
Abstract
Postthrombotic syndrome (PTS) is a frequent complication of venous thromboembolism (VTE). Using MarketScan claims data from January 2012 to June 2015, we identified adults with a primary diagnosis code for VTE during a hospitalization/emergency department visit, ≥6 months of insurance coverage prior to the index event and newly started on rivaroxaban or warfarin within 30 days of the index VTE. Patients with <4-month follow-up postindex event or a claim for any anticoagulant during 6-month baseline period were excluded. Differences in baseline characteristics between rivaroxaban and warfarin users were adjusted for using inverse probability of treatment weights based on propensity scores. Patients were followed for the development of PTS starting 3 months after the index VTE. Cox regression was performed and reported as hazard ratios with 95% confidence intervals (CIs). In total, 10 463 rivaroxaban and 26 494 warfarin users were followed for a mean of 16 ± 9 (range, 4-39) months. Duration of anticoagulation was similar between cohorts (median = 6 months). Rivaroxaban was associated with a 23% (95% CI: 16-30) reduced hazard of PTS versus warfarin. Rivaroxaban was associated with a significant risk reduction in symptoms of PTS compared to warfarin in patients with VTE treated in routine practice.
Introduction
Postthrombotic syndrome (PTS) is a frequent complication of deep vein thrombosis (DVT) with or without pulmonary embolism (PE), with prospective studies reporting anywhere from 20% to 50% of patients with DVT developing PTS. 1 Signs and symptoms of PTS can vary from patient to patient but often include pain, swelling, heaviness, fatigue, itching, and cramping at night in the affected limb. 1 Postthrombotic syndrome can reduce patients’ health-related quality of life and increase health-care costs. 2–3 The mean cost of PTS treatment in the United States (US) has been estimated at ∼US$7000 per patient per year. 3
Elastic compression stockings have had a controversial role in the prevention of PTS because of sparse and often conflicting data backing their use 1 and therefore increasing the importance of optimizing anticoagulation in this setting. Patients with venous thromboembolism (VTE) treated with a vitamin K antagonist (VKA) often spend substantial portions of time below their target international normalized ratio (INR) range of 2 to 3. 4–5 Suboptimal anticoagulation of DVT may result in VTE recurrence, insufficient or slower thrombus resolution, persistent venous obstruction and insufficiency, venous valve damage and impaired microcirculation, and eventually PTS. 1,6–7 In the EINSTEIN clinical trial program, rivaroxaban has been shown to be at least as effective as enoxaparin/VKA in the acute treatment and secondary prevention of recurrent VTE in patients with a creatinine clearance >30 mL/min, with a 46% (P = .002) decreased risk of major bleeding. 8 –10 Rivaroxaban is characterized by a rapid onset of anticoagulation activity (peak factor Xa inhibition within 2 to 4 hours after oral administration) 11 and predictable pharmacologic profile compared to VKAs. Moreover, a post hoc analysis of a small sample from the EINSTEIN DVT trial suggested that rivaroxaban could be associated with a reduced incidence of PTS. 12
A scientific statement on evidence-based prevention, diagnosis, and treatment strategies for PTS published by the American Heart Association (AHA) 1 notes that there is “a pressing need” for research evaluating the effectiveness of direct-acting oral anticoagulants (DOACs) to reduce the occurrence of PTS. Therefore, the objective of this study was to assess the relative hazard of PTS among patients with VTE treated with rivaroxaban or warfarin in routine US clinical practice.
Materials and Methods
This study report was written in compliance with the STrengthening the Reporting of OBservational studies in Epidemiology statement. 13
We performed a retrospective claims database study using US Truven MarketScan data from January 2012 to June 2015. MarketScan combines 2 separate databases, a commercial and a Medicare supplemental database, to cover all age groups, and as of March 2017 contains claims from 260 contributing employers, 40 contributing health plans, and government and public organizations representing nearly 240 million covered American lives. 14 Truven MarketScan captures health plan enrollment records, participant demographics, International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) diagnosis codes, Current Procedural Technology, Fourth Revision (CPT-4) procedure codes, admission and discharge dates, inpatient mortality data, outpatient medical services data, and prescription dispensing records. All data included in the Truven MarketScan databases are de-identified and are in compliance with the Health Insurance Portability and Accountability Act of 1996 to preserve participant anonymity and confidentiality. For this reason, this study was exempt from institutional review board oversight.
To be included in the present study, patients had to be ≥18 years of age with a primary discharge diagnosis code for DVT (ICD-9-CM = 451.1, 451.2, 453.40, 2453.41, 453.42, 453.8, 453.9) or PE (ICD-9-CM = 415.1x) during a hospitalization or emergency department visit (index event), 15 filling their first prescription for rivaroxaban or warfarin within 30 days of the index event and have ≥6 months of continuous medical and prescription benefits prior to the index event (baseline period). The patients with PE (regardless of whether there was a concomitant diagnosis code for DVT) were included since it has been demonstrated that patients with a majority symptomatic PE also have DVT (symptomatic or asymptomatic). 16–17 Patients with <4-month follow-up postindex event, only an outpatient diagnosis code for VTE (which has been shown poorly predictive of acute VTE 15 ) or a VTE claim or prescription claim for an outpatient anticoagulant during the baseline period, were excluded. This limited our population to patients who had not experienced a recent VTE event and those receiving anticoagulation for other indications (eg, atrial fibrillation). Given the large number of patients available in claims database analyses, no calculations to estimate required sample size were performed; rather all eligible patients meeting inclusion/exclusion criteria were analyzed.
The primary end point for this study was the development of PTS (symptoms of PTS). A secondary end point was the development of PTS with venous ulcer. No specific ICD-9-CM code(s) exist to indicate a diagnosis of PTS are available 1 ; therefore, the occurrence of symptoms of PTS during follow-up was determined using an algorithm developed by MacDougall and colleagues 18 and used in multiple prior claims database studies. 19–20 The algorithm takes into account the syndrome, often waxing-and-waning nature of the disease. 1,18 The MacDougall algorithm 18 defines PTS as a code for ≥1 extremity venous study including Doppler waveform analysis or venous plethysmography (CPT-4 = 93 965-93 971) along with diagnosis code(s) for both pain (ICD-9-CM = 729.5) and swelling of the limb (ICD-9-CM = 729.81) within 7 days of each other, lower extremity varicose veins (ICD-9-CM = 454.xx) with or without ulcer and/or inflammation, postphlebitic syndrome (ICD-9-CM = 459.1x) with or without ulcer and/or inflammation, or other disorder of the circulatory system (ICD-9-CM = 459.8x) at least 3 months after the index VTE event (Supplemental Table 1). Diagnosis and procedure codes could be identified in any (primary or nonprimary) coding position. The 3-month delay in our study for identifying PTS was chosen based on scientific statements from the International Society on Thrombosis and Hemostasis 21 and the AHA 1 that recommend PTS not be diagnosed before 3-month postevent to avoid inappropriately attributing acute signs and symptoms to the PTS. Moreover, prior claims-based studies using the MacDougall algorithm have employed a similar 3-month gap. 19–20 In our study, patients were followed until the development of PTS, disenrollment from their insurance plan, or end-of-study follow-up.
To adjust for potential confounding resulting from imbalances in baseline patient characteristics, we utilized inverse probability of treatment weighting (IPTW) based on the propensity score. 22 Inverse probability of treatment weighting uses propensity scores (predicted probability of initiating a specific oral anticoagulants given baseline characteristics) to generate patient-specific weights to adjust for any baseline imbalances. Propensity scores were calculated using multivariable logistic regression incorporating patient demographics, comorbidities, known VTE risk factors, and concomitant nonoral anticoagulant medications identified during the 6-month baseline period. Residual differences in baseline characteristics between weighted cohorts were assessed by calculating absolute standardized differences (the systematic differences in observed baseline characteristics), with differences <0.1 considered well balanced. 22
Baseline patient characteristics were analyzed using descriptive statistics. Cox proportional hazard regression was performed and results reported as adjusted hazard ratios (HRs) with accompanying 95% confidence intervals (CIs). Adjusted incidence rate differences (AIRD) were estimated using IPTW event counts and follow-up time for each index oral anticoagulant group. Because all baseline characteristics were balanced after adjustment using IPTW, our Cox regression models included only index oral anticoagulant treatment received (rivaroxaban or warfarin) as an independent variable.
We performed subgroup analyses to examine the impact of age (<60 or 60+ years), initial VTE diagnosis (presence or absence of PE), and sex on the effectiveness of rivaroxaban (vs warfarin) in preventing PTS. We also performed sensitivity analyses in which we restricted the PTS end point to only those codes associated with ulcer (ICD-9-CM = 459.11, 459.13, 454.0, 454.2) which by the Villalta Scale would automatically be severe PTS, 1 allowing patients to be newly started on rivaroxaban or warfarin within 60 days of the index event instead of 30 days, and upon requiring a 6-month time gap following the index VTE before PTS could be diagnosed. 1,21
All statistical analyses were performed using SAS version 9.4 (SAS Inc., Cary, North Carolina). A P value <.05 was considered statistically significant in all cases.
Results
In total, this study evaluated 10 463 rivaroxaban and 26 494 warfarin users meeting inclusion/exclusion criteria (Figure 1). Included patients were followed for a mean of 16 ± 9 months (range, 4-39 months), and rivaroxaban and warfarin users had similar durations of anticoagulation (mean = 7 months; median = 6 months for both cohorts) and times to first prescription claim (mean = 4 ± 8, range, 0-30 days vs 5 ± 4, range, 0-30 days, respectively). Based on the assessment of absolute standardized differences between the rivaroxaban and warfarin users, patients were deemed well balanced on all independent variables entered into the propensity score logistic regression model (Table 1).
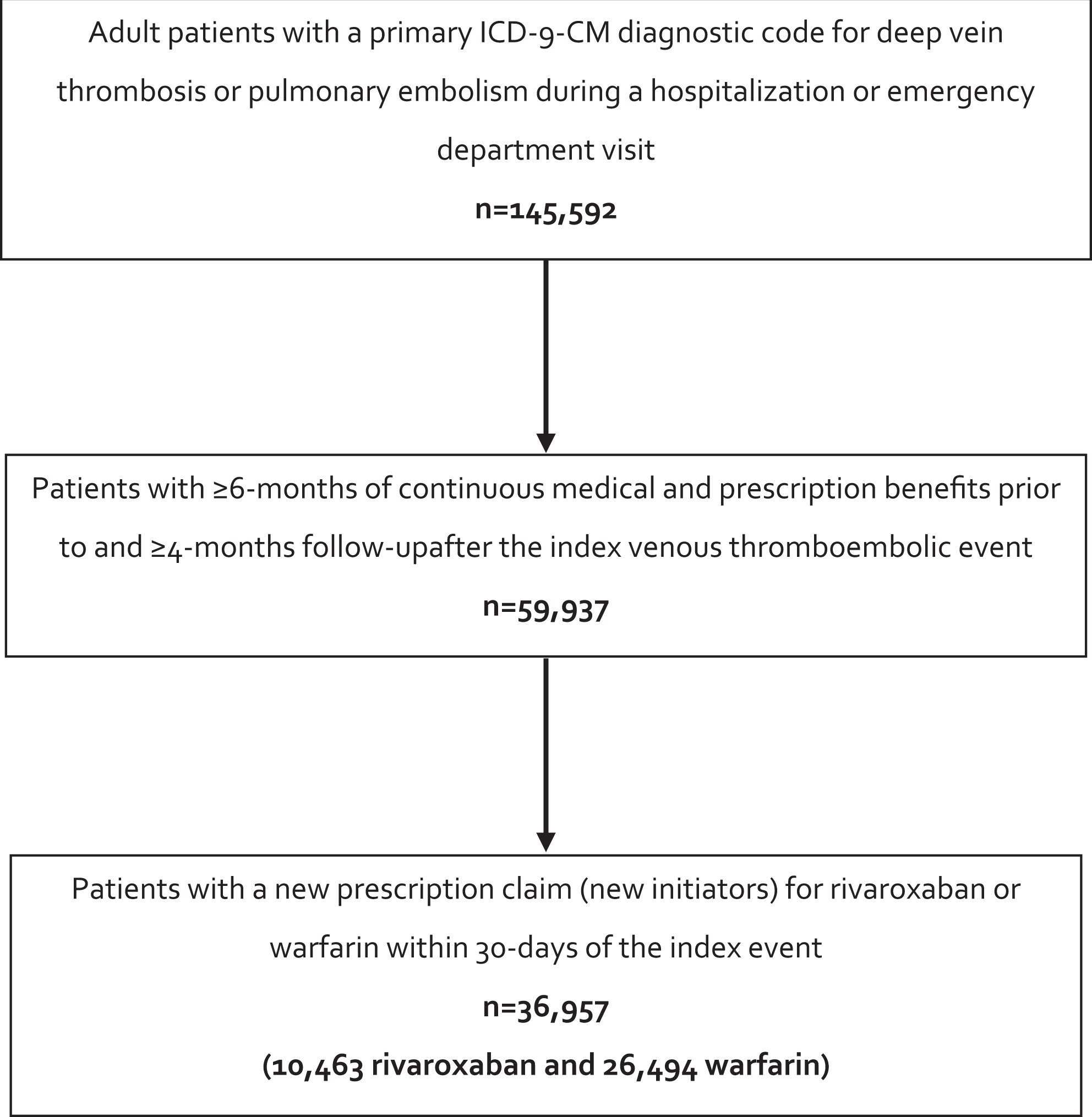
Patient inclusion and exclusion ICD. ICD-9-CM indicates International Classification of Diseases, Ninth Revision, Clinical Modification.
Baseline Characteristics of Weighted Rivaroxaban and Warfarin Cohorts.
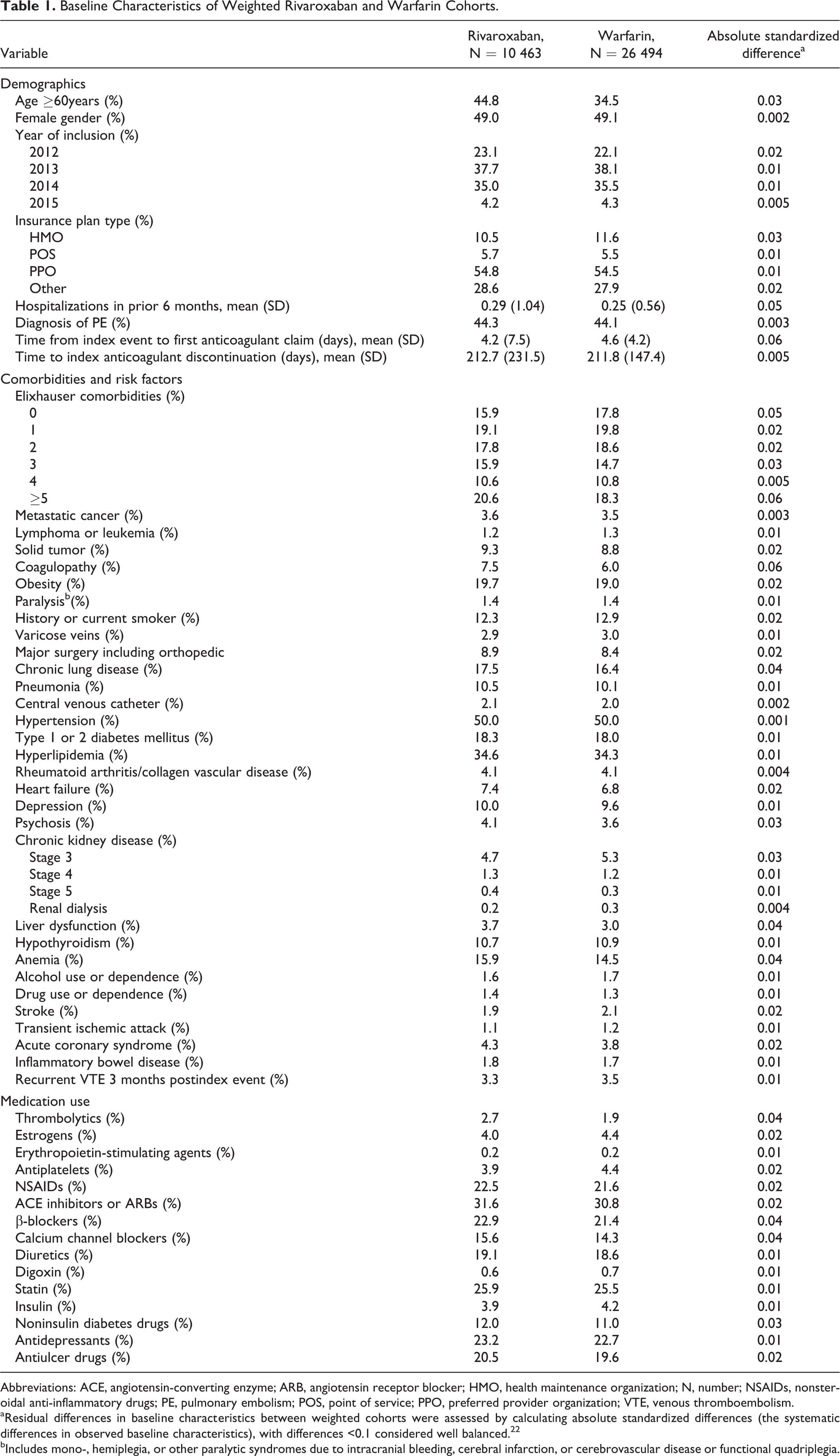
Abbreviations: ACE, angiotensin-converting enzyme; ARB, angiotensin receptor blocker; HMO, health maintenance organization; N, number; NSAIDs, nonsteroidal anti-inflammatory drugs; PE, pulmonary embolism; POS, point of service; PPO, preferred provider organization; VTE, venous thromboembolism.
aResidual differences in baseline characteristics between weighted cohorts were assessed by calculating absolute standardized differences (the systematic differences in observed baseline characteristics), with differences <0.1 considered well balanced. 22
bIncludes mono-, hemiplegia, or other paralytic syndromes due to intracranial bleeding, cerebral infarction, or cerebrovascular disease or functional quadriplegia.
In total, 2418 PTS events were identified during follow-up, of which 720 (29.8%) were associated with a venous ulcer ICD9-CM code. Upon Cox proportion hazard regression, rivaroxaban was found to be associated with a significant 23% reduced hazard of developing PTS compared to warfarin (adjusted rates = 3.69 vs 4.73 events per 100 person-years, respectively; Figure 2). This corresponded to an AIRD of 1.04 fewer events per 100 person-years of follow-up in favor of rivaroxaban. Reductions in the hazard of developing PTS with rivaroxaban were consistent across subgroups (HR range, 0.60-0.85, P < .05 for all; Figure 3). Rivaroxaban continued to be associated with a reduced risk of PTS when the end point was restricted to only PTS with venous ulcer (adjusted rates = 1.11 vs 1.38 events per 100 person-years, respectively; HR = 0.81, 95% CI: 0.70-0.94, P = .006; Figure 4), when time to new oral anticoagulation start could be extended up to 60 days from the index VTE event (HR = 0.86, 95% CI: 0.79-0.93, P = .0002) and when a ≥6-month postindex event gap was required before PTS diagnosis (HR = 0.76, 95% CI: 0.69-0.85, P < .0001).
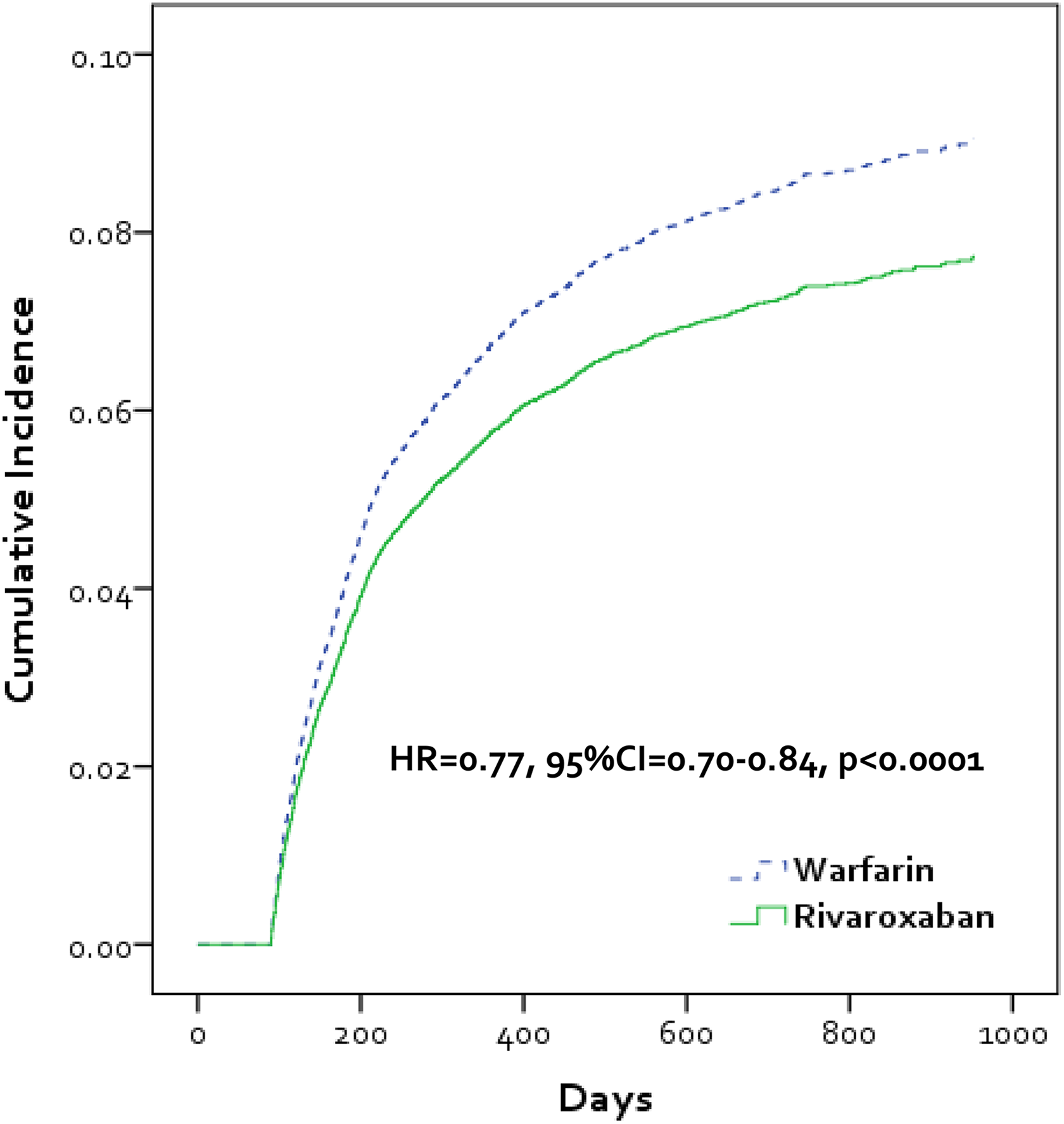
Kaplan-Meier curve depicting cumulative incidence of postthrombotic syndrome in patients treated with rivaroxaban or warfarin for venous thromboembolism. CI indicates confidence interval; HR, hazard ratio.
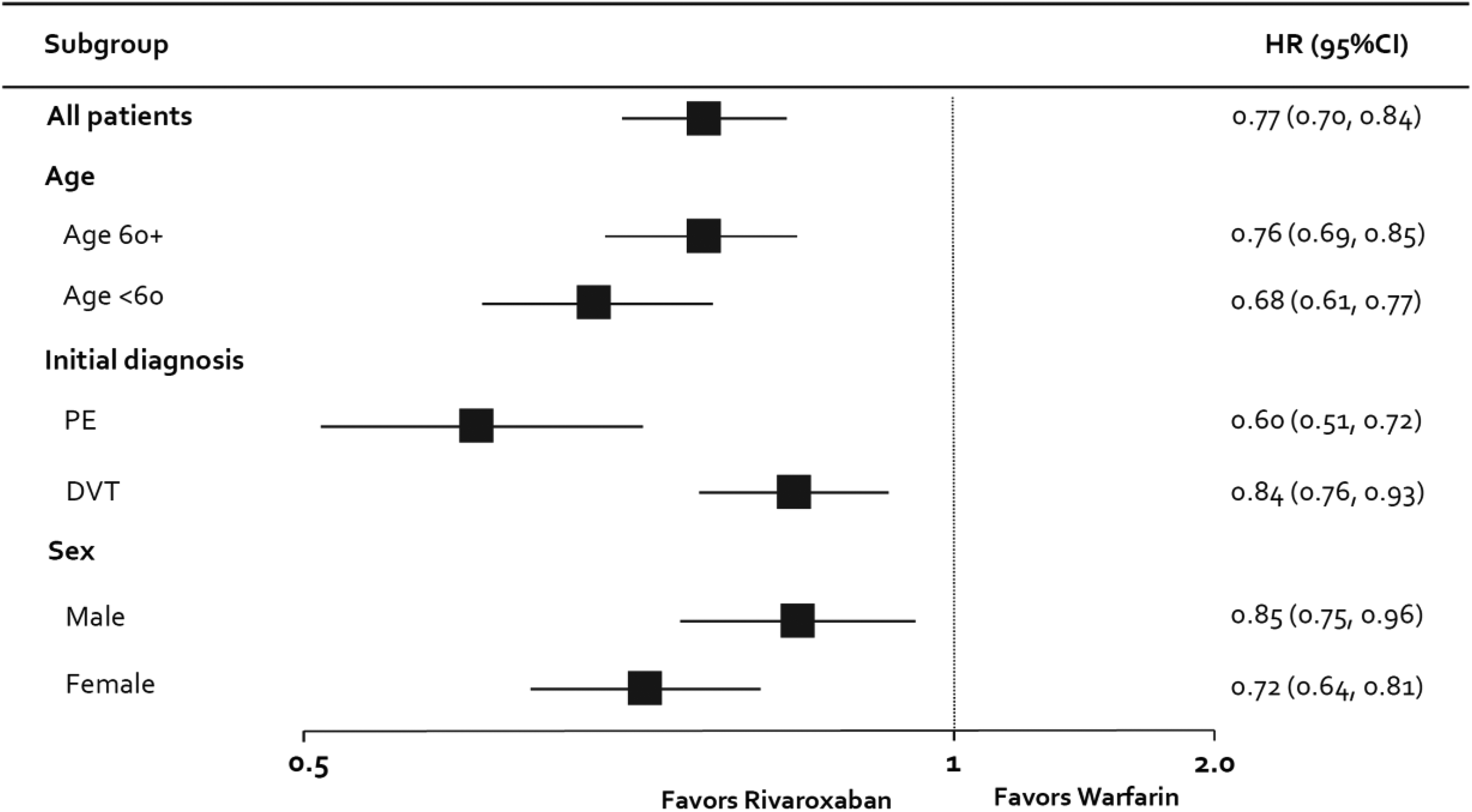
Development of postthrombotic syndrome in patients treated with rivaroxaban or warfarin for venous thromboembolism*. * denotes P < .05 for all rivaroxaban versus warfarin subgroup comparisons. CI indicates confidence interval; DVT, deep vein thrombosis; HR, hazard ratio; N, number; PE, pulmonary embolism.
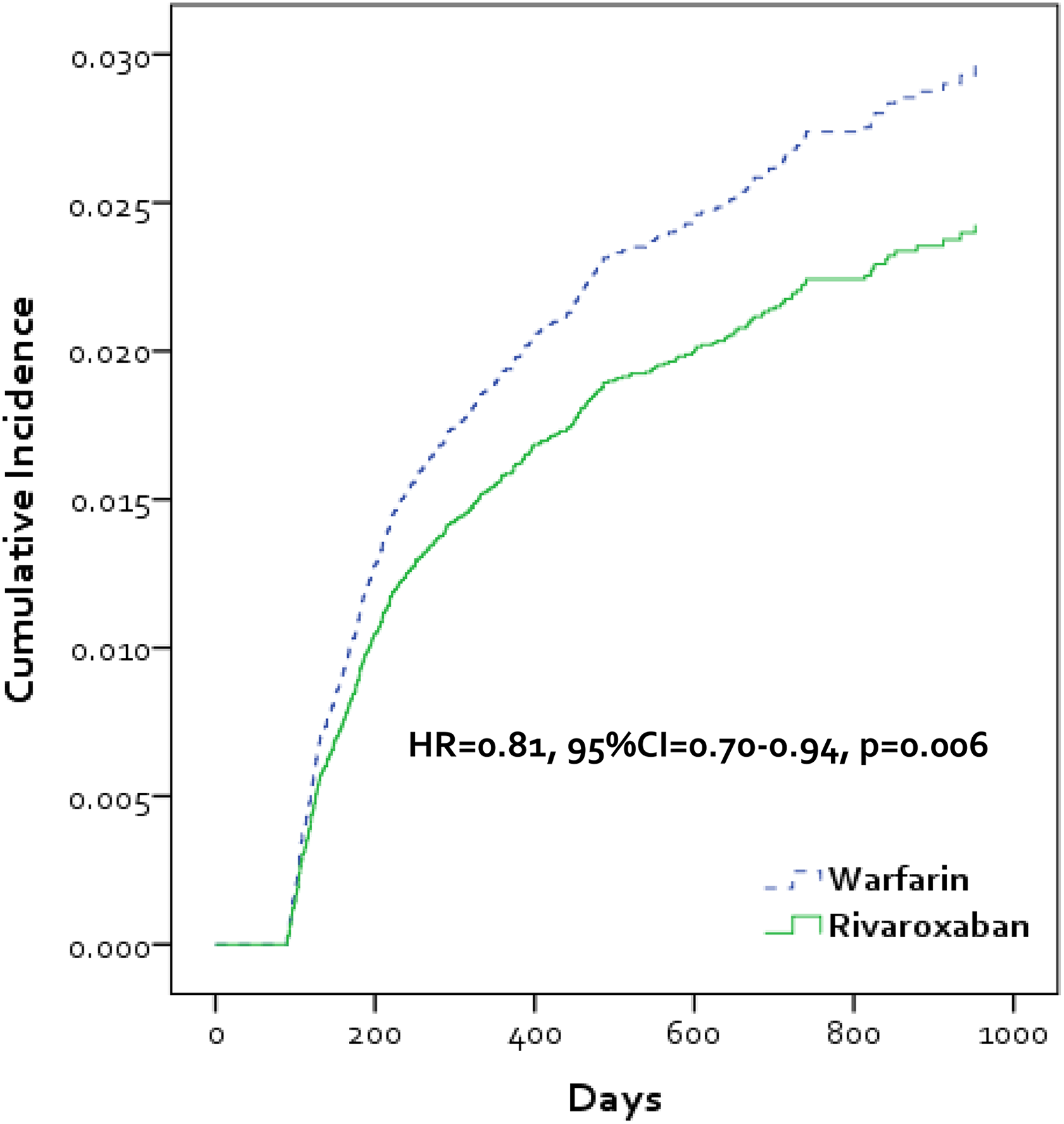
Kaplan-Meier curve depicting cumulative incidence of postthrombotic syndrome with venous ulcer in patients treated with rivaroxaban or warfarin for venous thromboembolism. CI indicates confidence interval; HR, hazard ratio.
Discussion
This study performed in the US MarketScan administrative claims databases evaluated the risk of PTS in patients with VTE when anticoagulated with either rivaroxaban or warfarin. Analysis demonstrated that rivaroxaban use was associated with a significantly reduced hazard of developing PTS compared to warfarin users (HR = 0.77, AIRD = 1.04 events per 100 person-years) and PTS associated with venous ulcer (HR = 0.81, AIRD = 0.27 events per 100 person-years). This finding of a significantly reduced PTS rate with rivaroxaban was observed across various patient subgroups (HR range, 0.60-0.85, P < .05 for all) and sensitivity analyses (HR range, 0.76-0.86, P < .05 for all). As the subgroup and sensitivity analyses’ HRs were often based on differing size populations or event rates (affecting estimate precision), we caution against the overinterpretation of these results.
There is limited published data evaluating the impact of DOACs on the incidence of PTS following a DVT and/or PE. Cheung and colleagues 12 performed a post hoc analysis of a small subset of patients with DVT (without symptomatic PE) enrolled in the EINSTEIN-DVT randomized controlled trial (RCT) to assess the impact of rivaroxaban versus enoxaparin bridging to a VKA in preventing PTS. The investigators followed a total of 336 patients for a median of 57 months (∼4.75 years) for the occurrence of PTS diagnosed based upon a Villalta score ≥5. 12,23 Forty-five of 162 rivaroxaban (estimated rate ∼5.8%/year) and 66 of 174 enoxaparin/VKA participants (estimated rate ∼8.0%/year) developed PTS (HR = 0.76, 95% CI: 0.51-1.13, P = .18) during follow-up. Therefore, the HRs (0.77 and 0.76) and absolute rates (3.4 vs 4.7 per 100 person-years in our analysis compared to 5.8 vs 8.0 per 100 person-years in EINSTEIN) for PTS with rivaroxaban versus conventional anticoagulation observed in both studies were relatively similar. Importantly, we feel that the similarity in rates detected in both studies supports the validity of our claims-based (MacDougall algorithm) approach to PTS identification. The lower rates of PTS observed in our claims analysis compared to EINSTEIN might be explained by a failure of clinicians to code for more mild cases of PTS (which were frequent in EINSTEIN) and/or EINSTEIN’s use of an objective assessment for PTS. 12 It has been suggested that providing anticoagulation at an appropriate intensity (and duration), particularly during the first week after a DVT, is an important means of preventing PTS. 1,6–7 As part of the prospective Recurrent Venous thromboembolism Risk Stratification Evaluation study, 6 the odds of a patient with DVT ± PE developing PTS were shown to be 1.84-fold (P < .05) higher during the first 3 months of treatment in patients with an INR <2.0 at least 20% of the time. Unfortunately, studies have frequently demonstrated that patients with VTE spend only about one-half of their time in the target INR range of 2.0 to 3.0, with a strong tendency toward subtherapeutic anticoagulation (∼42% below range in the first month of treatment, 35% in 1-3 months, and 24.1% in 1-6 months). 5 Moreover, there are significantly more drug–drug interactions with warfarin that can both impact INR control and decrease its effectiveness and increase bleeding risk. Direct-acting oral anticoagulants such as rivaroxaban have a rapid onset of anticoagulation activity and a predictable pharmacologic profile which allows them to surmount the early subtherapeutic anticoagulation frequently observed with VKAs and allow for substantially simplified perioperative anticoagulation management by allowing prescribers to stop and restart at the appropriate time with no need for parenteral overlap or bridging therapy in the procedural setting. 24
Both residual thrombosis burden and incomplete resolution of leg symptoms and signs at 1 month after DVT have been shown to be important risk factors for PTS development. 1 Consequently, data from the phase II Oral Direct Factor Xa Inhibitor BAY 59-7939 in Patients With Acute Symptomatic Deep-Vein Thrombosis -DVT trial of rivaroxaban showing faster and more extensive clot resolution earlier after treatment provides an additional potential mechanism underlying our finding that rivaroxaban was associated with less PTS than conventional anticoagulation. 25 In this study, Agnelli and colleagues performed ultrasound estimation of clot burden on the day of DVT diagnosis as well as days 21 and 84. At day 21 following a DVT, more than half of patients who received rivaroxaban twice daily experienced an improvement of ≥4 points in thrombus score (experienced improved clot resolution) compared to 45.9% in those receiving enoxaparin/VKA; however, by day 84, these differences were no longer evident.
It is important to note that PTS has been associated with poorer quality of life in patients with VTE. In a meta-analysis performed by Lubberts and colleagues, 26 the development of PTS was associated with worse patient-reported physical health (P < .001, n = 7 studies), mental health (P < .001, n = 7 studies), and disease-specific quality of life (P < .001, n = 10 studies). Thus, potentially reducing PTS by utilizing anticoagulants shown to reduce PTS risk could yield dramatic patient-perceived benefits. 26–27 Unfortunately, we were unable to assess differences in patient quality of life between cohorts as such data were not available in the Truven MarketScan database. The ability of DOACs, including rivaroxaban, to improve quality of life of patient with VTE by preventing PTS merits prospective study evaluation.
As a retrospective analysis of US claims data, our study has limitations worthy of discussion. First, as we used US claims data only, our results will likely be most applicable to a US population. Second, misclassification and sampling biases are always important limitations in administrative claims database studies.
28
Third, while propensity score
22
can aid in generating cohorts that are comparable in key characteristics, only those variables measured in the Truven MarketScan databases
14
could be adjusted upon using IPTW in this analysis. Therefore, residual confounding cannot be excluded regardless of the sophistication of the methodology and the number of variables used in developing patients’ propensity scores.
28
Fourth, the majority of administrative claims databases, including Truven MarketScan, are hindered by insufficient reporting of some clinical (eg, inpatient anticoagulation, DVT location or thrombus burden, use of elastic compression stockings) and laboratory (eg, INR,
In conclusion, this large administrative claims database study suggests that rivaroxaban is associated with less PTS and less PTS associated with venous ulcers compared to warfarin in patients with VTE managed in routine US clinical practice. These findings are consistent with those from a post hoc analysis of the EINSTEIN-DVT trial. Larger randomized controlled trials evaluating the potential benefits of rivaroxaban on PTS incidence are warranted.
Supplemental Material
SUPPLEMENTAL_APPENDIX - Postthrombotic Syndrome in Patients Treated With Rivaroxaban or Warfarin for Venous Thromboembolism
SUPPLEMENTAL_APPENDIX for Postthrombotic Syndrome in Patients Treated With Rivaroxaban or Warfarin for Venous Thromboembolism by Craig I. Coleman, Jan Beyer-Westendorf, Thomas J. Bunz, Charles E. Mahan, and Alex C. Spyropoulos in Clinical and Applied Thrombosis/Hemostasis
Footnotes
Authors’ Note
All authors contributed to the design, analysis, interpretation of data, drafting the article, or revising it critically for important intellectual content and approved the final version to be published. Dr Coleman is the senior and corresponding author and guarantor. The lead author (Craig I. Coleman) affirms that the manuscript is an honest, accurate, and transparent account of the study being reported, that no important aspects of the study have been omitted, and that any discrepancies from the study as planned (and, if relevant, registered) have been explained. Data sharing is not possible because US Truven MarketScan owns and licenses the utilized data.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Dr Coleman has served as a consultant for Boehringer Ingelheim, Janssen Scientific Affairs, Bayer AG and Portola; Dr Beyer-Westendorf has served as a consultant to and has received honoraria from Bayer, Boehringer Ingelheim, Daiichi Sankyo, Pfizer, Portola, CSL Behring, and Medscape. Dr Mahan has served as a consultant for Portola, Point of Care Software Solutions, Daiichi-Sanyko, Sanofi-Aventis, Boehringer Ingelheim, Johnson and Johnson, Polymedix Inc, Leo, Eisai, and New York Hospital Association. He has also served as a speaker for Janssen, Bristol Myers Squibb, Pfizer, Sanofi-Aventis, Portola, and Boehringer Ingelheim; Dr Spyropoulos has served as a consultant for Boehringer Ingelheim, Janssen, Bayer Healthcare, and Daiichi Sankyo and has served on advisory committees for Bristol-Myers Squibb, Pfizer, Janssen, Portola, and Bayer Healthcare.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Bayer AG, Berlin, Germany, for the submitted work; Dr Coleman has received research grants from Bayer AG and Janssen Scientific Affairs, LLC. Dr Beyer-Westendorf has received research grants from Bayer, Boehringer Ingelheim, Daiichi Sankyo, Pfizer, and Portola.
Supplemental Material
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.