
Abstract
Thrombolysis and anticoagulation were the main treatment methods for acute pulmonary embolism. However, the use of thrombolysis drugs may lead to bleeding complications. We compared intermittent low-dose urokinase (UK) and alteplase (recombinant tissue plasminogen activator [rt-PA]) in normotensive patients with intermediate-high-risk pulmonary embolism. The UK group was treated with intravenous UK 10 000 U/kg once a day for 7 days. The rt-PA group was given alteplase 50 mg by intravenous injection within 2 hours of admission. After thrombolytic therapy, 48 patients were included in this trial. Compared with before treatment, right and left ventricular diastolic diameter ratio, systolic pulmonary artery pressure, and cardiac troponin I of the 2 groups all significantly decreased 8 and 14 days after treatment, which indicated that right heart function improved. Total efficacy rates for the UK group 8 and 14 days after treatment (79.2%, 87.5%) and the rt-PA group (75.0%, 91.67%) were not significantly different. Adverse bleeding reactions were higher in the rt-PA group (20.8%) than in the UK group (8.3%). This pilot study indicates that intermittent low-dose UK thrombolysis is equally effective as rt-PA. However, future large-scale studies must also determine whether small doses of UK thrombolysis reduce the risk of bleeding.
Introduction
Pulmonary embolism (PE) has increasing rates of incidence and prevalence, and the diagnosis is missed easily. 1,2 Although the 30-day mortality rate of acute PE has been declining, approximately 10% of patients with acute PE die within 3 months after the diagnosis, usually as a result of unstable hemodynamics. 3,4 Based on clinical severity, echocardiography, computed tomography pulmonary angiography (CTPA), and biomarkers, the 2014 European Society of Cardiology (ESC) guidelines 5 divided PE into 3 groups: high risk, intermediate risk, and low risk. The intermediate-risk group was divided into intermediate-high-risk and intermediate-low-risk group. The intermediate-high-risk group usually has right ventricular (RV) dysfunction and elevated circulating levels of biomarkers of myocardial injury.
Anticoagulation therapy is recommended in the guidelines for patients with intermediate-low and low-risk PE, and emergency thrombolysis is recommended for high-risk or massive PE, in order to stabilize hemodynamics and reduce early mortality. 5 –7 However, there remains controversy about the treatment of acute intermediate-high-risk PE. 8
Thrombolytic therapy can reduce all-cause mortality in patients with intermediate-high-risk PE, 9 but the rate of hemorrhage is high, especially in elderly patients. 10,11 Systemic thrombolysis has not been routinely recommended as a primary treatment for patients with intermediate-high-risk PE. However, if during the process of anticoagulation hemodynamic instability occurs, rescue thrombolysis may be considered. Thrombolytic therapy in patients with intermediate-high-risk PE can reduce the short-term mortality rate. 12 The incidence of chronic thromboembolic pulmonary hypertension was increased in the later stage of anticoagulant therapy. 8
The commonly used thrombolytic drugs include urokinase (UK) and recombinant tissue plasminogen activator (rt-PA, such as alteplase). 13 However, the use of these 2 drugs may lead to bleeding complications. One report showed that the risk of cerebral hemorrhage with rt-PA was higher than with UK (1.6% vs 0.5%). 14 Initially, evidence indicated low-dose streptokinase for PE was suitable when standard thrombolytic regimens were contraindicated and could serve as an alternative to the standard dosage. 15,16 In another report, low-dose UK (1000 U/kg/h) was used to treat PE in patients with a history of recent surgery and recent bleeding duodenal ulcers. Consequently, the cardiac index returned to normal after 48 hours of treatment, and systemic arterial pressure gradually stabilized. No major bleeding was observed. It has also been reported that low-dose UK can be used to treat submassive PE via the immediate catheter-directed thrombolysis method. 17 This collectively showed that prolonged thrombolysis with low-dose UK could be a suitable alternative approach to therapy in patients with PE. 18
Until now, there has been a lack of prospective studies evaluating the effects of small doses of UK thrombolysis in a real-world population. For this reason, we performed this clinical pilot study to assess intermittent use of small doses of UK thrombolysis for patients with intermediate- to high-risk PE.
Materials and Methods
Study Design and Randomization
A single-center, prospective, randomized, active control comparison trial was conducted in the Department of Respiratory and Critical Care Medicine of First People’s Hospital, Yichang, China. All eligible patients were randomly grouped using a computerized system. Patients in our hospital who met the inclusion criteria were randomly divided into a UK group and an rt-PA group. The trial protocol was written by 3 academic experts and submitted to our trial steering committee for review, revision, and approval. The final trial protocol was approved by the hospital ethics review board and all patients signed informed consent.
Patient Selection
The diagnosis of acute intermediate-high-risk PE was based on the 2014 ESC guidelines. 5 All patients were diagnosed by CTPA. Inclusion criteria were as follows: (1) CTPA demonstrating PE, (2) symptomatic onset less than 14 days prior to admission, (3) echocardiogram demonstrating RV dysfunction or pulmonary hypertension, (4) B-type natriuretic peptide >100 ng/L and cardiac troponin I greater than the upper limit of normal, and (5) age greater than 60 years. Exclusion criteria were as follows: (1) primary heart disease; (2) high-risk PE, implied by the presence of shock and/or hypotension or systolic blood pressure lower by more than 40 mm Hg from a known baseline blood pressure; (3) Pulmonary Embolism Severity Index (PESI) class I–II or simplified PESI of 0 (implying low-risk PE); (4) the use of heparin for more than 72 hours; (5) presence of contraindications to thrombolytic therapy; and (6) other serious organ disease.
Sample Size
Because this is a pilot study, type I error was kept to α = 0.05 and type II error to β = 0.1, and a 20% difference in the response between the 2 treatment methods was considered significant. We here considered the efficacy of alteplase 50 mg for PE to be 89.1%. 19 We set the sample to 50 patients per group and calculated the power at 90%. Eventually, we recruited 48 patients and randomly allocated them to the UK group and the rt-PA group during the study period. This is a pilot trial presented as preliminary research.
Treatment
All eligible patients were randomly divided into the UK and rt-PA groups by means of a computerized Internet-based system. Respiratory rate, heart rate, blood pressure, and arterial blood gas were monitored in all patients after admission. All patients were in bed and breathing oxygen using a nasal catheter or mask. The UK group was given UK 10 000 U/kg intravenously in a 2-hour infusion once a day for 7 days. The rt-PA group was given alteplase 50 mg by intravenous injection within 2 hours of admission. All the patients were treated with low-molecular-weight heparin after end of thrombolytic therapy, and activated partial thromboplastin time and prothrombin time were followed. Warfarin was initiated in all patients and low-molecular-weight heparin was continued while monitoring the international normalized ratio (INR). When INR reached 2 to 3, low-molecular-weight heparin was discontinued and warfarin was used alone for 3 to 6 months.
Follow-Up and Outcome Assessment
All patients were followed up for 30 days and were evaluated for death, hemodynamic decompensation, bleeding, recurrent PE, and other serious adverse events. The same experienced radiologists performed CTPA examinations on all patients before treatment and then also both 8 and 14 days after treatment. Patients were divided into 3 grades (highly effective, moderately effective, and ineffective) according to the improvement of clinical symptoms and the change of lung lesion area. Highly effective: Clinical symptoms disappeared or were significantly relieved, and CTPA showed pulmonary defect area reduced more than 75%. Moderately effective: The clinical symptoms were alleviated, and CTPA showed pulmonary defect area reduced more than 25%, but less than 75%. Ineffective: Clinical symptoms aggravated during follow-up or death, and CTPA showed pulmonary defect area was reduced by less than 25%, unchanged, or extended.

Safety outcomes were assessed based on bleeding caused by thrombolysis within 8 days and serious adverse events within 30 days. In addition, all patients’ RV function was evaluated by echocardiography on the 8th and 14th day after treatment. In order to reduce the measurement error, all the patients were evaluated by the same experienced ultrasonic doctor. Right ventricular diastolic diameter/left ventricular (LV) diameter and systolic pulmonary artery pressure (SPA) were measured. Troponin I and
Statistical Analyses
Statistical analyses were performed using the SPSS 19.0 (SPSS Inc, Chicago, Illinois). Continuous variables were expressed as mean (standard deviation), whereas categorical variables were given as numbers (percentages). Repeated-measures analysis of variance was used to compare the measurement data before and after treatment. Categorical variables were compared by χ2 or Fisher exact test. P < .05 was considered statistically significant.
Result
Study Selection and Characteristics
From October 2014 to December 2016, 106 hospitalized patients were screened. Excluded from the study were 9 patients with high PE, 29 patients with intermediate-low-risk PE and low-risk PE, 16 patients with serious organ disease (cerebral hemorrhage, major surgery, digestive tract hemorrhage, renal insufficiency), and 4 patients who declined to participate in this trial. A total of 48 patients with intermediate-high-risk PE were available for the study and signed informed consent. Of these patients, 24 were randomly assigned to the UK group and 24 assigned to the rt-PA group. Demographic data, clinical status, and medical history were well matched between the 2 treatment groups (Table 1). Mean age of patients (n = 24) who received thrombolysis with UK was 69.5 (3.7) years, which was comparable with the age in the rt-PA group of 71.4 (4.1) years. All patients were normotensive, with mean systolic pressure in UK group being 130 (16) mm Hg, while in the rt-PA group, it was 130 (17) mm Hg. Smoking was the most common risk factor for PE and present in 33.3% (n = 16) of all the patients, followed by recent history of hypertension in 22.9% (n = 11), diabetes mellitus in 10.4% (n = 5), coronary heart disease in 12.5% (n = 6), and chronic pulmonary disease in 10.4% (n = 5) of patients. These risk factors were not significantly different between groups.
Characteristics of the Patients at Baseline.
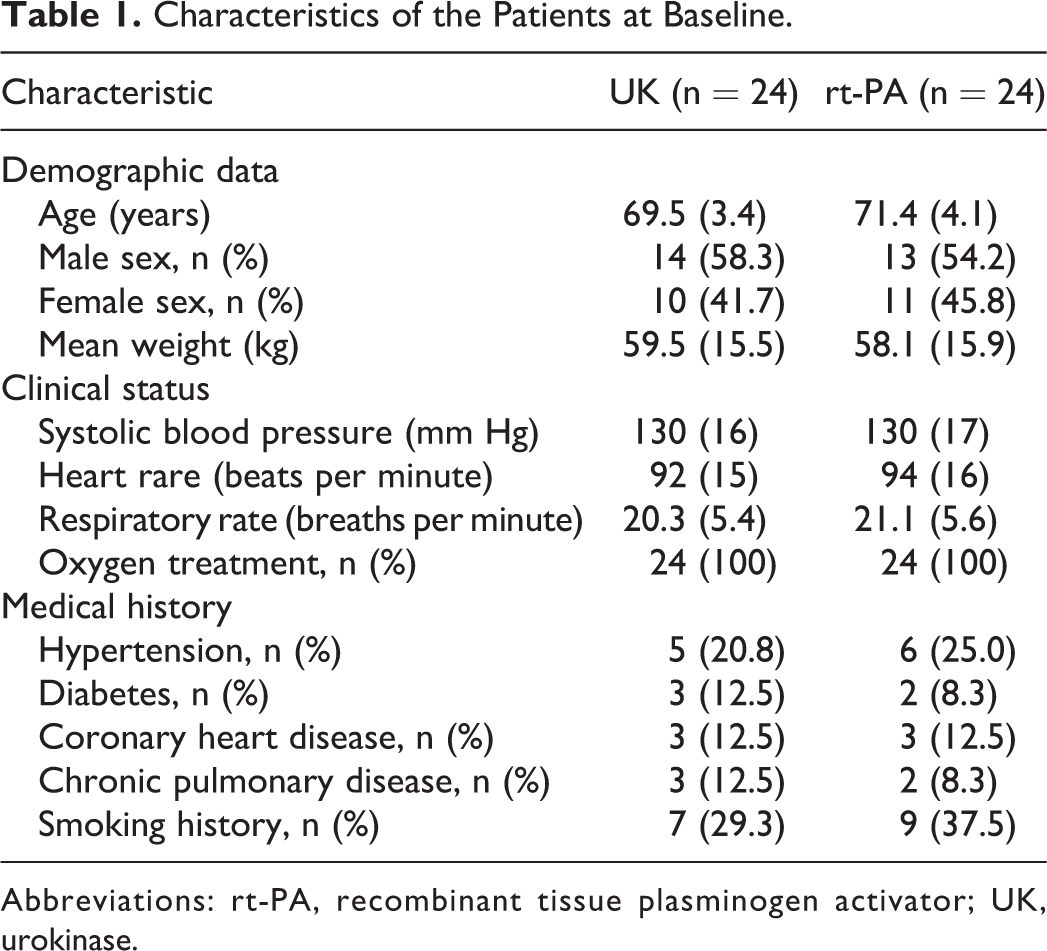
Abbreviations: rt-PA, recombinant tissue plasminogen activator; UK, urokinase.
Efficacy Outcomes
Between randomization and 30 days, as a result, patients with death and hemodynamic collapse were not found. We further evaluated the therapeutic effects by comparing echocardiography, CTPA, and serum enzyme assessments of myocardial injury before and after treatment.
Echocardiography
All patients underwent echocardiography at baseline and at 8 and 14 days after admission. The RV/LV end-diastolic dimension ratio was similar in the 2 treatment groups at baseline (1.01 [0.06] and 1.03 [0.05] in UK and rt-PA groups, respectively). Systolic pulmonary arterial pressure at baseline was also similar in the 2 groups. At 8 and 14 days after initiation of thrombolysis, both RV/LV and SPA significantly decreased compared with baseline levels in both groups (Table 2).
Comparison of Right Ventricular Function.a
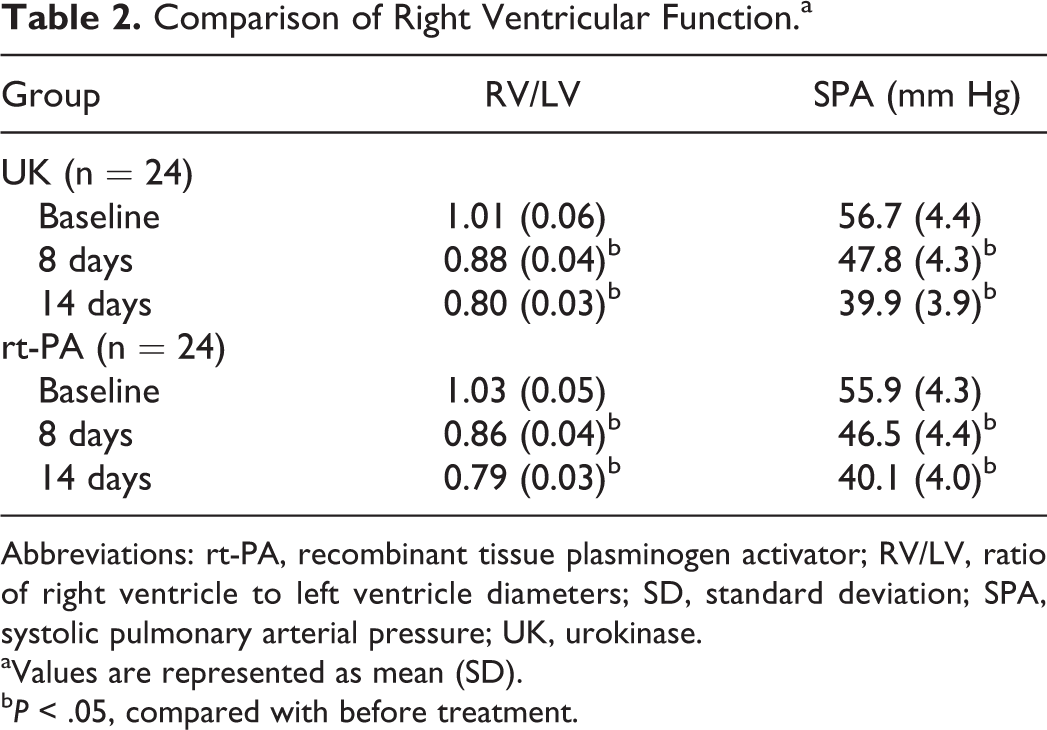
Abbreviations: rt-PA, recombinant tissue plasminogen activator; RV/LV, ratio of right ventricle to left ventricle diameters; SD, standard deviation; SPA, systolic pulmonary arterial pressure; UK, urokinase.
aValues are represented as mean (SD).
b P < .05, compared with before treatment.
Computed tomography pulmonary angiography
Definitive diagnosis of PE was established by CTPA. The effect of thrombolysis was evaluated by 2 subsequent CT examinations in all participants. At 8 days after treatment, the total efficacy rates for the UK and rt-PA groups were 19 (79.2%) and 18 (75.0%), respectively (P = .5). By 14 days, the total efficacy rates of the 2 groups increased (87.5% and 91.7% in the UK and rt-PA groups, respectively, P = .5; Table 3). There were no significant differences between the groups evidenced by this assessment of thrombolytic efficacy.
Comparison of Thrombolytic Effect.a
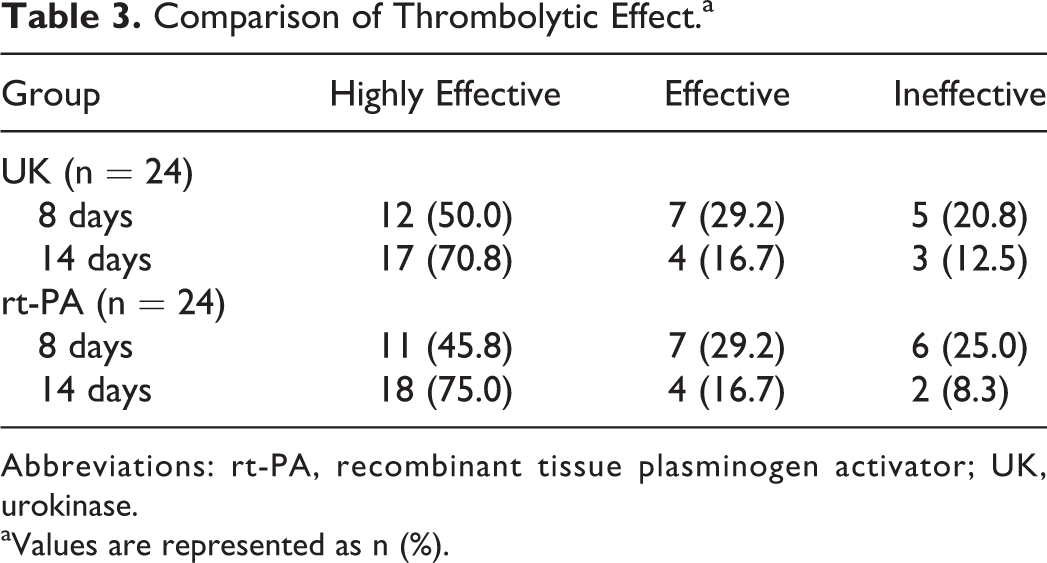
Abbreviations: rt-PA, recombinant tissue plasminogen activator; UK, urokinase.
aValues are represented as n (%).
Biochemical indicators
Patients with acute intermediate-high-risk PE often have elevated troponin I and
Comparisons of Biochemical Indices.a
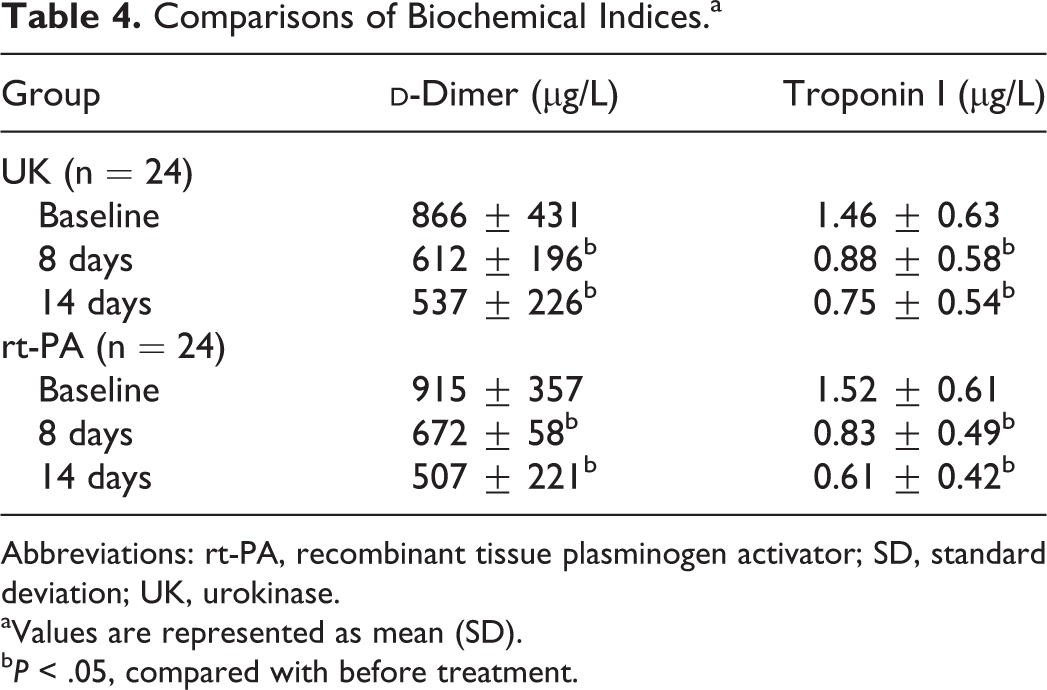
Abbreviations: rt-PA, recombinant tissue plasminogen activator; SD, standard deviation; UK, urokinase.
aValues are represented as mean (SD).
b P < .05, compared with before treatment.
Safety Outcomes
Safety was assessed in accordance with the criteria of the International Society on Thrombosis and Haemostasis. 20 Intracranial bleeding occurred in 1 (4.1%) patient in the rt-PA group, but not in the UK group. Minor bleeding tended to occur more in the rt-PA group than in the UK group (n = 4; 16.7% vs n = 2; 8.3%), although this was not statistically significant (P = .41).
Discussion
Patients with intermediate-high-risk PE, with RV dysfunction or injury to the myocardium, may have an elevated risk of early death or major complications, even while measured hemodynamics are stable. 21 –23 Thrombolytic therapy can dissolve intravascular thrombosis rapidly, relieve pulmonary arterial pressure, and improve the dysfunction of right heart. 24
The latest guidelines suggest that we should attempt to cure the patients with acute intermediate-high-risk PE by anticoagulant therapy, but if hemodynamics become unstable, then thrombolytic therapy should be considered as a rescue treatment method. Research demonstrates that both therapeutic pathways can improve patients’ clinical symptoms, but thrombolysis is able to remarkably decrease the mortality of patients with high risk and intermediate-high-risk PE. Konstantinides et al 9 found that, when compared to simple anticoagulant therapy, thrombolytic therapy combined with anticoagulant therapy can reduce the right heart load in elderly patients with submassive PE, restore lung tissue effective blood supply, prevent disease progression, and ultimately reduce the mortality of PE. Berghaus et al 25 found that the hospitalization time of patients with PE was closely related to the patient age and complications. Effective thrombolytic therapy can shorten the median hospital stay. Fasullo and his colleagues 26 discovered that compared with the simple anticoagulation therapy, thrombolysis combined with anticoagulant therapy can significantly improve the RV diameter and pulmonary artery pressure. Furthermore, during the hospital stay and 6-month follow-up, the incidence of adverse events was significantly lower than those in simple coagulation therapy. However, the excess bleeding after thrombolysis was higher than from anticoagulation alone. Marti et al 11 performed a meta-analysis of 12 randomized controlled studies and found that 96 (9.9%) of the 974 patients who received thrombolysis had bleeding complications, compared to only 3.6% in the anticoagulation group. Intracranial hemorrhage or fatal bleeding occurred with thrombolysis in up to 1.7%, which was significantly higher than patients treated with simple anticoagulation, in which 0.3% were so afflicted. In a randomized, controlled, double-blind trial, 13 1005 patients with intermediate-risk PE with RV dysfunction were enrolled who had elevated troponin I or T levels. Five hundred six patients were treated with alteplase combined with anticoagulant therapy, and 499 patients were treated with placebo plus anticoagulation. The results showed that the incidence of bleeding, death, or hemodynamic deterioration in patients treated with thrombolytic therapy (2.6%) was lower than in the placebo group (5.6%). However, the incidence of extracranial bleeding significantly increased in the thrombolytic group (6.3%) compared with the placebo group (1.2%). The number of hemorrhagic strokes in the thrombolysis group (2.4%) was higher than that in the placebo group (0.2%). In the majority of patients with bleeding, adverse reactions occurred in patients over the age of 75. Overall, it appears that thrombolysis combined with anticoagulant therapy is generally more effective than anticoagulant therapy alone and can be considered in patients with moderate and high-risk acute PE. However, the incidence of bleeding with thrombolysis is high. In order to solve this problem, some scholars have reduced the dosage of drugs in the treatment of patients with acute PE 27 and have reported good results.
Treatment of PE with ultrasound-assisted catheter thrombolysis can reduce the dosage of thrombolytic agents and reduce the adverse effects of bleeding. 28 In this study, we used intermittent intravenous low-dose UK in the treatment of acute intermediate-high-risk PE, which we assessed to determine whether there was risk reduction while still ensuring effective thrombolytic therapy.
For elderly patients with acute intermediate-high-risk PE, our study found that there was no significant difference in efficacy outcome variables between the UK-treated group (provided in intermittent [daily] treatment over 7 days) and the rt-PA group treated with conventional 2-hour thrombolysis. However, 1 patient in the rt-PA group had an intracranial hemorrhage. Bleeding in the UK group occurred only in the puncture site. In the rt-PA group, the incidence of adverse events of bleeding (20.8%) trended higher than that in the UK group (8.33%), without this reaching statistical difference.
For patients with PE who have recently undergone surgery and have bleeding risk, a small dose of UK thrombolysis was a treatment option. 16,18 It has also been reported that small doses of UK combined with low-molecular-weight heparin could be used to treat patients with higher risk of bleeding in patients with deep vein thrombosis. 29
This study has some limitations, mainly the small sample size, that should be acknowledged. Furthermore, UK was administered for 7 days, whereas rt-PA was administered only once, immediately after hospital admission. This led to the failure to adopt double-blind methods and may have introduced performance bias. In addition, in the rt-PA group, the incidence of adverse events of bleeding (20.8%) trended higher than in the UK group (8.33%), but this difference did not reach statistical significance, possibly because of the small sample size. Future large-scale studies are needed to determine whether small doses of UK thrombolysis reduce the risk of bleeding.
Conclusions
According to the results of this study, for elderly patients with acute intermediate-high-risk PE, either intermittent-low-dose UK or alteplase thrombolytic treatment is effective, but patients treated with intermittent-low-dose of UK thrombolysis may have less bleeding risk.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The scientific research program of Hubei Provincial Department of Education (D20171201), Research Fund for Excellent Dissertation of China Three Gorges University (2017YPY060), National Science Foundation of China grant (81200052).