
Abstract
Aim:
The aim of the present study was to investigate the predictive value of preoperative neutrophil–lymphocyte ratio (NLR) in postoperative saphenous vein graft patency in patients undergoing coronary artery bypass grafting (CABG) surgery.
Method:
We retrospectively analyzed 444 patients who had undergone CABG and a further control coronary angiography due to recurrence of symptoms. The patients were divided into tertile groups according to the NLR. The primary end point was 50% saphenous vein graft stenosis or more or complete occlusion.
Result:
The saphenous vein graft failure in the 3 groups based on NLR was 33%, 66.2%, and 79.1%, in the low-, middle- and high-risk groups, respectively. In multivariate regression modeling, current smoker, diabetes mellitus, target artery diameter <1.5 mm, and NLR independently predicted saphenous vein graft patency in patients after CABG. Conclusion: Preoperative NLR is clearly an independent predictor of saphenous vein graft patency in patients after CABG.
Introduction
Coronary artery bypass grafting (CABG) is an effective therapy for the treatment of advanced coronary artery disease. However, the long-term results are compromised after CABG by the development of saphenous vein graft failure (SVGF). 1 One month after bypass surgery, the vein graft failure was due to thrombotic occlusion; but the vein graft failure at a later stage was due to atherosclerotic obstruction occurring in a foundation of neointimal hyperplasia. 2
Atherosclerosis plays an important role not only in initiation and progression of coronary artery disease but also in the development of saphenous graft stenosis. 1,2 The role of low-grade inflammation in the pathogenesis of atherosclerosis and its acute complications are well determined, and several biological markers of inflammation predict cardiovascular risk. 3,4 Neutrophil to lymphocyte ratio (NLR), a recently described novel risk marker, has been shown to be predictive of mortality in following percutaneous coronary intervention and CABG. 3 –5
The NLR has been used in in-stent restenosis 6 and progression of coronary artery disease 7 to investigate the relationship between inflammatory response and progression of atherosclerosis; however, no study has investigated any possible association between NLR and SVGF after CABG. The aim of the present study was to evaluate the usefulness of NLR before successful CABG in predicting SVGF.
Materials and Methods
The study population included 458 patients who had undergone a primary coronary artery bypass surgery between January 2002 and January 2011 with at least 1 vein graft and who later had a recurrence of symptoms that necessitated a coronary angiogram.
Patients below 80 years of age undergoing nonemergent primary isolated coronary bypass surgery with graftable 2-vessel disease were eligible for the study. In addition, circumflex of the target coronary vessels and the right coronary arteries, which had lesions with ≥70% diameter narrowing, were deemed to be of acceptable quality, according to visual assessment of the preoperative angiogram by the operating surgeon were the inclusion criteria for the study.
Patients with active infectious disease (n = 3), clinical evidence of cancer (n = 2), unavailable complete blood cell count or medical records (n = 5), or chronic inflammatory disease (n = 4) were excluded from the outcome analysis. Fourteen patients were excluded according to these criteria. Thus, 444 patients were included in the study. The preoperative patient characteristics, laboratory data, operative, and postperative variables were recorded in the database (Table 1). The local ethics committee approved the study protocol.
Baseline Characteristics of Patients Grouped by Tertile of Neutrophil–Lymphocyte Ratio.
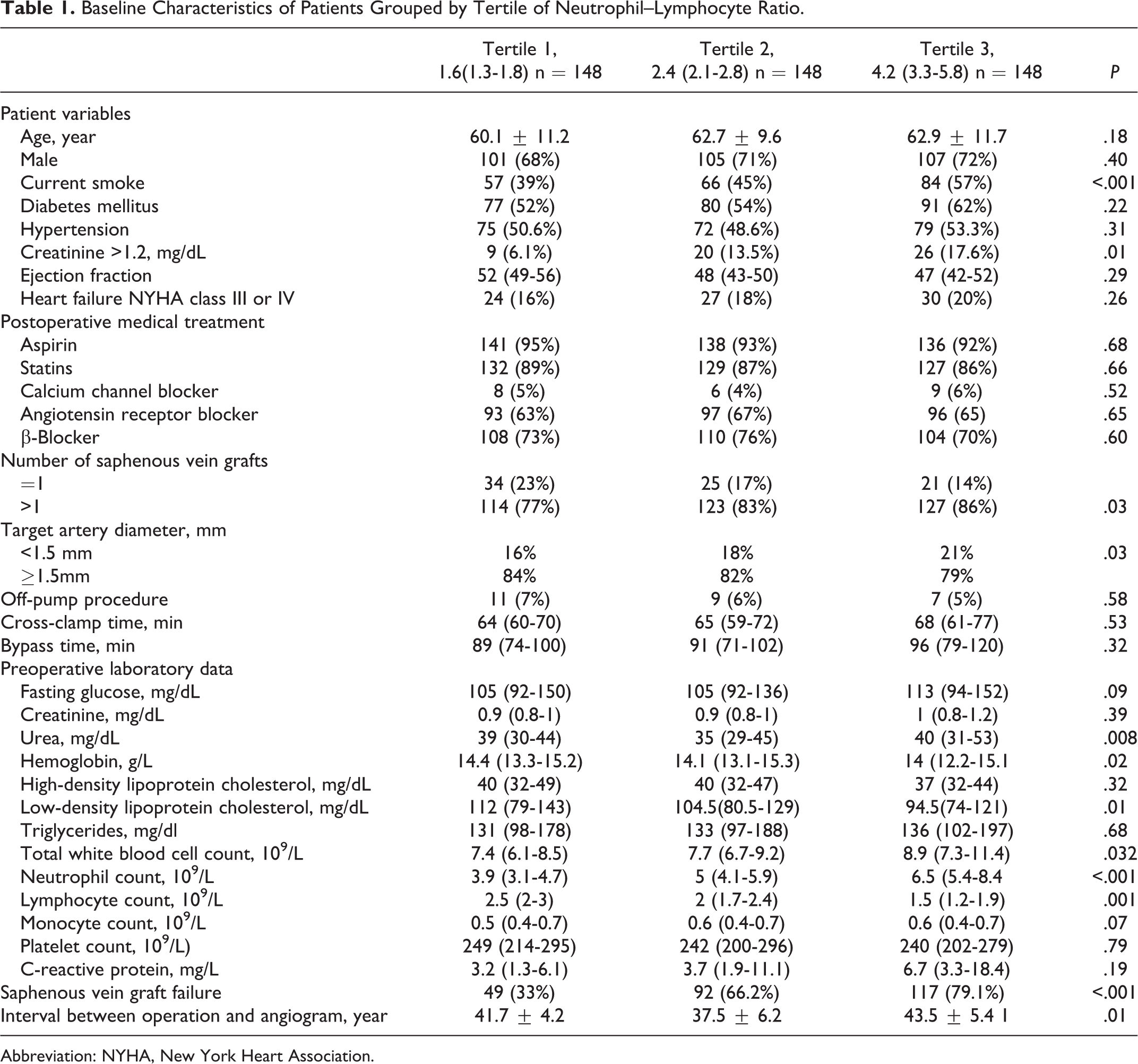
Abbreviation: NYHA, New York Heart Association.
All laboratory data were obtained from venous blood samples up to 1 day before the surgery. Total white blood cell (WBC), neutrophil, lymphocyte, and monocyte counts were calculated using an automated blood cell counter (ADVIA 2120i Hematology System, Siemens Healthcare Diagnostics, Deerfield, Illinois). The NLR was calculated as the preprocedural ratio of neutrophils to lymphocytes, which was obtained from the same blood samples. The C-reactive protein (CRP) levels were measured by an immunonephelometric method (Roche Diagnostics GmbH, Marburg, Germany).
During the operation, saphenous veins were harvested by a conventional open “no-touch” technique. Veins from the calf were generally preferred. Veins were dilated to their naturally distended state, and overdistention was avoided. An internal thoracic artery was used to bypass the left anterior descending artery territory. The SVG was used for the right coronary system and the region with circumflex. Additional grafts were constructed, if necessary, with single rather than sequential grafts. After the operation, atorvastatin and aspirin were routinely used.
Angiographic Analysis
During routine clinical follow-up after operation, coronary angiography was performed secondarily in patients with stable or unstable angina pectoris. Control coronary angiograms were recorded with Judkins technique and interpreted by 2 independent cardiologists and a surgeon who were blinded to the patients’ data. The method of reporting was uniform. All the grafts were described in detail, including the degree of stenosis and coronary grafting. Saphenous vein graft was considered to have failed if it had 50% stenosis or more or complete occlusion. Each angiogram was independently adjudicated in a blinded fashion by 2 committee members, with a third review in the case of disagreement in outcome.
Statistics
Analyses were performed using SPSS 15.0 statistical software (SPSS Inc, Chicago , IL). Continuous data were presented as median and interquartile range or mean ± standard deviation. To test the distribution pattern, the Kolmogorov-Smirnov test was used. The study population was assigned into tertiles based on NLRs at admission. Comparisons of multiple mean values were carried out by Kruskal-Wallis tests or analysis of variance, as appropriate. Categorical variables were summarized as percentages and compared with chi-square test. Spearman correlation coefficient was computed to examine the association between 2 continuous variables. Effects of different variables on SVGF were calculated in univariate analysis for each. Variables that had unadjusted P value <.10 in logistic regression analysis were identified as potential risk markers and included in the full model. We reduced the model using stepwise multivariate logistic regression analyses and eliminated potential risk markers using likelihood ratio tests. A P value <.05 was considered statistically significant, and the confidence interval was 95%.
Results
In total, 444 patients (mean age 61.9 ± 10.6 years, 313 [70.4%] male) were enrolled in the study (Table 1). Most patients had been diagnosed with diabetes mellitus (56%) or hypertension (51%) before surgery. Surgeons at one surgical center performed a mean of 3.1 ± 0.7 grafts (range, 2-6 grafts; total 1314 saphenous vein grafts, 55 radial artery grafts), with the majority of patients undergoing on-pump surgical procedures. The number of saphenous veins grafted to each of the target coronary arteries was as follows: the left anterior descending artery, 10 (0.7%); diagonal artery, 157 (11.9%); obtuse marginal artery, 368 (28%); posterior descending artery, 149 (11.3%); and right coronary artery, 199 (15.1%). The mean interval from operation to re-angiogram was 47 months (Table 1).
Postoperative Management
Discharge medications prescribed included aspirin in 93% patients, lipid-lowering medications in 87%, and beta-blockers in 73%. Patients were divided into 3 tertiles based on NLR: 1.69 (1.44-1.88) in tertile 1, 2.55 (2.30-2.79) in tertile 2, and 3.80 (3.25-5.03) in tertile 3. Each group was composed of 148 patients. Table 1 presents the baseline demographic and clinical data of patients by tertile of NLR. Patients in tertile 3 were more likely to have higher urea, hemoglobin, low-density lipoprotein cholesterol, total WBC, and CRP levels than those in tertiles 1 and 2. Also, creatinine >1.2, interval between operation and angiogram, current smoking, number of saphenous vein grafts >1, and target artery diameter <1.5 mm were higher in patients in tertile 3. A positive correlation was observed between NLR and CRP levels (r = .148, P =.04). Overall there were 258 SVGF, and patients with a high NLR showed the highest SVGF (79.1%) when compared to patients with medium (66.2%) and low NLR (33%), respectively (Table 1). Furthermore, comparison of SVGF in high NLR versus intermediate and low NLR was also statistically significant (Figure 1; P = .001, P <.001).
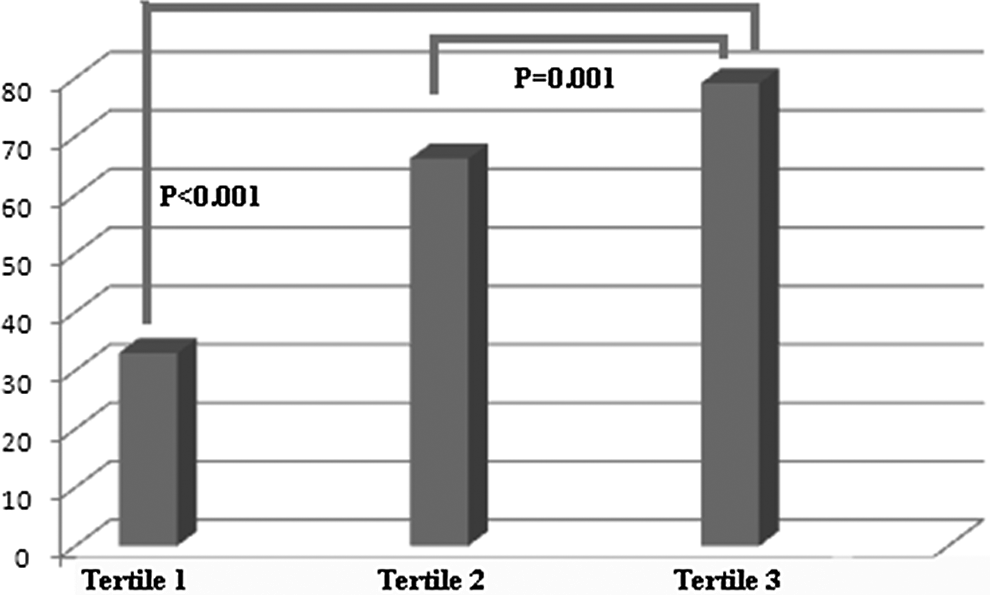
Percentage of patients developing saphenous vein graft failure stratified by tertile of preprocedural neutrophil to lymphocyte ratio.
In patients, SVGF was correlated with admission fasting glucose (r = .129, P = .007), total WBC count (r = .206, P < .001), neutrophil count (r = .108, P = .02), NLR (r = .211, P < .001), creatinine >1.2 (r = .098, P = .04), target artery diameter <1.5 mm (r = −.232, P < .001), current smoking (r = .105, P = .02), diabetes mellitus (r = .192, P < .001), and interval between operation and angiogram (r = .204, P < .001). There were no significant correlations between all-cause mortality and the other data (P > .05).
In univariate logistic regression analyses, creatinine >1.2, target artery diameter <1.5 mm, current smoking, diabetes mellitus, NLR, and interval between operation and angiogram were all significantly associated with SVGF. When these 6 variables were included in a multivariate regression modeling, current smoking, diabetes mellitus, target artery diameter <1.5 mm, and NLR remained as independent factors associated with SVGF (Table 2).
Significant Predictors of Saphenous Vein Graft Failure in Univariable and Multivariable Logistic Regression Analyses.
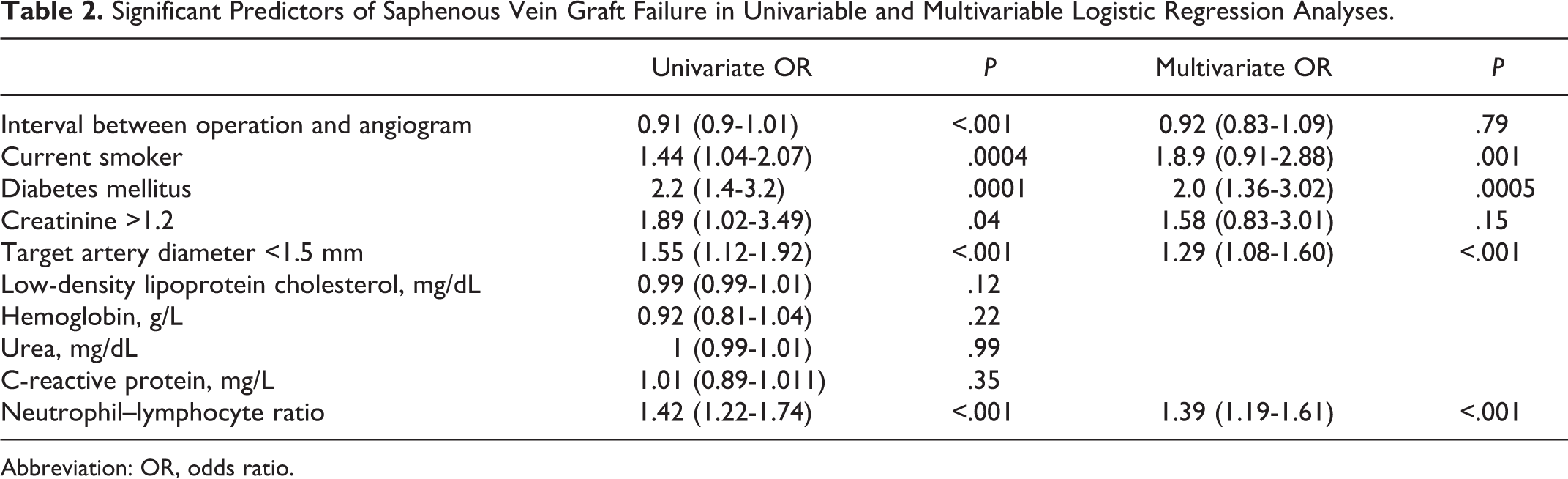
Abbreviation: OR, odds ratio.
Discussion
The findings of the present study demonstrate that a simple ratio (NLR) obtained from a universally available low-cost test provides relevant information regarding the risk of SVGF in patients who had underwent successful CABG before. We demonstrated that NLR is a powerful and independent predictor of further SVGF after CABG. Patients in the highest tertile of NLR were at greater risk.
In some series, up to 20% of saphenous vein grafts become occluded within the first year after CABG. 1,8 Historically, 10 years after surgery, only 60% of the SVGs remain patent and half of those that are patent have clinically important stenosis. 1,9,10 Patients who have previously undergone CABG are therefore at risk of subsequent ischemic events. 1,9,10 Although arterial conduits have gained attention in the recent years, saphenous vein remains the most commonly used conduit during CABG because of its ease of use and ready availability. 8,11
Saphenous vein graft disease is composed of 3 discrete processes: thrombosis, intimal hyperplasia, and atherosclerosis. Between 3% and 12% of saphenous vein grafts occlude, due to thrombotic occlusion, with or without symptoms, within the first month of bypass surgery. 10,12 Neointimal hyperplasia, whether in the balloon-injured coronary artery or in the grafted vein, follows a similar pathogenic mechanism. Nonetheless, neointimal hyperplasia could constitute a potent point for later development of graft atheroma. The extensive neointimal hyperplasia throughout the length of a vein graft may effectively create a diffuse atherosclerosis-prone region. 1
Beyond the first year after bypass surgery, atherosclerosis is the dominant process underlying the attrition of saphenous vein grafts. Necropsy studies have found evidence of atheromatous plaques as early as 1 year after the bypass surgery, but hemodynamically important vein graft atheroma increases markedly after 5 to 7 years. 2,8,13,14 The histological types and stages of atherosclerotic lesion development in native coronary arteries have been comprehensively reviewed by the AHA Council on Arteriosclerosis. 15 Although the fundamental process of atheroma development and the predisposing factors are similar in vein grafts, 1 atherosclerotic process may progress more rapidly in saphenous vein grafts. Saphenous vein graft atheroma has more foam cells and inflammatory cells than the native coronary atheroma in histologic studies. These results support the role of inflammatory process in the progression of saphenous vein atheroma. 1,2,8
In recent years, it has become clear that atherogenesis represents an active inflammatory process rather than simply a passive vascular injury with infiltration of lipids. Chronic low-grade inflammation in the arterial wall plays a crucial role in the initiation and progression of atherosclerosis. 16 –19 Experimental models provide compelling evidence for the role of inflammation in the initiation, progression, and complication of atherosclerosis confirmed in the clinical setting. 20
The association between systemic inflammation and arteriosclerosis has been reported in various studies conducted on different inflammatory markers. Of those, CRP was the most frequently studied biomarker, owing to its accurately reflecting systemic inflammation and it being a strong predictor of cardiovascular outcomes. 21,22 However, high levels of high-sensitivity CRP are correlated with angiographically proven coronary artery disease progression. 23,24 Other inflammatory biomarkers such as fibrinogen, interleukin 1, lipoprotein (a), and interleukin 6 may also provide additional information regarding the preprocedural inflammatory state and anticipation of coronary atherosclerosis. 25,26 A higher level of WBC count, even within normal range, has been associated with atherosclerotic cardiovascular events. 17,27 Stimulated WBCs have an increased tendency to adhere to vascular endothelium and easily penetrate the intima, causing capillary leukostasis and increased vascular resistance. 28 –30 Additionally, stimulated WBCs release a variety of hydrolytic enzymes, cytokines, and growth factors that can induce further vascular damage. 18,19 The WBCs are composed of 5 different types of immune cells. Leukocytes play a major role in this inflammatory process. For example, much of the predictive power of the total leukocyte count is contained in the neutrophil component. 17,31 Horne et al 32 reported that a high neutrophil count with a low WBC count accounts for cardiovascular diseases. In an animal study, neutrophil invasion to atherosclerotic plaque has been visualized directly in vivo. 33 Moreover, CAPRIE 34 and SOLVD 35 studies showed that increased neutrophil count and decreased lymphocyte count are associated with worse cardiovascular outcomes. Likewise, reduced lymphocyte counts in patients with CAD reflect a physiologic stress response to cortisol and are independently associated with worse prognosis. 36,37 The predictive value of these indices has been combined by calculating the NLR. This may be a more powerful predictor of cardiovascular risk than the total WBC or individual WBC subtypes. 5,32
Unlike many other inflammatory markers and bioassays, NLR is an inexpensive and readily available marker that provides an additional level of risk scores in predicting in-hospital and long-term outcomes. The NLR, a recently described novel risk marker, has been shown to be predictive of morbidity and mortality in a variety of cardiovascular settings, including acute myocardial infarction, 38 coronary artery disease, 7,17 heart failure, 39 and critical limb ischemia. 16 Moreover, multiple studies have suggested that NLR is a strong predictor of outcomes in percutaneous coronary intervention 5 and CABG. 3 Similarly, it is shown that progression of atherosclerosis in native coronary arteries, 7 bare-metal stent restenosis, 6 and graft patency following lower limb revascularization 40 had been associated with NLR in previous studies. In present study, we evaluated the NLR as a powerful and independent risk factor for saphenous vein graft stenosis after successful CABG surgery. According to our knowledge, this is the first study demonstrating the association between NLR and SVGF after CABG.
The limitations of the present study are as follows: (1) This study was conducted on a retrospective basis and represented a single-center experience. (2) Only 1 measurement of admission full blood count and calculation of NLR was included in the analysis, and it was not possible to determine whether an acute and brief inflammation was responsible for the correlation observed. (3) Definition of stenosis was based on visual inspections and not on quantitative measurements.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.