/33) diagnosed with the following conditions: 7 ovarian cysts, 9 headaches, 6 diastolic hypertension, 1 cataract, 2 Raynaud phenomenon, 1 patent foramen ovale, 2 lower limb edema, 9 early miscarriages, 1 bowel fistula, 3 hirsutism, 1 mitral valve prolapse, 3 menorrhagia, 1 eczema, 1 sternal trauma, 1 left ventricular dysfunction, 1 hypoxic gliosis, 2 peripheral neuropathy, 1 epilepsy, 1 colonic polyps, 1 goitre, and 1 upper limb paresthesias. The normal controls included 49 participants (M/F 23/26) seen for the following reasons: 2 liver donors, 1 kidney donor, and 46 for a thrombophilia screen: 7 before starting oral contraception and 39 were first-degree family members of a proband with thrombosis and inherited thrombophilia.
oxLDL/β2GPI, HC, and aPTT Across Groups
Plasma concentrations of oxLDL/β2GPI were progressively higher from controls, through patients with VTE to patients with ARE (P < .0001), HC showed a similar but nonsignificant trend, whereas aPTTr was lower in the VTE group (P = .02; Table 1).
oxLDL/β2GPI, ARE, and VTE
The oxLDL/β2GPI levels were divided into 4 quartiles: quartile 1, 20 to 175.6 U/mL; quartile 2, 175.7 to 227.8 U/mL; quartile 3, 227.9 to 251.6 U/mL; and quartile 4, 251.7 to 482.2 U/mL. The odds of having any vascular event was greater in the fourth and second quartiles than in the first quartile (9.9 and 4.1, respectively; Figure 1A); this is a reflection of the greater odds of having ARE in the fourth and second quartiles than in the first quartile (8.5 and 6.0, respectively; Figure 1C); among the ARE phenotypes, the odds of having MI was maximal in the fourth quartile (17.8; Figure 1C). The odds of having VTE was greater in the fourth quartile with a gradual reduction to the second quartile (11.4; Figure 1B).
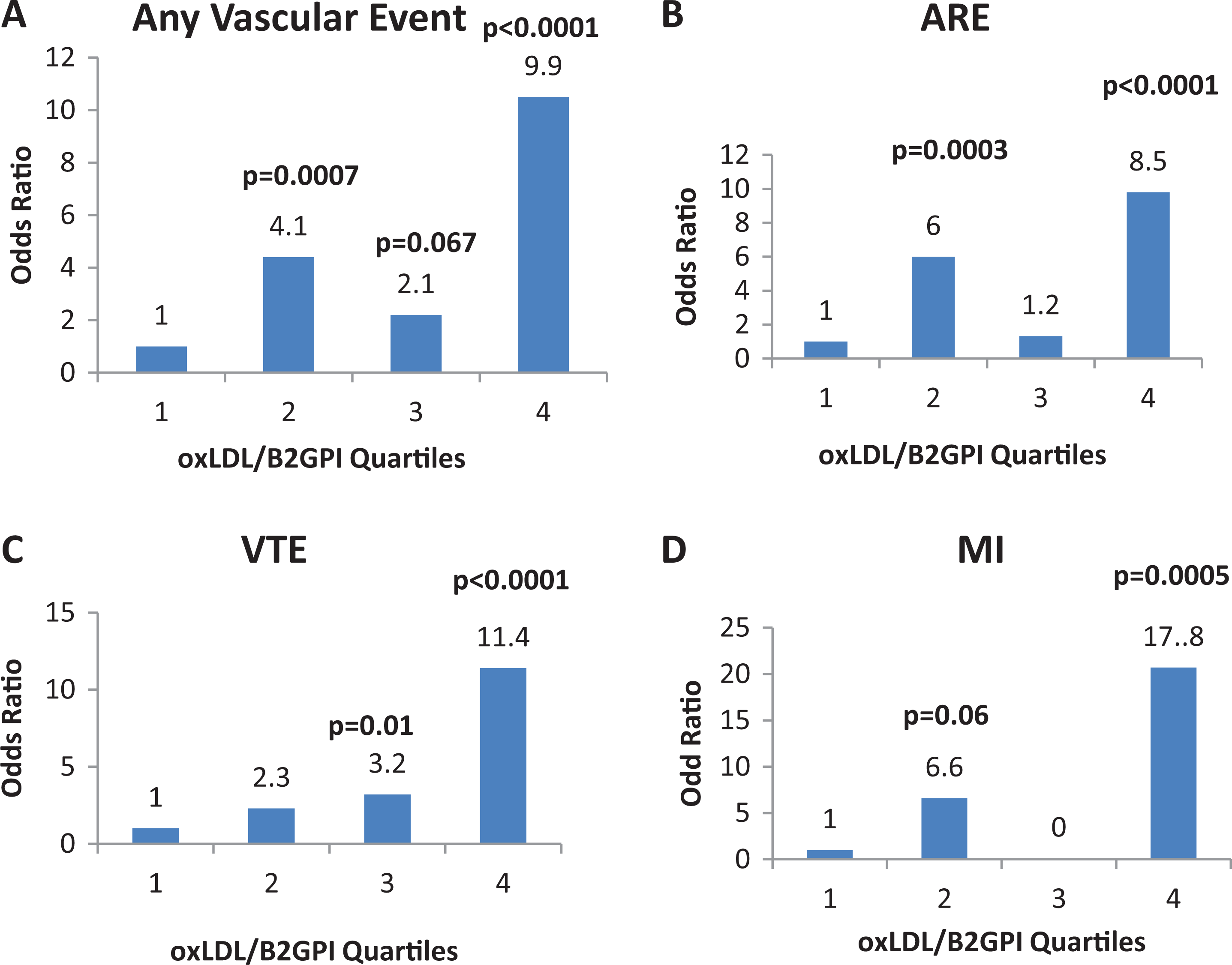
Odds ratio (OR) of any vascular event (A), atherosclerosis-related events (ARE) (B), spontaneous venous thromboembolism (VTE) (C), and myocardial infarction (MI) (D) by oxLDL/β2GPI quartiles. oxLDL/β2GPI indicates oxidized low-density lipoprotein/beta-2-glycoprotein-I.
Predictors of oxLDL/β2GPI in the ARE Group
By univariate analysis, oxLDL/β2GPI correlated to lipids status (r = 0.25, P = .056), subgroup (r = 0.62, P < .0001), and aPTTr (r = −0.32, P = .02); by multivariable analysis with age, sex, lipid status, and subgroup as independent variables and oxLDL/β2GPI as the dependent variable, only the MI subgroup independently predicted oxLDL/β2GPI (Table 2).
Predictors of β2GPI/oxLDL in Atherosclerosis-Related Event Group.
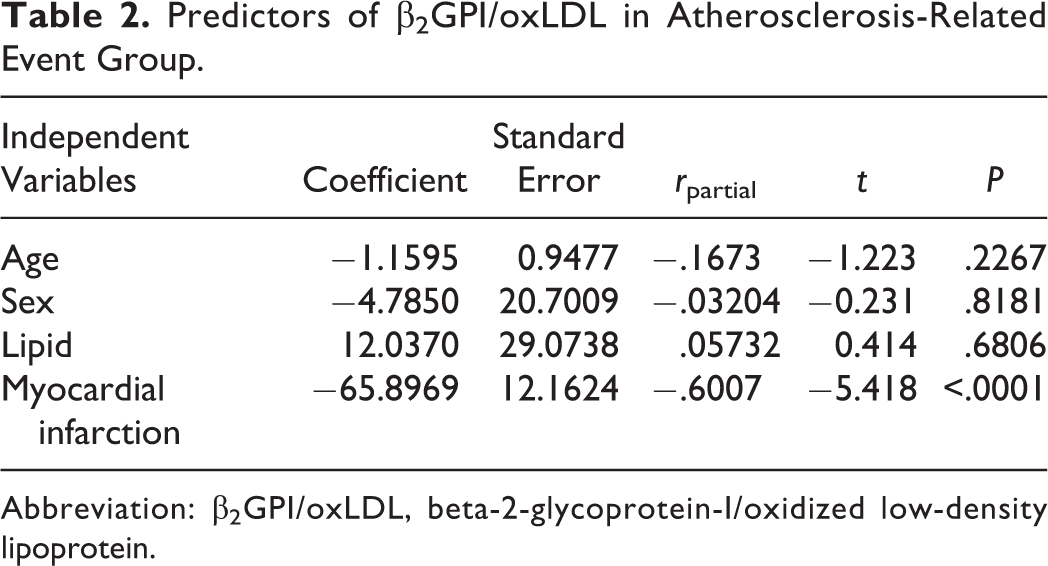
Abbreviation: β2GPI/oxLDL, beta-2-glycoprotein-I/oxidized low-density lipoprotein.
Predictors of aPTTr in the ARE Group
By univariate analysis, aPTT correlated negatively to age (r = −.27, P = .054) and to oxLDL/β2GPI (r = −.32, P = .02); by multivariable analysis, age, sex, oxLDL/β2GPI, and lipid status entered a multivariable regression model as independent variables and aPTTr as the dependent variable: Only age and oxLDL/β2GPI independently predicted aPTTr (Table 3). No relationship was found between oxLDL/β2GPI and any variable in patients with VTE.
Predictors of aPTTr in Atherosclerosis-Related Event Group.
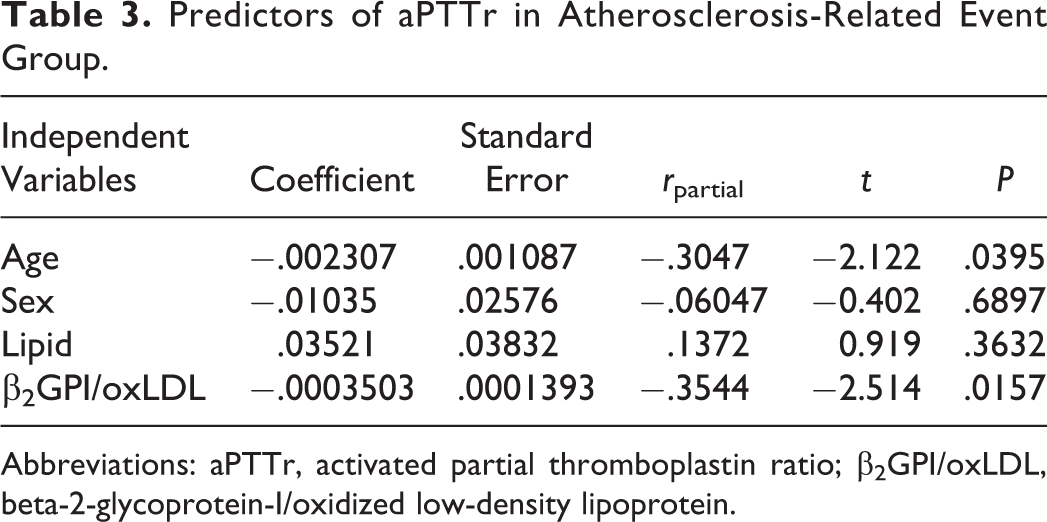
Abbreviations: aPTTr, activated partial thromboplastin ratio; β2GPI/oxLDL, beta-2-glycoprotein-I/oxidized low-density lipoprotein.
Discussion
Our study shows that the mean plasma concentration of oxLDL/β2GPI complexes is elevated in ARE and VTE. Patients in the upper quartiles were equally likely to suffer ARE or VTE: However, when the data were analyzed according to ARE subtype, patients in the upper quartile were much more likely to have suffered MI than other arterial phenotypes, though different MI severity may account for the bimodal significance of the quartiles; the multivariable regression confirmed MI as an independent predictor of oxLDL/β2GPI complexes. Given the relationship between plasma HC and oxidative stress, 10 we sought a possible relation between plasma HC and oxLDL/β2GPI: In the ARE group, neither HC nor hypertension, nor smoking, nor statin use was associated with oxLDL/β2GPI complexes though lipid status did, but only in univariable analysis. Likely the predictive effect of MI toward oxLDL/β2GPI may be explained by the vascular inflammation 12 that predisposes to oxLDL/β2GPI complex formation. 13
Notably, in the ARE group, we found that oxLDL/β2GPI negatively predicted the aPTTr: Oxidative modifications of LDLs have been associated either with a lower aPTTr 14 or with a higher aPTTr, 15 but this is the first time such an association is found with the oxLDL/β2GPI complex; β2GPI binds to oxLDL in the attempt to quench LDL oxidation, and oxidation of certain lipoprotein phospholipids supports thrombin generation, 16 hence β2GPI quenching should limit thrombin generation and coagulation activation and be more in keeping with a greater aPTTr 15 ; on the other hand, even oxLDL/β2GPI complexes may have residual oxidative capacity as indicated by C-reactive protein binding to oxLDL/β2GPI in an attempt to further quench its oxidative potential. 17 Alternatively or additionally, the relation between oxLDL/β2GPI and a lower aPTTr may be explained by increased plasma level of clotting factors as part of the vascular inflammation accompanying MI. 18
With regard to VTE, this is the first report of a graded OR between oxLDL/β2GPI quartiles and VTE; moreover, a closer overview of our data shows that the ORs for VTE and ARE (excluding MI) are quite similar, lending support to the idea that arterial and venous disease might share common pathogenic pathways among which oxidative and inflammatory mechanisms. According to a meta-analysis including 21 studies and 63 552 patients, cardiovascular risk factors associate with VTE 19 ; moreover, residual VTE is associated with a higher prevalence of subclinical atherosclerosis, 20 indicating a bidirectional relationship into which oxLDL/β2GPI complexes may well find its niche.
Limitations
We consider the following as limitations: (1) the cross-sectional nature of the study; (2) the lack of electrocardiographic screening in most control participants, as we cannot exclude that some of them might have subclinical ischemic heart disease though this would blunt rather than accentuate differences between groups; (3) the lack of lipid profiles in a proportion of patients, mostly in the VTE group, as participants attended a hamostasis unit and we did not test them; and (4) the lack of inflammatory markers or other clotting factors behaving as acute-phase reactants that would have allowed further insight into the relationship between oxLDL/β2GPI and aPTTr of the ARE group.
Conclusions
The oxLDL/β2GPI may represent a marker for MI, whereas the graded association with VTE should be further explored taking into account the extension of the venous occlusions 8 and we describe for the first time a link between oxLDL/β2GPI complexes and a low aPTTr. The bidirectional relationship oxLDL/β2GPI with ARE and VTE suggests that the link between arterial and venous disease may rely on similar oxidative/inflammatory and eventually coagulation pathways that require more elucidation on the venous side.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr L. R. Lopez is chief medical officer of Corgenix.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: oxLDL/β2GPI kits were a kind gift from Corgenix.