
Abstract
Background:
Few studies have identified patterns and predictors of use of direct oral anticoagulants for venous thromboembolism (VTE).
Objective:
To describe the use of anticoagulants and assess predictors associated with the prescription of rivaroxaban over vitamin K antagonist (VKA) for the subsequent treatment of VTE.
Methods:
This cross-sectional study was built with all consecutive patients newly diagnosed with acute VTE admitted between February 18, 2013, and September 18, 2013, in an academic tertiary care center in Quebec, Canada. Patient characteristics and VTE treatments were described. Univariate analyses and a multiple forward stepwise logistic regression were performed to assess predictors of rivaroxaban use over VKA for the subsequent treatment of VTE.
Results:
The study included 256 patients, 36.7% with a diagnosis of deep vein thrombosis (DVT) and 63.3% with pulmonary embolism (PE). Mean age was 63.1 years, and 28.1% of patients had cancer-associated VTE. Overall, rivaroxaban was prescribed in 1.6% of patients for the initial treatment and in nearly 20% of patients for the subsequent treatment of VTE. Low-molecular-weight heparin and VKA were mostly prescribed. Independent predictors associated with the prescription of rivaroxaban over VKA were as follows: age < 65 years (OR: 2.86, 95% CI 1.29-6.37), a diagnosis of DVT versus PE (OR 2.54, 95% CI 1.20-5.40), and an emergency department visit rather than a hospitalization (OR 2.24, 95% CI 1.06-4.71).
Conclusion:
Several months following its availability, rivaroxaban was rarely prescribed for acute VTE disease. It also appears to be prescribed in different patient populations than VKA.
Introduction
In the general population, the annual incidence of venous thromboembolism (VTE) is between 1 and 2 events per 1000 adults. 1 Anticoagulants are essential and effective in treating VTE symptoms, preventing pulmonary embolism (PE) in patients with deep vein thrombosis (DVT), and decreasing the risks of recurrent VTE and death. 2 However, they are associated with bleeding risks, and nearly 2% of patients will experience a major hemorrhage during a long-term treatment with an oral anticoagulant (vitamin K antagonist [VKA]), which may be fatal. 3 Standard treatment of VTE includes initial therapy with a parenteral anticoagulant such as unfractionated heparin (UFH), low-molecular-weight heparin (LMWH), or fondaparinux, followed by an oral VKA for at least 3 months. 4 Because the onset of anticoagulant activity with VKA is delayed for several days, an initial period of overlap with parenteral anticoagulant is used. 5 Vitamin K antagonists also require frequent monitoring of the anticoagulant activity and dose adjustments. These drugs are associated with numerous drug interactions. 6,7 An oral direct Xa inhibitor, rivaroxaban (Xarelto®; Bayer Inc., Ontario, Canada), was the first direct oral anticoagulant approved for the treatment of VTE in Canada. Rivaroxaban (15 mg twice daily for 3 weeks, followed by 20 mg once daily) has been shown to be noninferior to standard therapy (enoxaparin [LMWH] followed by a VKA) in the treatment of VTE in terms of recurrent events and major hemorrhages. 8,9 It is easier to use by patients and physicians: It has a rapid onset of action, fewer drug interactions, fixed doses are given, and there is no need for anticoagulant activity monitoring. 2,10 However, there is no specific antidote currently available to reverse its anticoagulant activity. 10 Moreover, reimbursement of rivaroxaban in patients with public medication insurance in the Canadian province of Quebec is currently restricted to those who cannot use a VKA. 11 All of these factors may limit the use of rivaroxaban.
The availability of rivaroxaban in Canada might have brought important changes in current practice, but little data are available on its real-life use. Since its arrival, physicians have had the choice between 2 different classes of oral agents, and they have had to balance the risks and benefits of each one according to the type of patients treated. Despite some advantages of rivaroxaban over VKA, it is currently unknown how commonly it is prescribed and in what type of patients. Therefore, the main objectives of this study were to describe patterns of use of anticoagulants for the treatment of VTE following the introduction of rivaroxaban in an academic tertiary care center and to determine the predictors of choice of oral anticoagulant (rivaroxaban over VKA) prescribed at hospital discharge for the subsequent treatment of acute VTE.
Methods
Study Design and Setting
This cross-sectional study was conducted at a 677-bed academic tertiary care center in Quebec, Canada. The study included all consecutive patients admitted to the emergency department (ED) or hospitalized between February 18, 2013, and September 18, 2013 (ie, starting 2 months following the approval of rivaroxaban for the treatment of DVT at this institution) for an acute DVT and/or PE. Patients with a diagnosis of DVT and/or PE were identified in the hospital database using the Tenth Revision of the International Classification of Diseases (ICD-10 codes I26.xx and I82.xx).
Patients
Adult patients were included if they had a diagnosis of DVT and/or PE documented in the ED consultation sheet or in the discharge summary during the study period and had at least 1 dose of anticoagulant at therapeutic dosage (ie, for VTE treatment, not prophylaxis) documented in the medication administration record. Patients were excluded if they had a diagnosis of superficial vein thrombosis in the absence of DVT, a documented prescription for an anticoagulant at therapeutic dosage in the last 6 months, or a discontinuation of the anticoagulant therapy at hospital discharge.
Data Collection and Definitions
The electronic medical records (EMRs) of eligible patients were manually reviewed by a study investigator, and data were collected using a study-specific electronic case report form. Multiple sources of data were used: laboratory values (ie, on the day the subsequent anticoagulant treatment was initially prescribed or the closest value before prescription up to the first value available during the hospital stay), medical consultations, ED consultations, discharge summary, medical progress notes, prescriptions during the hospital stay, pharmacological profile of the community pharmacy, in-hospital medication administration record, and medication reconciliation sheet (documentation of drugs prescribed at home and at hospital discharge). Data on comorbidities were collected from medical/ED consultations, discharge summary, and medical progress notes. Variables were defined, and specific sources of data were determined at the beginning of the study to ensure a systematic data collection.
The patient characteristics collected included age, gender, body mass index (BMI), renal function (ie, estimated glomerular filtration rate [eGFR] reported in the laboratory values and calculated with the Chronic Kidney Disease Epidemiology Collaboration [CKD-EPI] equation 12 ), VTE diagnosis (ie, DVT, PE, or both), DVT diagnosis (ie, proximal: thrombosis of the popliteal, femoral, or iliac vein; distal: thrombosis of the peroneal, posterior, anterior tibial vein or muscular vein; upper extremity, or other), length of hospital stay, presence of active cancer, previous VTE at any point in time, and the presence of thrombophilia (ie, antiphospholipid syndrome, antithrombin, protein C and S deficiencies, factor V Leiden, and prothrombin gene mutation 13 ).
In order to describe prescription patterns, the anticoagulant prescribed in the first 5 to 10 days of VTE was reported to be the initial treatment, and the anticoagulant prescribed following this period and at hospital discharge was defined as the subsequent treatment. 2
Risk factors for VTE recurrence and/or bleeding were considered potential predictors of rivaroxaban prescription over VKA for the subsequent management of acute VTE. A total of 25 predictors were selected based on the published literature, 14,15 expert opinions, and availability of the information in EMRs. These were age (<65 vs ≥65 years), gender (male vs female), eGFR, obesity (BMI ≥ 30 vs <30 kg/m2), 16 Charlson comorbidity index score, 17 polypharmacy (≥5 prescription drugs per day at hospital discharge vs <5), 18 dementia, atrial flutter or fibrillation, previous VTE, hospital status (ED visit only vs hospitalization), specialty of the prescriber (internal medicine vs others), diagnosis of VTE (DVT alone vs PE with or without DVT), unprovoked VTE (ie, not caused by a transient risk factor such as surgery, trauma, or fracture in the last 3 months, immobility ≥5 days, prolonged air or car travel, estrogen therapy, pregnancy, or postpartum), 13,19 presence of active cancer, diabetes mellitus, thrombophilia, dyslipidemia, current smoking, renal impairment (ie, on dialysis, renal transplant, or a serum creatinine value >200 µmol/L), 15 hepatic impairment (ie, documentation of chronic hepatic disease (eg, cirrhosis), bilirubin value >2 times the upper limit of normal or aspartate aminotransferase/alanine aminotransferase/alkaline phosphatase >3 times the upper limit of normal), 15 hypertension, anemia, bleeding (ie, antecedent of bleeding, active bleeding at admission, or episode of bleeding that occurred during the hospital stay and documented in the medical chart), concomitant use of antiplatelets, and history of falls.
Data Analysis
The baseline patient characteristics were presented as means with standard deviations or medians with interquartile ranges for continuous variables. Categorical variables were expressed as frequencies and percentages.
Univariate analyses were performed to evaluate the association between the potential predictors and the choice of the oral anticoagulant (rivaroxaban over VKA) prescribed at hospital discharge for the subsequent treatment of VTE. Student t test or Mann-Whitney U test was used to compare continuous variables, and categorical variables were analyzed by χ2 test or Fisher exact test. P values, crude odds ratios (OR), and 95% confidence intervals (CI) were reported for each potential predictor. Subsequently, potential predictors with a P value less than .05 were analyzed using a multiple logistic regression analysis by forward stepwise method. For this analysis, the hot deck imputation method using the deterministic selection was used to handle missing data and thus to reduce nonresponse bias. 20,21 The basic property of this method is that each missing value is replaced with the value of a patient with similar characteristics. Adjusted OR and 95% CI were reported for each variable in the final model. Associations were considered statistically significant when the P values were <.05. Statistical analyses were performed using the SPSS software, version 22.0 (IBM Corp, Armonk, New York). The conduct of this study was approved by the Ethics Committee of the Centre hospitalier universitaire de Sherbrooke (CHUS) academic health center.
Results
Patient Characteristics
A total of 256 patients with acute VTE were included in this study. Mean age was 63.1 years, and 48.8% of patients were male (Table 1). Most had a normal BMI (66.1%), and fewer than half (42.5%) had a normal eGFR of at least 90 mL/min/1.73 m2. The median length of hospital stay was 5.5 days, excluding patients admitted to the ED only and patients admitted for another primary diagnosis that had developed VTE during hospitalization. Pulmonary embolism (with or without DVT) was the main diagnosis of VTE (63.3%). Overall, 28% of patients had cancer-associated VTE, about 17% had a history of a thromboembolic event, and 5% of patients had a diagnosed thrombophilia.
Baseline Characteristics for All Patients According to the Type of Anticoagulant Prescribed at Hospital Discharge for the Subsequent Treatment of VTE.
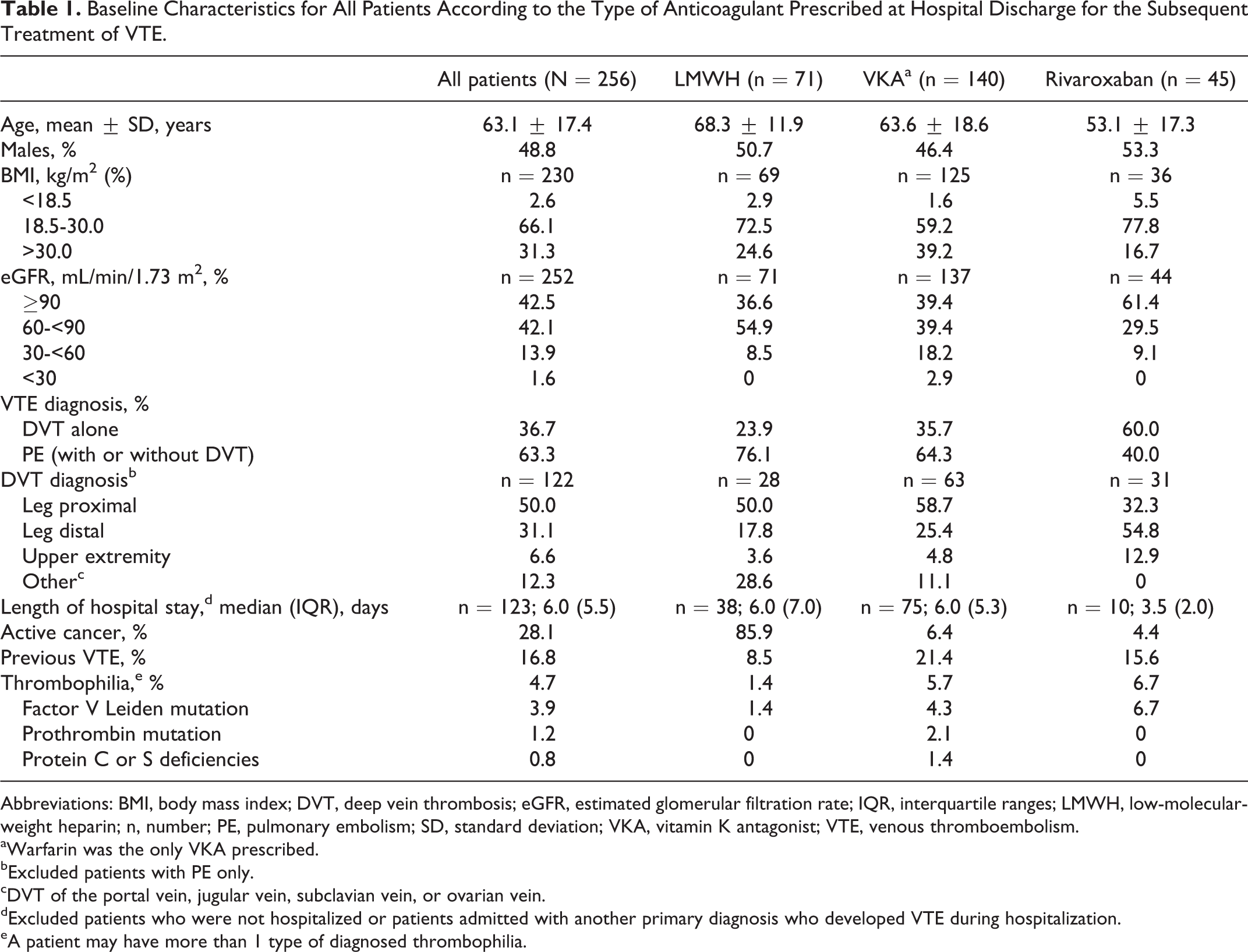
Abbreviations: BMI, body mass index; DVT, deep vein thrombosis; eGFR, estimated glomerular filtration rate; IQR, interquartile ranges; LMWH, low-molecular-weight heparin; n, number; PE, pulmonary embolism; SD, standard deviation; VKA, vitamin K antagonist; VTE, venous thromboembolism.
aWarfarin was the only VKA prescribed.
bExcluded patients with PE only.
cDVT of the portal vein, jugular vein, subclavian vein, or ovarian vein.
dExcluded patients who were not hospitalized or patients admitted with another primary diagnosis who developed VTE during hospitalization.
eA patient may have more than 1 type of diagnosed thrombophilia.
Treatment of VTE
Overall, the most commonly prescribed anticoagulant therapy for the initial treatment of VTE was LMWH alone (61.7%; Table 2). Other anticoagulants prescribed were UFH, fondaparinux, or combinations of these. Few patients received rivaroxaban for the initial treatment of the disease. For the subsequent treatment of acute VTE, VKA (warfarin) was prescribed in 54.7% of patients and LMWH in monotherapy was prescribed in 27.7% of patients (85.9% of them had active cancer), while rivaroxaban was the least prescribed (17.6%). No trend toward a higher or lower use of rivaroxaban was observed during the course of the study (Figure 1).
Treatment of Acute VTE.
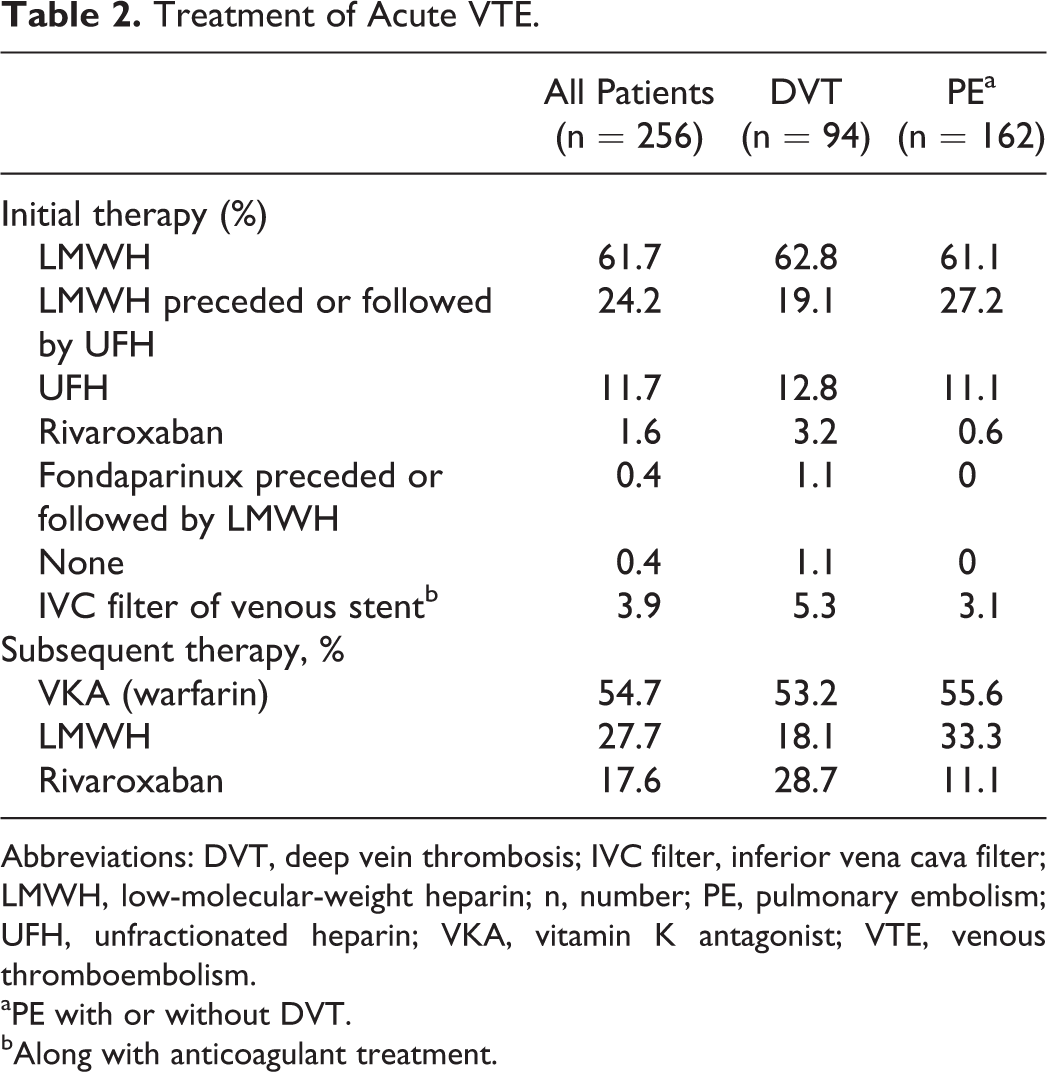
Abbreviations: DVT, deep vein thrombosis; IVC filter, inferior vena cava filter; LMWH, low-molecular-weight heparin; n, number; PE, pulmonary embolism; UFH, unfractionated heparin; VKA, vitamin K antagonist; VTE, venous thromboembolism.
aPE with or without DVT.
bAlong with anticoagulant treatment.
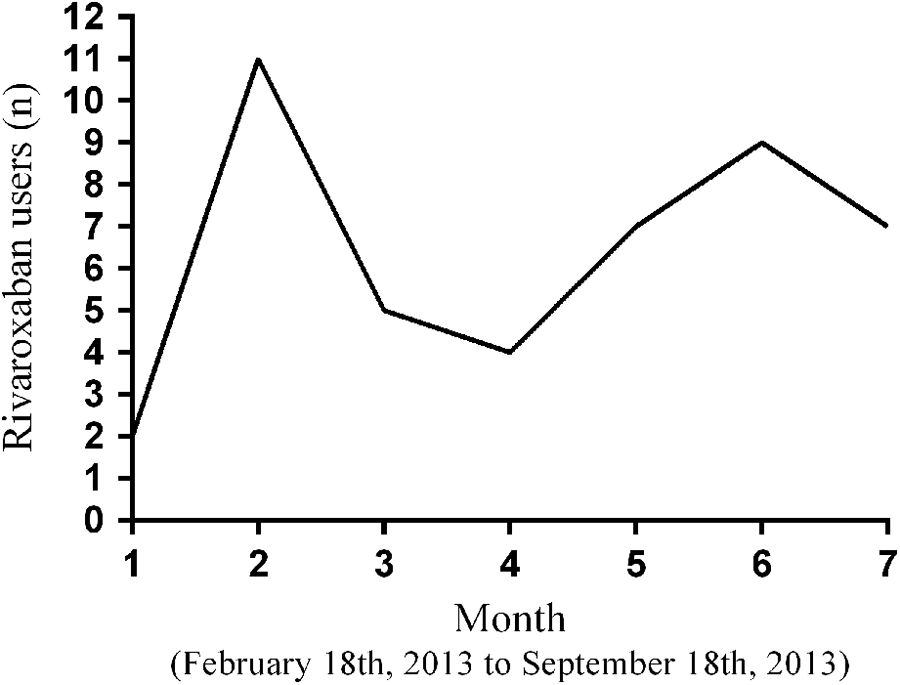
Monthly trend in the prescription of rivaroxaban for the subsequent treatment of VTE disease.
Predictors of Choice of Oral Anticoagulant for the Subsequent Treatment of VTE
Only patients who were prescribed an oral anticoagulant at hospital discharge were considered in this analysis (185 patients). Of the 25 predictors, 11 were significantly associated with the choice of the new oral anticoagulant over VKA in univariate analyses (Table 3). Patients in the rivaroxaban group were younger, had a greater mean eGFR, and had a lower median Charlson comorbidity score. This group also had lower percentages of patients with obesity, polypharmacy, unprovoked VTE, dyslipidemia, and hypertension and had greater percentages of patients with an emergency visit only and a diagnosis of DVT in the absence of PE.
Univariate Analyses of Potential Predictors of Rivaroxaban Prescription Over VKA for the Subsequent Treatment of VTE.
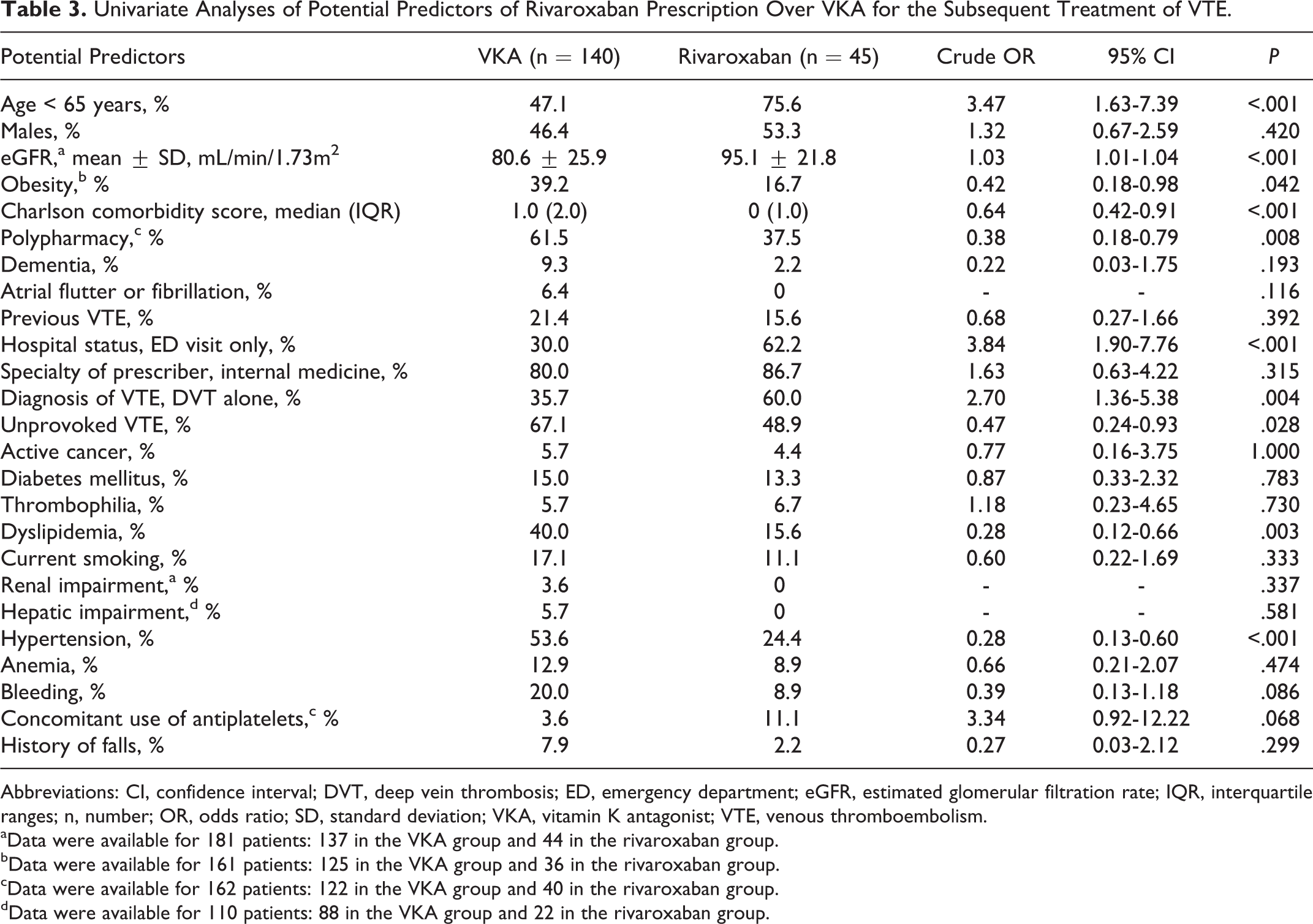
Abbreviations: CI, confidence interval; DVT, deep vein thrombosis; ED, emergency department; eGFR, estimated glomerular filtration rate; IQR, interquartile ranges; n, number; OR, odds ratio; SD, standard deviation; VKA, vitamin K antagonist; VTE, venous thromboembolism.
aData were available for 181 patients: 137 in the VKA group and 44 in the rivaroxaban group.
bData were available for 161 patients: 125 in the VKA group and 36 in the rivaroxaban group.
cData were available for 162 patients: 122 in the VKA group and 40 in the rivaroxaban group.
dData were available for 110 patients: 88 in the VKA group and 22 in the rivaroxaban group.
Estimated glomerular filtration rate was excluded from the multiple logistic regression analysis because it was highly correlated with age. Age was selected over eGFR because it had a strongest association with the choice of the anticoagulant in the univariate analysis. Charlson comorbidity score was also highly correlated with polymedication, and polymedication was excluded because of its high number of missing data. The hot deck imputation using a deterministic selection was performed only for the variable BMI since data were missing for 23 patients.
The multiple logistic regression analysis showed that age <65 years (adjusted OR: 2.86, 95% CI: 1.29-6.37), a diagnosis of DVT rather than a diagnosis of PE (adjusted OR: 2.54, 95% CI: 1.20-5.40), and an ED visit rather than a hospitalization (adjusted OR: 2.24, 95% CI: 1.06-4.71) were independent predictors of receiving rivaroxaban over VKA for the subsequent treatment of acute VTE (Table 4). The same conclusion was obtained with a stepwise backward selection method (data not shown).
Final Model of the Multiple Logistic Regression of Independent Predictors of Rivaroxaban Prescription Over VKA for the Subsequent Treatment of VTE.
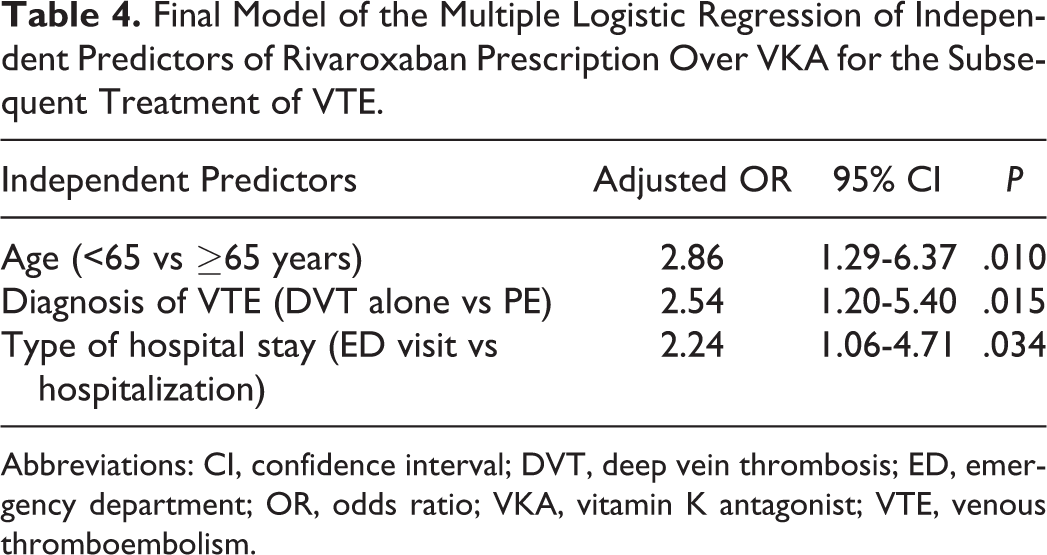
Abbreviations: CI, confidence interval; DVT, deep vein thrombosis; ED, emergency department; OR, odds ratio; VKA, vitamin K antagonist; VTE, venous thromboembolism.
Discussion
This study describes the use of anticoagulants for VTE following the approval of rivaroxaban, along with predictors of its use over standard oral therapy, VKA. Prescription of rivaroxaban for the initial and subsequent treatment of VTE was low in the 2- to 9-month period following its approval at our health care center (1.6% and 17.6%, respectively). This suggests that the addition of rivaroxaban on the CHUS drug formulary did not have an immediate impact on prescription patterns. Low-molecular-weight heparin and VKA were most commonly prescribed, a finding similar to a previous study conducted in 2 Canadian tertiary care centers (LMWH followed by a VKA was prescribed in 71% of patients). 22 However, the previous study was conducted before the availability of rivaroxaban. Several factors could explain the limited use of rivaroxaban for VTE treatment. First, the majority of patients in the phase 3 clinical trials performed with rivaroxaban had received at least 1 dose of LMWH, UFH, or fondaparinux before their inclusion in the study (73.0% in EINSTEIN-DVT clinical trial and 92.5% in EINSTEIN-PE clinical trial). 8,9 Therefore, it may be difficult to clearly evaluate the efficacy of rivaroxaban in the initial phase of VTE treatment, particularly in the first hours following the diagnosis. Second, there are few data on the use of rivaroxaban among the population with a higher risk of VTE recurrence, such as patients with cancer and thrombophilia, which represents a small proportion of patients in the EINSTEIN-DVT and EINSTEIN-PE studies. 8,9 Third, data are lacking for patients with a higher risk of bleeding (eg, participants with severe renal impairment), since those were excluded from the pivotal trials. 8,9 Interestingly, the use of rivaroxaban appeared limited to patients with similar characteristics to those included in these trials (relatively young patients with few comorbidities). Finally, the reimbursement of rivaroxaban in patients with a public medication insurance is restricted to patients who cannot receive standard therapy (eg, not possible to monitor international normalized ratio with VKA). 11
Rivaroxaban was prescribed in only a few patients with cancer-associated VTE, which is similar to the proportions included in EINSTEIN-DVT and EINSTEIN-PE studies. 8,9 According to the product monograph, rivaroxaban is neither indicated nor contraindicated in patients with active cancer. 10 Furthermore, the American College of Chest Physicians guidelines recommend the use of LMWH as a first-line therapy in these patients. 4 Therefore, it is possible that rivaroxaban was prescribed as an alternative for individuals with cancer-related VTE who refused to be treated with LMWH because of its injectable form.
The strongest predictor of rivaroxaban use in the treatment of acute VTE was to be younger than 65 years old. In fact, older patients have a higher risk of major bleeding. 15 Deterioration in renal function with aging is a well-known phenomenon 23 and is associated with a greater risk of bleeding due to higher systemic exposure to the drug. Clinical studies with rivaroxaban have revealed that in the elderly patients, the terminal half-life of the drug is longer. 10 This could explain why VKA was more frequently prescribed to older patients. Another factor that could explain the use of rivaroxaban in younger patients is that they are more likely to be covered by a private medication insurance. 24 –26
A second independent predictor of rivaroxaban use was the diagnosis of DVT in the absence of PE. Several hypotheses can explain this result. First of all, DVT is less severe and is associated with a lower mortality rate than PE. 1 Second, rivaroxaban was initially approved for the treatment of DVT, and our study began before its approval for PE. 27,28 However, the number of PE treated with rivaroxaban before and after its approval was analyzed, and no statistical difference was observed. Finally, when we compared the results to the EINSTEIN-DVT and EINSTEIN-PE studies, rivaroxaban was found to be noninferior to standard therapy in both the trials, but the number of recurrent VTE was numerically higher with rivaroxaban in the PE trial, and concerns were raised about the selection of a noninferiority margin of 2.0, which allows a 2-fold increased risk of VTE recurrences between groups. 9,29 Findings from this study might have influenced the use of rivaroxaban in the treatment of PE.
The last independent predictor of rivaroxaban use was the type of hospital stay. Patients who visited the ED only were more likely to receive rivaroxaban. This could be explained, for example, by the fact that a patient with a diagnosis of isolated distal DVT with few symptoms is more likely to be discharged quickly from the ED than a patient admitted with a massive PE and severe dyspnea. Furthermore, it is easier for physicians to prescribe rivaroxaban in patients who have a short length of hospital stay, since there is no need to overlap with a parenteral anticoagulant.
To our knowledge, this is the first study to evaluate predictors of rivaroxaban choice over standard oral therapy in patients with VTE. However, there are several limitations. First, because of its cross-sectional design, data of interest were not always available or were not systematically documented, for example, data on the history of minor bleeding episodes. This may have introduced a nondifferential misclassification bias. Second, important potential predictors of choice such as the physician’s characteristics could not be collected. Third, we evaluated the use of anticoagulants 2 months following the introduction of rivaroxaban in our institution for the treatment of VTE and for a period of 7 months only. This represents a short period to observe significant changes in prescribing patterns, and it could explain our findings on the limited use of rivaroxaban. Finally, the generalizability of this study is limited, since it was conducted in only 1 tertiary care center and most patients included were hospitalized for a diagnosis of PE.
Conclusion
Low-molecular-weight heparin and VKA are mostly prescribed for the treatment of acute VTE even after the approval of a new treatment option for this indication. In real clinical practice, age <65 years, a diagnosis of DVT alone, and an ED visit without hospitalization are associated with the prescription of rivaroxaban rather than VKA for the subsequent treatment of VTE. Our findings suggest that physicians prescribe rivaroxaban according to current recommendations but in a conservative manner, and they seem to limit its use to younger patients with few comorbidities and less severe VTE disease. Finally, this study should be repeated in the future in order to follow the evolution on the use of rivaroxaban in real clinical practice.
Footnotes
Acknowledgments
The authors acknowledge the contributions of Katy Lavoie, Jean-Nicolas Charron, Sarah Bilodeau, Marie-Hélène Guilmain, and Claudie Rodrigue.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Sanofi Canada and Pfizer Canada provided an unrestricted grant for this study. The study sponsors were not involved in the design and conduct of the study; the collection, management, analysis, or interpretation of the data; the writing or the review of the manuscript; or the decision to submit the manuscript for publication.