
Abstract
Women with polycystic ovary syndrome (PCOS) have coagulation disturbances and inflammation, which increases the risk of atherothrombosis. We evaluated the status of circulating tissue factor (TF), the receptor for coagulation factor VII involved in atherothrombosis, in women with PCOS and weight-matched controls. Two-way analysis of variance models were fit to evaluate the effect of PCOS status and weight class on TF and other parameters. The TF levels were significantly higher in lean women with PCOS compared to lean controls. Plasminogen activator inhibitor 1 (PAI-1) levels were significantly higher in obese participants compared to lean participants after controlling for PCOS status. The TF levels directly correlated with percentage of truncal fat and plasma levels of PAI-1, testosterone, androstendione, and dehydroepiandrosterone-sulfate; and inversely correlated with insulin sensitivity index–OGTT(ISOGTT). Circulating TF is elevated in PCOS independent of obesity, but both PCOS and obesity contribute to a prothrombotic state. In PCOS, abdominal adiposity and hyperandrogenism may exacerbate the risk of atherothrombosis.
Introduction
The polycystic ovary syndrome (PCOS) is one of the most common female endocrinopathies affecting between 8% and 12% of reproductive age women. 1 The disorder is characterized by hyperandrogenism, chronic oligo- or anovulation, and polycystic ovaries, with 2 out of these 3 findings required to diagnose PCOS. 2 As many as 70% of women with PCOS exhibit insulin resistance, with the compensatory hyperinsulinemia considered to be a promoter of hyperandrogenism in the disorder.3,4 Insulin resistance is also associated with accelerated atherothrombosis. 5 Indeed, women with PCOS have increased fibrinolytic activity and a higher prevalence of coronary artery calcification reflecting a predisposition to atherothrombosis.6,7 Women with PCOS are often afflicted by obesity, which is another risk factor for developing atherothrombosis. 8
Tissue factor (TF) is the receptor for coagulation factor VII and the principal initiator of blood coagulation. Tissue factor induces thrombin generation to promote fibrin formation and platelet activation. Tissue factor is produced by foamy macrophages and activated vascular smooth muscle cells within atherosclerotic plaque.9,10 Spontaneous plaque rupture exposes TF to the circulating blood. This, in turn, triggers thrombosis and culminates in blood vessel occlusion. Plasminogen activator inhibitor type l (PAI-1) is a potent serine protease inhibitor that complements TF action. The PAI-1 inhibits plasmin formation during plasminogen activation and fibrinolysis, thereby retarding thrombolysis. 11 The PAI-1 is also produced by smooth muscle cells along with endothelial cells, platelets, and hepatocytes. 12 However, the majority of circulating PAI-1 originates from adipose tissue and, not surprisingly, is increased in obesity.13,14 Inflammatory stimuli such as tumor necrosis factor-α (TNF-α) and oxidized low-density lipoprotein (ox-LDL) are abundant in adipose tissue. TNF-a and ox-LDL are both capable of stimulating the production of TF and PAI-1 following postprandial hyperglycemia.15–17 Thus, inflammation triggered by diet promotes a prothrombotic state.
Elevated circulating PAI-1 levels have been reported in PCOS.18,19 However, it remains unclear whether these elevations are due to PCOS per se, or merely a function of obesity.20–22 We embarked on a pilot study to determine the status of circulating TF levels in women with PCOS compared to weight-matched controls. We also examined the relationship of TF with body composition, insulin sensitivity, and circulating levels of PAI-1 and androgens. We hypothesized that circulating TF is increased in PCOS and that TF is related to measures of adiposity, insulin sensitivity, PAI-1, and androgens.
Materials and Methods
Participants
Twelve women with PCOS (6 lean and 6 obese) and 12 weight-matched ovulatory women serving as controls (6 lean and 6 obese) volunteered to participate in the study. The women with PCOS were diagnosed on the basis of oligoamenorrhea and hyperandrogenemia after excluding nonclassic congenital adrenal hyperplasia, Cushing syndrome, hyperprolactinemia, and thyroid disease. Polycystic ovaries were present on ultrasound in all participants with PCOS. Evidence of ovulation in control participants was based on having regular menses and a luteal phase serum progesterone level greater than 5 ng/mL. All control participants exhibited normal circulating androgen levels and the absence of polycystic ovaries on ultrasound. All of the participants provided written informed consent in accordance with Institutional Review Board guidelines for the protection of human participants.
Study Design
All study participants underwent an oral glucose tolerance test (OGTT) between days 5 and 8 following the onset of menses and an overnight fast of <12 hours. The women were provided with a healthy diet consisting of 50% carbohydrate, 35% fat, and 15% protein for 3 consecutive days before the test. All participants also underwent body composition assessment on the same day the OGTT was performed.
Oral Glucose Tolerance Test
All participants ingested a 75-g glucose beverage. Blood samples were drawn while fasting and 2 hours after ingestion of the glucose beverage to measure glucose and insulin. Plasma glucose concentrations were assayed immediately, and insulin measurements were performed later from plasma stored at −80°C. Additional plasma was isolated from the fasting blood samples and stored at −80°C until assayed for TF, PAI-1, and lipids. Insulin sensitivity 23 was derived by ISOGTT using the following formula: 10 000 divided by the square root of (fasting glucose × fasting insulin) × (mean glucose × mean insulin).
Body Composition Assessment
Height without shoes was measured to the nearest 1.0 cm. Body weight was measured to the nearest 0.1 kg. Waist circumference was measured at the level of the umbilicus and used to estimate abdominal adiposity. 24 In addition, all participants underwent dual energy absorptiometry (DEXA) to determine the percenatge total body fat and percentage truncal fat using the QDR 4500 Elite model scanner (Hologic Inc, Waltham, Massachusetts) as previously described.25,26
Plasma Measurements
Plasma glucose concentrations were measured by the glucose oxidase method (YSI, Yellow Springs, Ohio), while plasma insulin concentrations were measured by a double antibody RIA (Linco Research, St Charles, Missouri). Luteinizing hormone (LH), testosterone, androstenedione, and dehydroepiandrosterone-sulfate (DHEA-S) levels were measured by RIA (Diagnostic Products Corporation, Los Angeles, California). Enzyme-linked immunosorbent assay (ELISA) was used to measure plasma concentrations of TF (American Diagnostica Inc, Greenwich, Connecticut) and PAI-1 (R&D Systems, Minneapolis, Minnesota). Levels of total cholesterol, triglyceride, and high-density lipoprotein (HDL) cholesterol were measured by enzymatic methods (SYNCHRON LX20 PRO automatic analyzer, Beckman Coulter, Inc, Fullerton, California). Low-density lipoprotein cholesterol was calculated using Friedewald’s formula. 27 All samples from each participant were measured in duplicate in the same assay at the end of the study. The interassay and intra-assay coefficients of variation for all assays were 7% and 12%, respectively.
Statistical Analysis
All values were initially examined graphically for departures from normality, and the natural logarithm transformation was applied as needed. A subsequent 2-way analysis of variance (ANOVA) model was fit to evaluate the effect of PCOS status (PCOS vs control) and weight class (obese vs lean) on each variable. The results of the main effect tests are reported because none of the study variables exhibited a statistically significant interaction effect between PCOS status and weight class. The correlation analyses were performed by Pearson linear regression using the method of least squares. All values are expressed as mean ± standard error (SE). All calculated P values are 2-sided, and an α-level of .05 was used to determine statistical significance.
Results
Age, Body Composition, Blood Pressure, and Lipids
Age was similar among groups regardless of PCOS status or weight class. As expected, body mass index, percentage of total body fat, percentage of truncal fat, and waist circumference were significantly (P < .03) greater in obese participants compared to lean participants (Table 1 ). Systolic blood pressure, diastolic blood pressure, and triglyceride levels were also significantly (P < .04) higher in obese participants compared to the lean participants after controlling for the effect of PCOS status. There were no significant differences in these parameters between the women with PCOS and control participants after controlling for the effect of weight class.
Age, Body Composition, Blood Pressure, Endocrine, and Metabolic Parameters of Participantsa,b
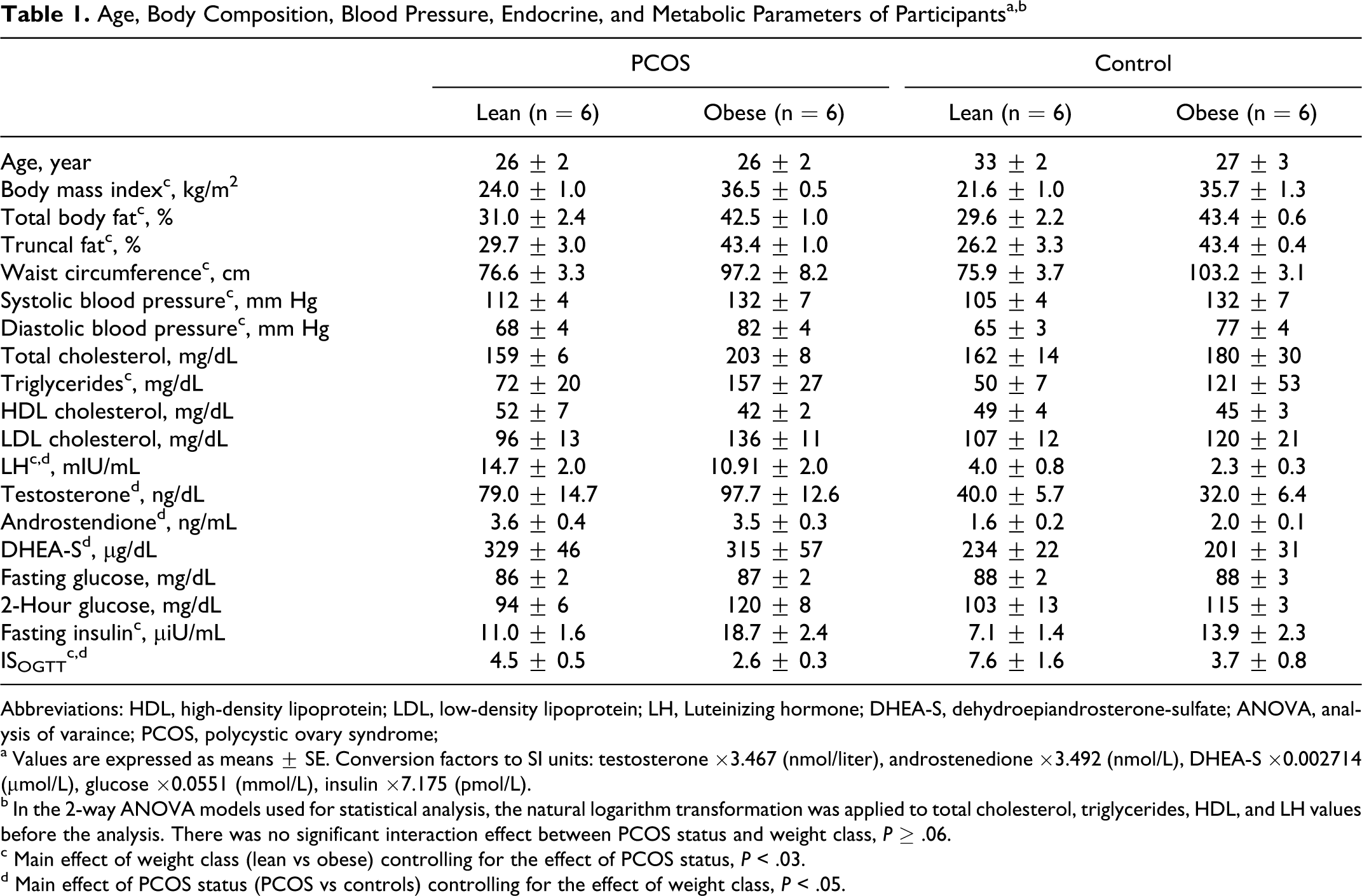
Abbreviations: HDL, high-density lipoprotein; LDL, low-density lipoprotein; LH, Luteinizing hormone; DHEA-S, dehydroepiandrosterone-sulfate; ANOVA, analysis of varaince; PCOS, polycystic ovary syndrome;
a Values are expressed as means ± SE. Conversion factors to SI units: testosterone ×3.467 (nmol/liter), androstenedione ×3.492 (nmol/L), DHEA-S ×0.002714 (μmol/L), glucose ×0.0551 (mmol/L), insulin ×7.175 (pmol/L).
b In the 2-way ANOVA models used for statistical analysis, the natural logarithm transformation was applied to total cholesterol, triglycerides, HDL, and LH values before the analysis. There was no significant interaction effect between PCOS status and weight class, P ≥ .06.
c Main effect of weight class (lean vs obese) controlling for the effect of PCOS status, P < .03.
d Main effect of PCOS status (PCOS vs controls) controlling for the effect of weight class, P < .05.
Plasma Hormone Levels, Glycemic Status, and Insulin Sensitivity
Circulating levels of LH, testosterone, androstenedione, and DHEA-S were significantly (P < .05) elevated in women with PCOS compared to control participants regardless of weight class (Table 1). Glucose levels while fasting and 2 hours post glucose ingestion were similar among groups regardless of PCOS status or weight class. Fasting insulin levels were significantly (P < .03) higher in obese participants compared to lean participants, regardless of PCOS status. ISOGTT was significantly (P < .03) lower in obese individuals compared to lean individuals and significantly (P < .05) lower in women with PCOS compared to the control participants.
Plasma TF and PAI-1 Levels
Plasma TF concentrations were significantly (P < .02) higher in women with PCOS compared to control participants after controlling for weight class (Figure 1 A). The concentrations of TF and PAI-1 were both significantly (P < .0004) higher in obese individuals compared to lean individuals after controlling for PCOS status (Figure 1A and B).
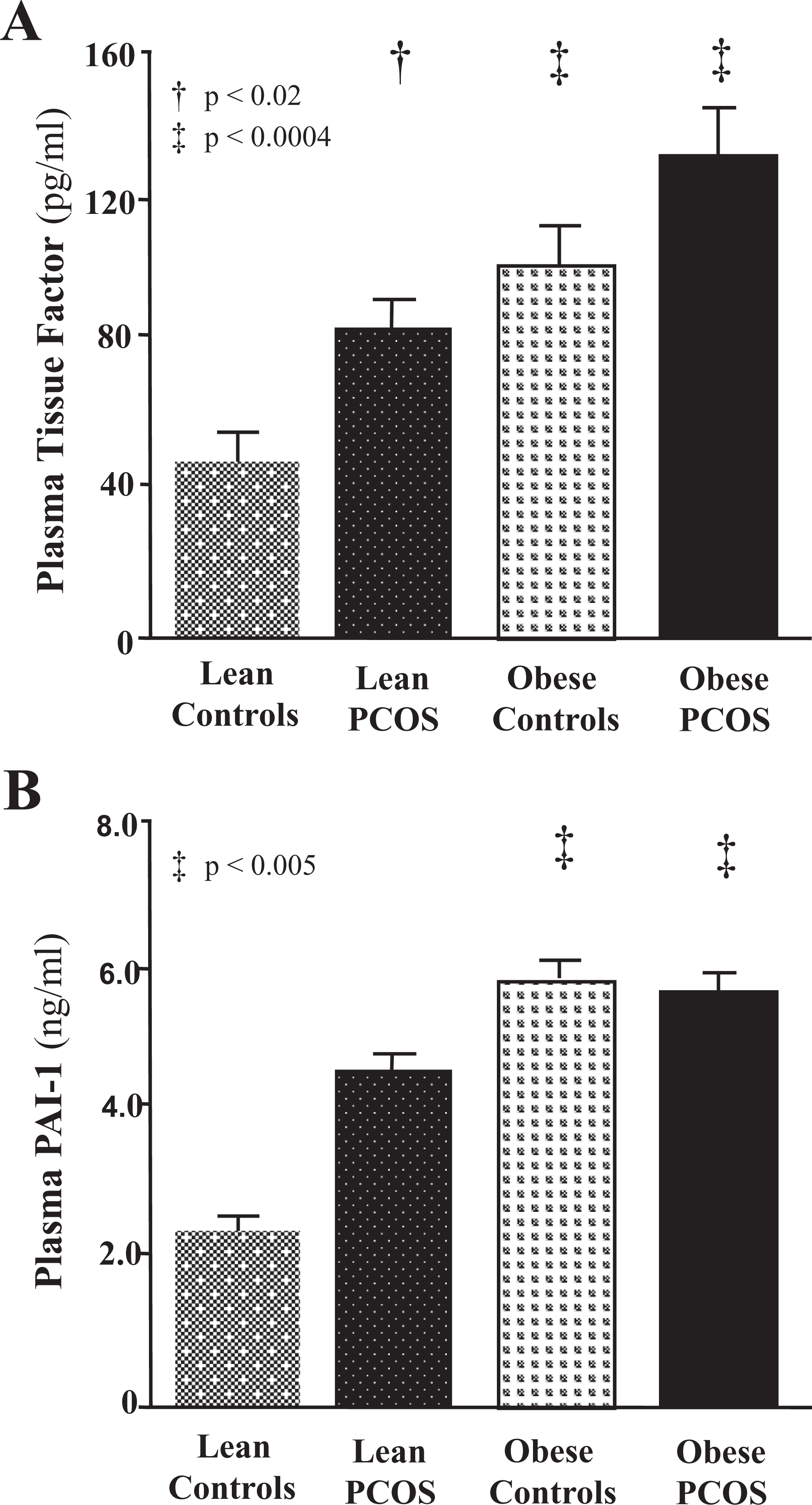
A, Plasma tissue factor (TF) measured in fasting blood samples. In a 2-way ANOVA model, there was no significant interaction effect between PCOS status and weight class, P = .83. †Main effect of PCOS status (PCOS vs controls) controlling for the effect of weight class, P < .02. ‡Main effect of weight class (lean vs obese) controlling for the effect of PCOS status, P < .0004. B, Plasma plasminogen activator inhibitor 1 (PAI-1) measured in fasting blood samples. In a 2-way ANOVA model, there was no significant interaction effect between PCOS status and weight class, P = .06. The natural logarithm transformation was applied to PAI-1 values before the analysis. †Main effect of PCOS status (PCOS vs controls) controlling for the effect of weight class, P = .07. ‡Main effect of weight class (lean vs obese) controlling for the effect of PCOS status, P < .005. PCOS indicates polycystic ovary syndrome; ANOVA, analysis of variance; PAI-1, plasminogen activator inhibitor 1.
Correlations
There was a positive correlation between plasma levels of TF and PAI-1 (r = .42, P < .05) for the combined groups. Each of these levels were directly correlated with BMI (TF: r = .63, P < .002; PAI-1: r = .55, P < .009), percentage of body fat (TF: r = .52, P < .01; PAI-1: r = .45, P < .04), percentage of truncal fat (TF: r = .54, P < .007; PAI-1: r = .46, P < .04), and fasting insulin (TF: r = .49, P < .02; PAI-1: r = .47, P < .03). Plasma TF was also positively correlated with waist circumference (r = .69, P < .0004), and plasma levels of testosterone (r = .41, P < .05), androstendione (r = .42, P < .05), and DHEA-S (r = .51, P < .02). ISOGTT was negatively correlated with TF (r = −.40, P < .05; Figure 2 A-C). There were no correlations between plasma PAI-1 and androgens or ISOGTT.
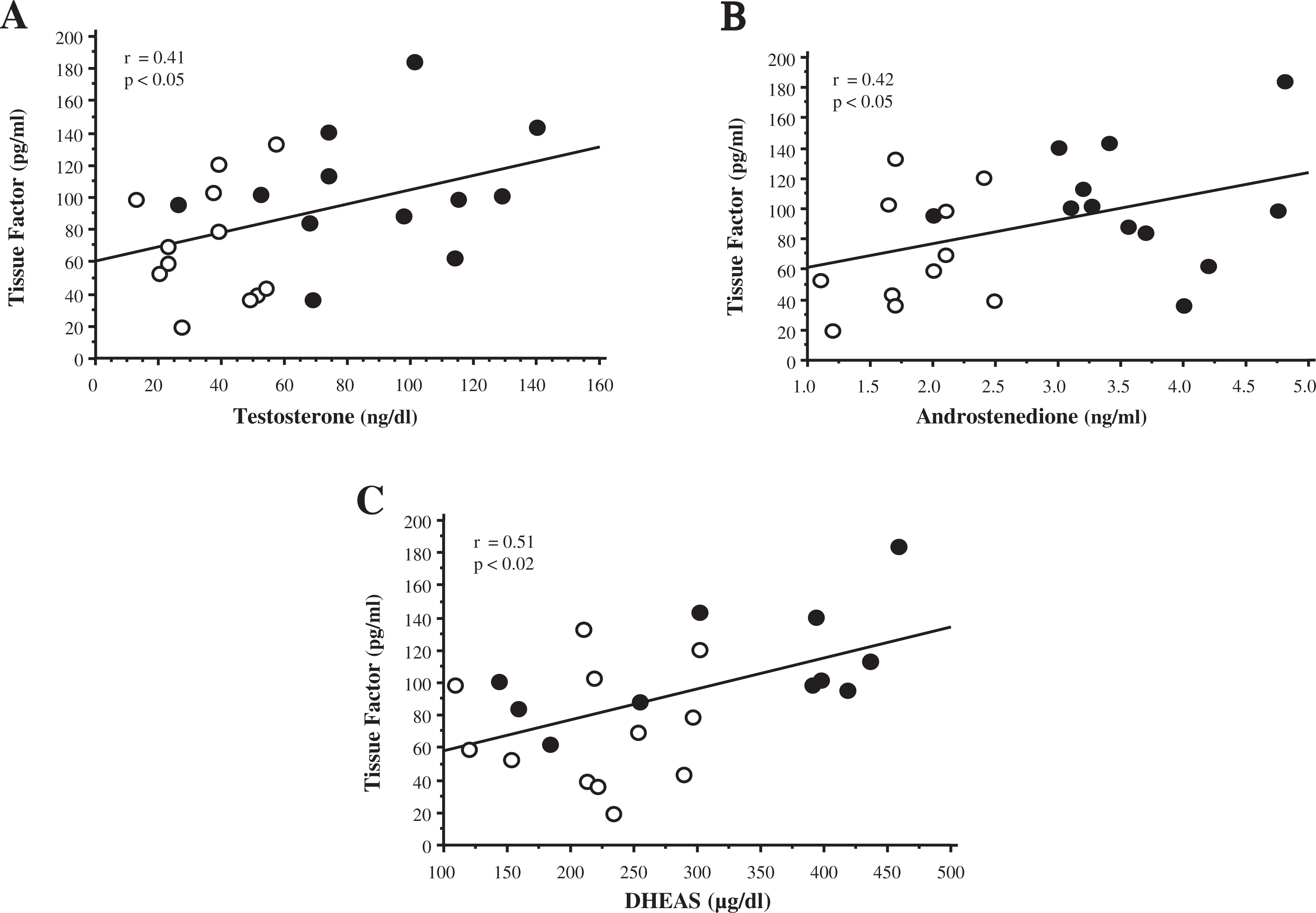
Correlations between plasma tissue factor levels and plasma levels of (A) testosterone, (B) androstenedione, and (C) DHEA-S. O, Control participants; •, women with PCOS. PCOS indicates polycystic ovary syndrome; DHEA-S, dehydroepiandrosterone-sulfate.
Discussion
Our data clearly show for the first time that circulating TF levels are elevated in PCOS; and that these elevations are independent of obesity. This is evident by the elevated TF levels in lean women with PCOS compared to weight-matched controls. In addition, systolic and diastolic blood pressures and triglycerides along with TF levels are increased in the obese whether or not they have PCOS. Insulin sensitivity is lower in women with PCOS compared to weight-matched controls, and the lowest insulin sensitivity evident in obese women with PCOS. Collectively, these findings support the concept that both PCOS and obesity contribute to a prothrombotic state, elevated blood pressure, and insulin resistance, which in turn underlie the development of atherothrombosis. Tissue factor is directly related to androgen levels suggesting that atherothrombotic activity may be promoted by hyperandrogenism in PCOS. Furthermore, the independent associations of TF and PAI-1 with abdominal adiposity suggest that the accumulation of abdominal fat is an important contributing factor in promoting atherothrombosis and subsequent cardiovascular events in obese women with PCOS.
In contrast to plasma TF, the elevation in plasma PAI-1 appears to be more a function of obesity than PCOS per se. Moreover, PAI-1 in the current study is elevated in obese participants compared to those who are lean regardless of the PCOS status. This latter finding is consistent with previous reports.20,21 Elevations in TF and PAI-1 may work in consort in PCOS to promote a prothrombotic state; and when combined with accelerated atherogenesis as described in our previous reports, increases the risk of cardiovascular events.28,29 This concept is further supported by the direct relationship between TF and PAI-1. Nevertheless, the elevated TF levels in lean women with PCOS compared to lean controls suggest that accelerated atherothrombosis in PCOS is independent of obesity. The insulin resistance evident in women with PCOS based on a lower ISOGTT is a feature highly associated with atherothrombosis. 5 This is confirmed in the present study by the inverse relationship between ISOGTT and plasma levels of TF. Thus, the presence of PCOS in combination with obesity may result in greater risk of atherothrombosis compared to having PCOS or obesity alone.
In PCOS, there may be a link between adiposity and circulating TF levels. While not evident in the present study, our group and other investigators have previously shown that aside from obese women with PCOS, abdominal adiposity can be increased in lean women with the disorder.30–32 Moreover, plasma TF is directly related to measures of adiposity, particularly abdominal adiposity. The same is true for plasma PAI-1 and is corroborated by our previous report. 29 Circulating mononuclear cells are known to migrate into adipose tissue to stimulate adipocyte production of TNF-α which, in turn, promotes increases in TF and PAI-1.15,33 Inflamed adipose tissue, especially in the abdominal region, may be a perpetuator of elevated circulating TF levels in obese women with PCOS. Thus, these data are striking because they suggest that adiposity-related inflammation may initiate a prothrombotic milieu in women with PCOS at an early age.
In PCOS, hyperandrogenism may be capable of promoting atherothrombosis. This is suggested by the direct relationship between TF and plasma levels of testosterone, androstenedione, and DHEA-S. Androgen exposure increases adhesion of mononuclear cells to vascular endothelium and oxidation of LDL by mononuclear cell-derived macrophages.34,35 Furthermore, androgens at physiologic concentrations enhance platelet aggregation and vascular reactivity.36,37 These androgen-related phenomena favor the production of TF and subsequent thrombin generation by TF during atherothrombosis. We have previously shown that in PCOS, hyperglycemia increases reactive oxygen species (ROS) generation, nuclear factor κB (NFκB) activation, and TNF-α release from mononuclear cells; and that similar to TF, these pro-oxidant, proinflammatory mediators are highly correlated with circulating androgens.25,38,39 Thus, hyperandrogenism in PCOS may be responsible for inducing the inflammation-related TF production that contributes to atherothrombosis.
In conclusion, circulating TF levels are elevated in PCOS independent of obesity. This prothrombotic phenomenon may place women with PCOS at an increased risk of developing atherothrombosis. Tissue factor is also associated with abdominal fat and circulating androgens. This suggests that increased abdominal adiposity and hyperandrogenism can contribute significantly to the promotion of atherothrombosis in PCOS.
Footnotes
Authors’ Note
This study was presented at the 64th Annual Meeting of the American Society for Reproductive Medicine, San Francisco, California, November 8-12, 2008.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed the receipt of following financial support for the research, authorship, and/or publication of this article: This work was supported by National Institutes of Health Grant HD-048535 to F.G.