
Abstract
The effect of anticoagulation by heparin on patients with non-ST elevation acute coronary syndrome (NSTE-ACS), receiving early dual antiplatelet therapy, has not been fully evaluated. We classified 355 patients with NSTE-ACS according to the adequacy of anticoagulation (percentage of low activated partial thromboplastin time [APTT] level). The 6-hour APTT level was optimal in only 23.1% of the patients treated with unfractionated heparin. The rate of poor preprocedural coronary blood flow (thrombolysis in myocardial infarction grade <3, 39.1%, 30.5%, 30.3%, and 33.9% in the 100% low-, 99%∼50% low-, 49%∼1% low-, and 0% low-APTT group, respectively, P = .632) and bleeding events did not differ between the groups. Instead, in multivariate analysis, the diagnosis of myocardial infarction was the only independent predictor of poor coronary flow. For bleeding events, the usage of glycoprotein IIb/IIIa inhibitor appeared to be a sole risk factor. In conclusion, inadequate preprocedural anticoagulation was not associated with adverse outcomes in patients with NSTE-ACS treated with dual antiplatelet agents.
Introduction
Initiation of anticoagulant therapy is recommended as soon as possible in patients with non-ST elevation acute coronary syndrome (NSTE-ACS) who are scheduled for percutaneous coronary intervention (PCI). 1 Various trials have shown that anticoagulants combined with antiplatelet therapy reduce fatal and nonfatal cardiovascular outcomes. 2 Currently, 2 different anticoagulants are widely used—unfractionated heparin (UFH) and low-molecular-weight heparin (LMWH). Both agents have strong recommendations for usage; when UFH is given, serial monitoring of the activated partial thromboplastin time (APTT) is needed to be determined to achieve therapeutic range. 3,4 Although the need for monitoring may complicate therapy for both the patient and the medical team, UFH is used over other agents because of its short biological half-life, relatively low cost, and availability of a neutralizing agent.
Due to the predetermined therapeutic range of UFH, previous studies have evaluated the effects of inadequate anticoagulation on ischemic or hemorrhagic complications of NSTE-ACS. 5 –8 However, these trials were conducted before the current treatment protocols including the use of early dual antiplatelet therapy, adjunctive medications such as glycoprotein IIb/IIIa inhibitors, and drug-eluting stents.
In this study, we examined the adequacy of anticoagulation and the effect of inadequate anticoagulation in patients with NSTE-ACS who were treated with early dual antiplatelet agents and PCI.
Methods
Study Population
Patients diagnosed with non-ST segment elevation myocardial infarction (MI) or unstable angina among those who visited Seoul National University Bundang Hospital emergency department from January 2007 to January 2011 and treated with PCI were enrolled in this study. Patients who were administered anticoagulants other than UFH or enoxaparin and patients with no APTT monitoring despite the use of UFH were excluded. Also, patients allergic to antiplatelet drugs, UFH, enoxaparin, metal alloys, or contrast agents, with a planned surgery within 1 month of PCI or planned thrombolysis, pregnant, age <18 or >95 years, with angina not due to coronary disease, or with a life expectancy <1 months were excluded. The study protocol was approved by the ethics committee at Seoul National University Bundang Hospital and was conducted according to the principles of the Declaration of Helsinki.
The diagnosis of unstable angina was based on symptoms of angina that were worsening or occurred with minimal activity and associated with either current electrocardiographic evidence of ischemia or previously documented objective evidence of a coronary artery disease. 1 Non-ST elevation MI was defined as the presence of diagnostic criteria of unstable angina plus detection of a rise and/or fall in cardiac biomarker values (preferably cardiac troponin). 9
To compare the adequacy of anticoagulation by UFH, the patients were categorized, according to the anticoagulant administered, and the follow-up APTT value obtained every 6 hours until PCI was performed. Patients given UFH were divided into 4 groups, according to the percentage of low APTT levels during the entire time period of APTT follow-up prior to PCI, those with 100% low, 99% ∼ 50% low, 49% ∼ 1% low, and 0% low APTT levels. Low APTT was defined as any APTT level lower than the therapeutic range. The LMWH group consisted of patients given enoxaparin.
Percutaneous Coronary Intervention Procedure
All patients received a loading dose of aspirin 300 mg and clopidogrel 300 mg upon arrival to the emergency department unless previously prescribed and an additional 300 mg of clopidogrel in the cardiac catheterization laboratory just before PCI. Clopidogrel 75 mg/d was recommended for at least 1 year with lifelong aspirin 100 mg/d. Other medications such as beta-blockers or nitrates were administered at the discretion of the attending physician.
The PCI was performed by standard techniques. As soon as the guiding catheter was engaged, the activated clotting time (ACT) of each patients was checked, and the loading dose of UFH was administered according to the ACT results (ACT < 150 seconds: heparin 100 U/kg, ACT ≤ 150 to < 200: heparin 70 U/kg, ACT ≤ 200 to < 300 seconds: heparin 50 U/kg, and ACT ≥ 300 seconds: no heparin given). If administration of glycoprotein IIb/IIIa inhibitors was planned, the heparin dose was adjusted (ACT < 150 seconds: heparin 70 U/kg, ACT ≤ 150 to < 200: heparin 50 U/kg, and ACT ≥200 seconds: no heparin given). After the initial dose, heparin was administered during the procedure to maintain an ACT > 250 seconds. Target lesions were predilated with a plain balloon followed by stent implantation and poststenting dilation if necessary. Thrombus aspiration catheter and glycoprotein IIb/IIIa inhibitors were used at the operators’ discretion. Following the intervention, cardiac enzymes including creatinine kinase, creatinine kinase MB (CK-MB), and cardiac troponin-I were obtained every 6 hours for 24 hours and then daily until within normal limits. All patients were clinically followed up for 30 days after PCI.
Activated Partial Thromboplastin Time Monitoring and Heparin Infusion Adjustment
The initial dose of UFH was an intravenous bolus of 60 U/kg (maximum of 4000 units) and an initial infusion of 12 U/kg/h (maximum of 1000 units/h). The target therapeutic range was an APTT ratio of 1.5 to 2.0 times the control. 10 The APTT was determined 6 hours after the initiation of UFH; if the results were within the therapeutic range, the infusion rate was left unchanged, and the APTT was measured after 6 hours. In patients whose APTT results were not within the therapeutic range, the infusion was adjusted according to a standard heparin nomogram (Table 1), and the APTT was measured 6 hours later. The UFH and LMWH were discontinued 6 hours and 12 hours prior to coronary angiography (CAG), respectively.
Unfractionated Heparin Dose Adjustment Nomogram of the Study Institution.
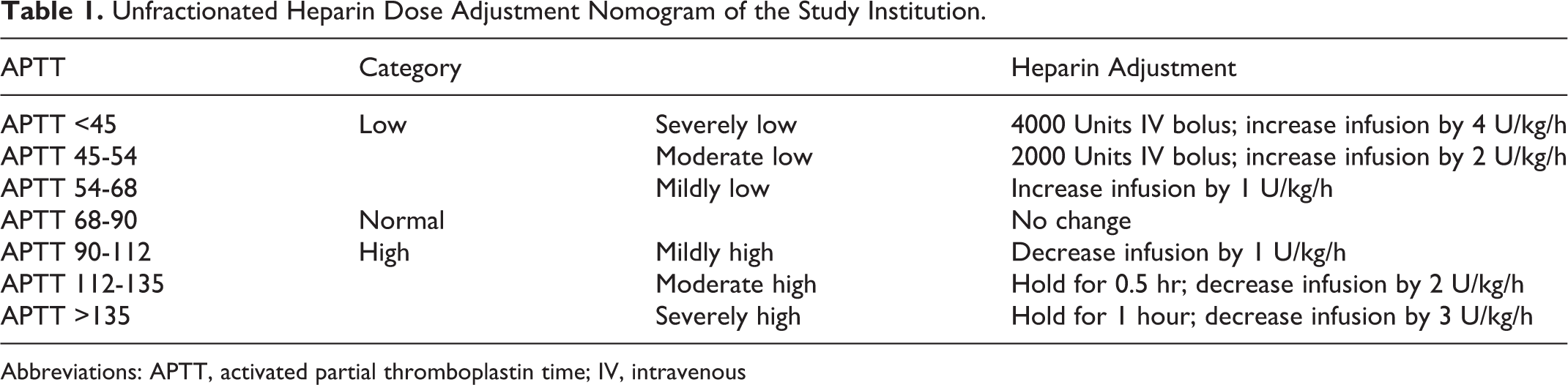
Abbreviations: APTT, activated partial thromboplastin time; IV, intravenous
Study End Points and Definitions
The primary end point was preprocedural coronary flow of the culprit artery graded by thrombolysis in myocardial infarction (TIMI) flow grade classification. The secondary end points were the presence of a visible thrombus at the initial CAG, periprocedural MI, major adverse cardiovascular events (MACEs), the composite of cardiac death, nonfatal MI, and target vessel revascularization at 30 days. Preprocedural TIMI flow and the presence of visible thrombus at the initial CAG were analyzed by 2 experienced angiography analysts who were blinded to all clinical data, presentation, and outcomes. In a situation of disagreement, the 2 analysts reviewed the angiographic data, and a final decision was established by consensus. Periprocedural MI was evaluated using trends in cardiac enzymes, specifically cardiac troponin-I. As defined previously, 9 when pre-PCI cardiac troponin-I was normal, elevation of biomarkers more than 5 times the 99th percentile upper reference limit (URL) after PCI was indicative of a periprocedural MI. When cardiac troponin-I was elevated but decreasing, recurrent infarction after PCI was diagnosed if there was a ≥20% increase in the value of the post-PCI sample. Patients with elevated cardiac troponin-I were not included in periprocedural MI analysis. For MACEs, all deaths were considered cardiac unless a noncardiac cause could be identified. The diagnosis of MI was based on the presence of new Q waves in at least 2 contiguous leads or an elevation of cardiac troponin-I above the URL. Periprocedural MI determined by cardiac enzyme was not included in MACE. For target vessel revascularization, all PCIs or coronary artery bypass graft (CABG) surgeries occurring after the baseline procedure were included. 11
The safety analysis end point was defined as clinically proven bleeding events. Bleeding events were classified using the Bleeding Academic Research Consortium (BARC) definitions. 12 Briefly, BARC type 1 includes bleeding events that are not actionable, type 2 includes events with any overt sign of hemorrhage that does not meet criteria for other types, type 3 includes intracranial or intraocular hemorrhage and overt bleeding plus hemoglobin drop, type 4 includes CABG-related bleeding events, and type 5 includes fatal bleeding events.
Statistical Analysis
Data are presented as numbers and frequencies for categorical variables and as mean ± standard deviation for continuous variables. To compare the groups, the chi-square test (or the Fisher exact test when any expected cell count was <5 for a 2 × 2 table) was used for categorical variables, and the unpaired Student t test or 1-way analysis of variance was applied for continuous variables. The individual level of significance in each group of comparisons was determined using the Bonferroni correction for multiple comparisons. A multiple logistic regression analysis was performed to identify variables influencing the primary outcome. The covariates included in multivariate analyses were selected if they were known to have predictive values or had significant effects (P < .10) on the outcomes in univariate analyses. The final model was determined by stepwise procedure, and the Hosmer-Lemeshow goodness-of-fit test was used to evaluate model calibration. All statistical tests were 2-tailed. A 2-sided probability value of less than .05 was considered statistically significant. Statistical tests were performed using SPSS, version 18 (SPSS Inc, Chicago, Illinois).
Results
Adequacy of Anticoagulation
Among the 520 patients diagnosed with NSTE-ACS, 291 (56.0%) patients presented with non-ST elevation MI and 229 (44.0%) patients presented with unstable angina. In all, 24 patients were given UFH without APTT monitoring and 79 patients who underwent CAG before administering heparin were excluded, leaving 417 patients who were grouped based on the anticoagulant administered and the adequacy of anticoagulation. A total of 355 patients received UFH and 62 patients received LMWH. Among the patients who received UFH, the mean number of APTT follow-up was 2.8 ± 3.1 (interquartile range 1.0-3.0). Out of these patients, 23.1% (82 of 355) achieved the prespecified optimal anticoagulation level at the 6-hour APTT follow-up, whereas 34.6% (123 of 355) had a low 6-hour APTT and 42.3% (150 of 355) had a high 6-hour APTT. At the 12-hour APTT follow-up, 32.5% (81of 249) and at the 18-hour APTT follow-up, 25.5% (39 of 153) had reached the optimal APTT (Figure 1). There was no significant difference in the rate of optimal APTT at the 6-hour and 12-hour follow-up (P = .870). Among the 82 patients who had an optimal 6-hour APTT, 53.3% (32 of 82) changed to a low APTT, 15.0% (9 of 82) to a high APTT, and only 31.7% (19 of 82) remained optimal (Figure 2). As more patients underwent angiography and PCI over time during heparin administration, the number of patients with follow-up APTT levels became less as time passed.
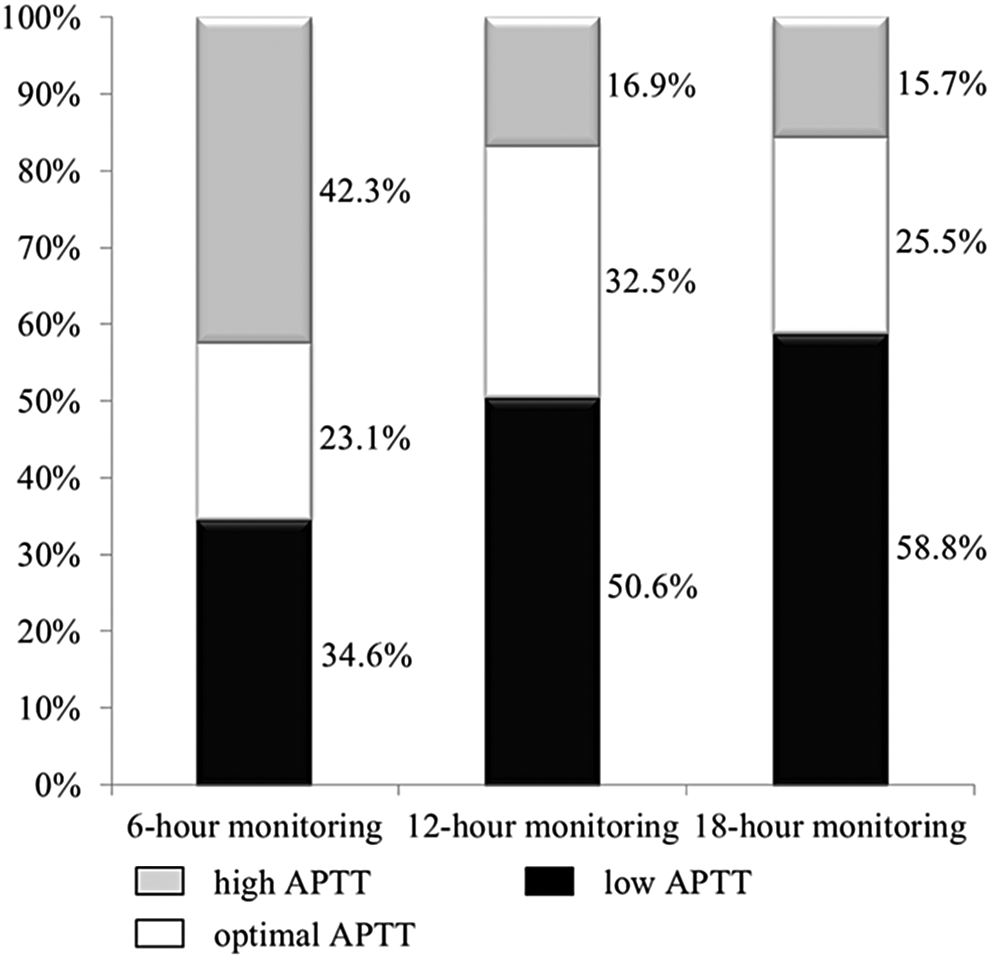
Proportion of patients with low, optimal, and high APTT levels at 6-hour, 12-hour, and 18-hour monitoring. APTT indicates activated partial thromboplastin time.
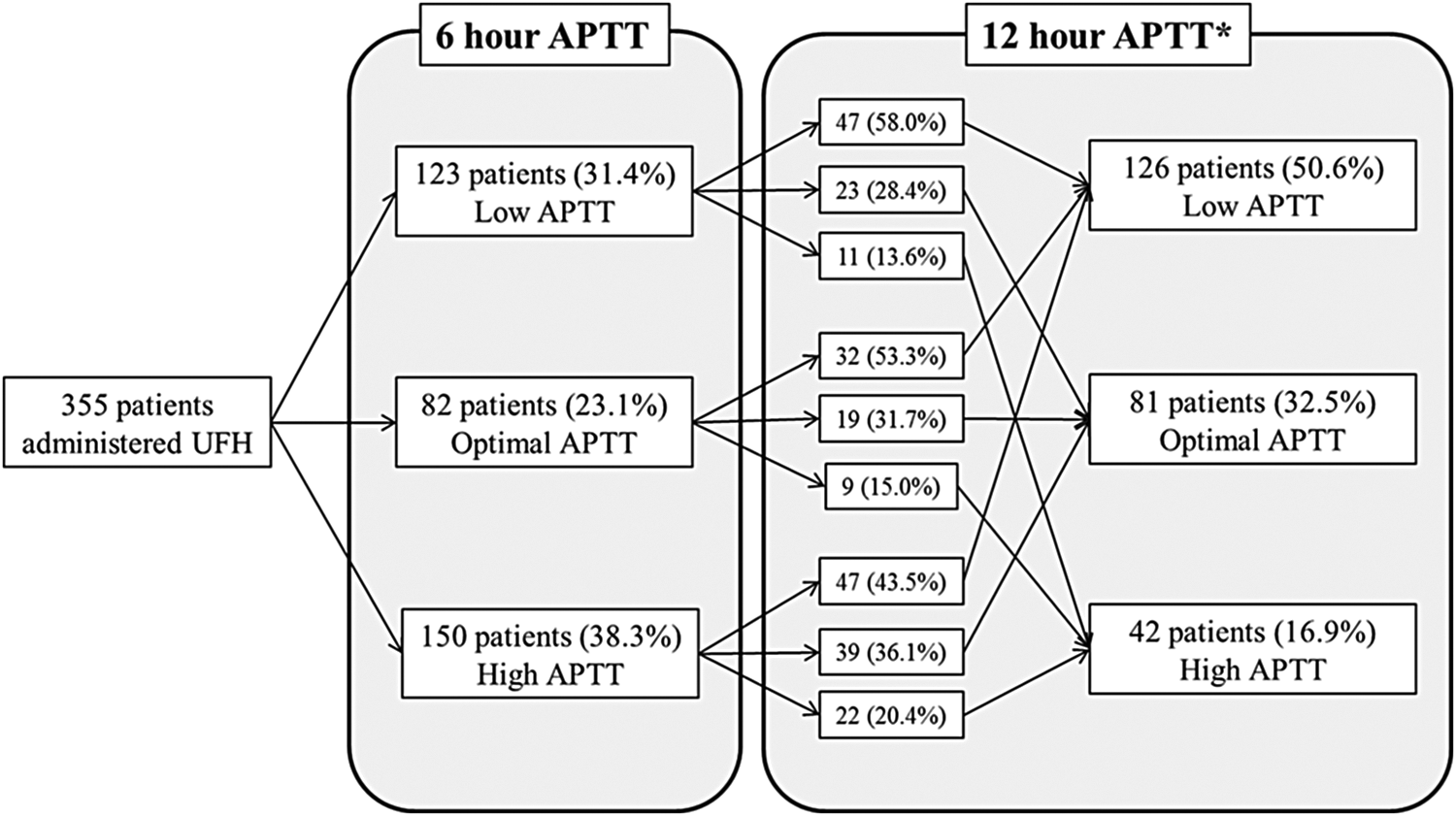
Change in APTT at the second APTT monitoring, for patients who had low, optimal, and high APTT at the 6-hour monitoring. APTT indicates activated partial thromboplastin time. *Of the 355 patients, 106 patients underwent PCI after the 6-hour APTT, leaving 249 patients in whom the 12-hour APTT was checked.
To find out predicting factors associated with a low 6-hour APTT, baseline characteristics were compared according to the 6-hour APTT. Patients with a low 6-hour APTT were likely to be younger, current smokers, have a lower TIMI score, and poor lipid profile (Table 2). A multivariate logistic regression analysis was done on variables with a P value < .1 on univariate analysis and basic demographic variables to estimate independent predictors of subtherapeutic anticoagulation; variables were age, sex, height, clinical diagnosis, current smoking, TIMI score, cholesterol level, and the initial CK-MB level. Only smoking (hazard ratio [HR] 2.187, 95% confidence interval (CI) 1.075-4.449, P = .031) was associated with a low 6-hour APTT level.
Baseline Characteristics of the Patients With Low, Optimal, and High 6-hour APTT Levels.a
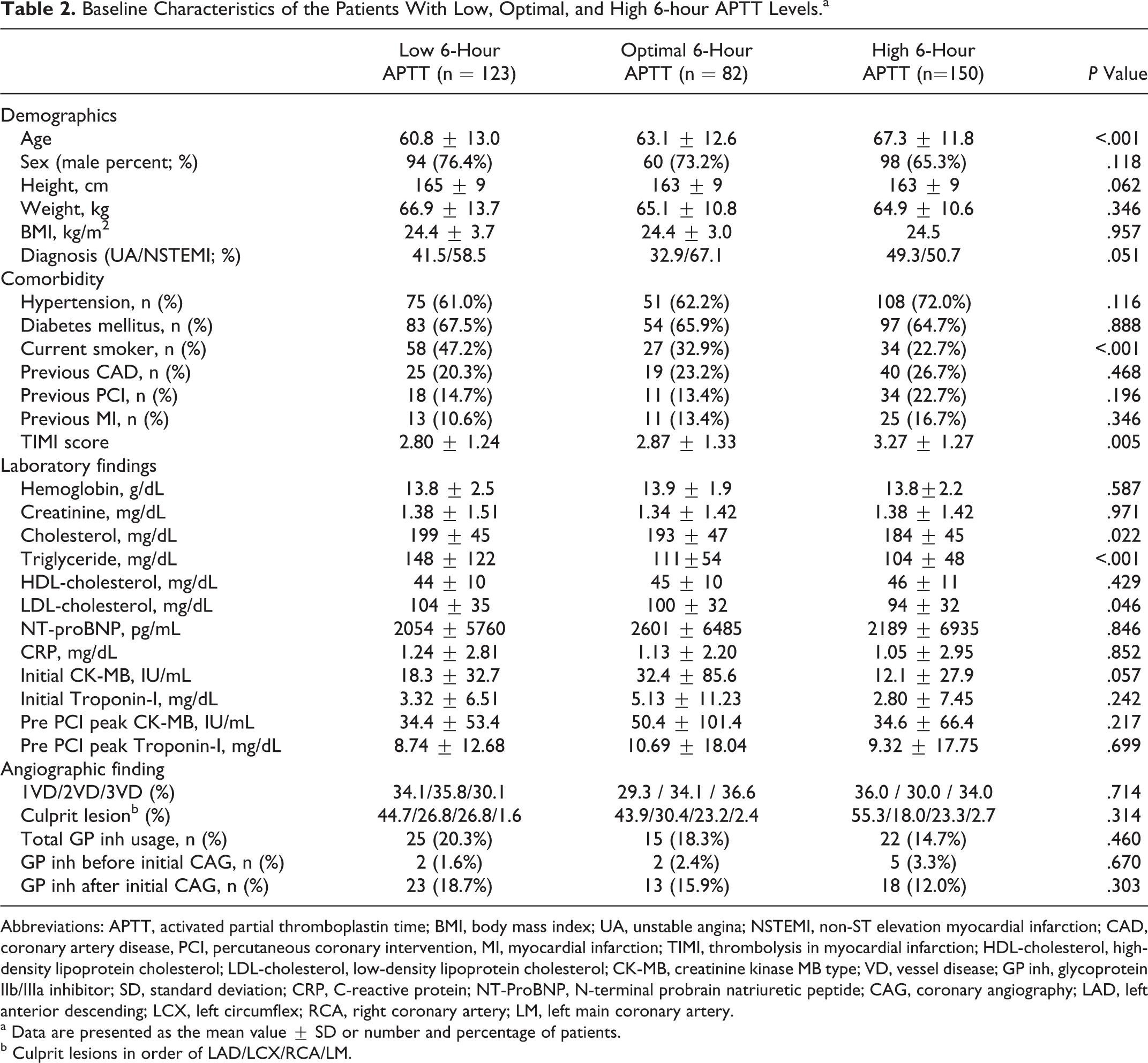
Abbreviations: APTT, activated partial thromboplastin time; BMI, body mass index; UA, unstable angina; NSTEMI, non-ST elevation myocardial infarction; CAD, coronary artery disease, PCI, percutaneous coronary intervention, MI, myocardial infarction; TIMI, thrombolysis in myocardial infarction; HDL-cholesterol, high-density lipoprotein cholesterol; LDL-cholesterol, low-density lipoprotein cholesterol; CK-MB, creatinine kinase MB type; VD, vessel disease; GP inh, glycoprotein IIb/IIIa inhibitor; SD, standard deviation; CRP, C-reactive protein; NT-ProBNP, N-terminal probrain natriuretic peptide; CAG, coronary angiography; LAD, left anterior descending; LCX, left circumflex; RCA, right coronary artery; LM, left main coronary artery.
a Data are presented as the mean value ± SD or number and percentage of patients.
b Culprit lesions in order of LAD/LCX/RCA/LM.
Baseline Characteristics According to Anticoagulation
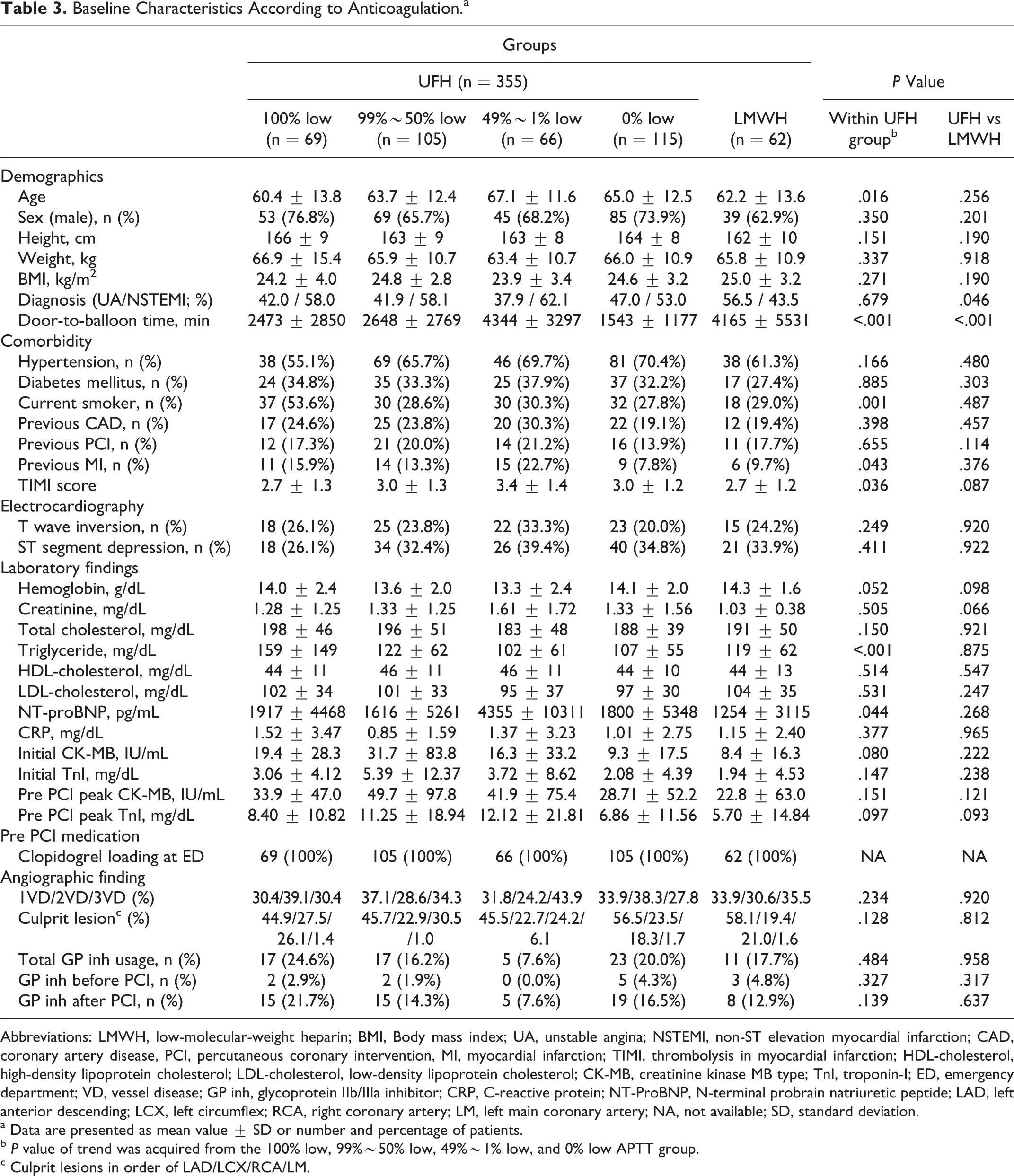
After grouping the study population according to the anticoagulation agent used and the adequacy of anticoagulation during the entire APTT monitoring period, 69 patients were classified as the 100% low APTT group, 105 patients as the 99%∼50% low APTT group, 66 patients as the 49%∼1% low APTT group, and 105 patients as the 0% low APTT group. Sixty-two patients who received enoxaparin were referred to as the LMWH group (Figure 3). Baseline clinical and angiographic characteristics are summarized in Table 3. The mean age, door-to-balloon time, proportion of current smokers, patients with previous MI, the TIMI score, triglyceride level, N-terminal probrain natriuretic peptide level differed between the groups. Comparing the population administered UFH or LMWH, it was found that the clinical diagnosis and door-to-balloon time differed between patients.
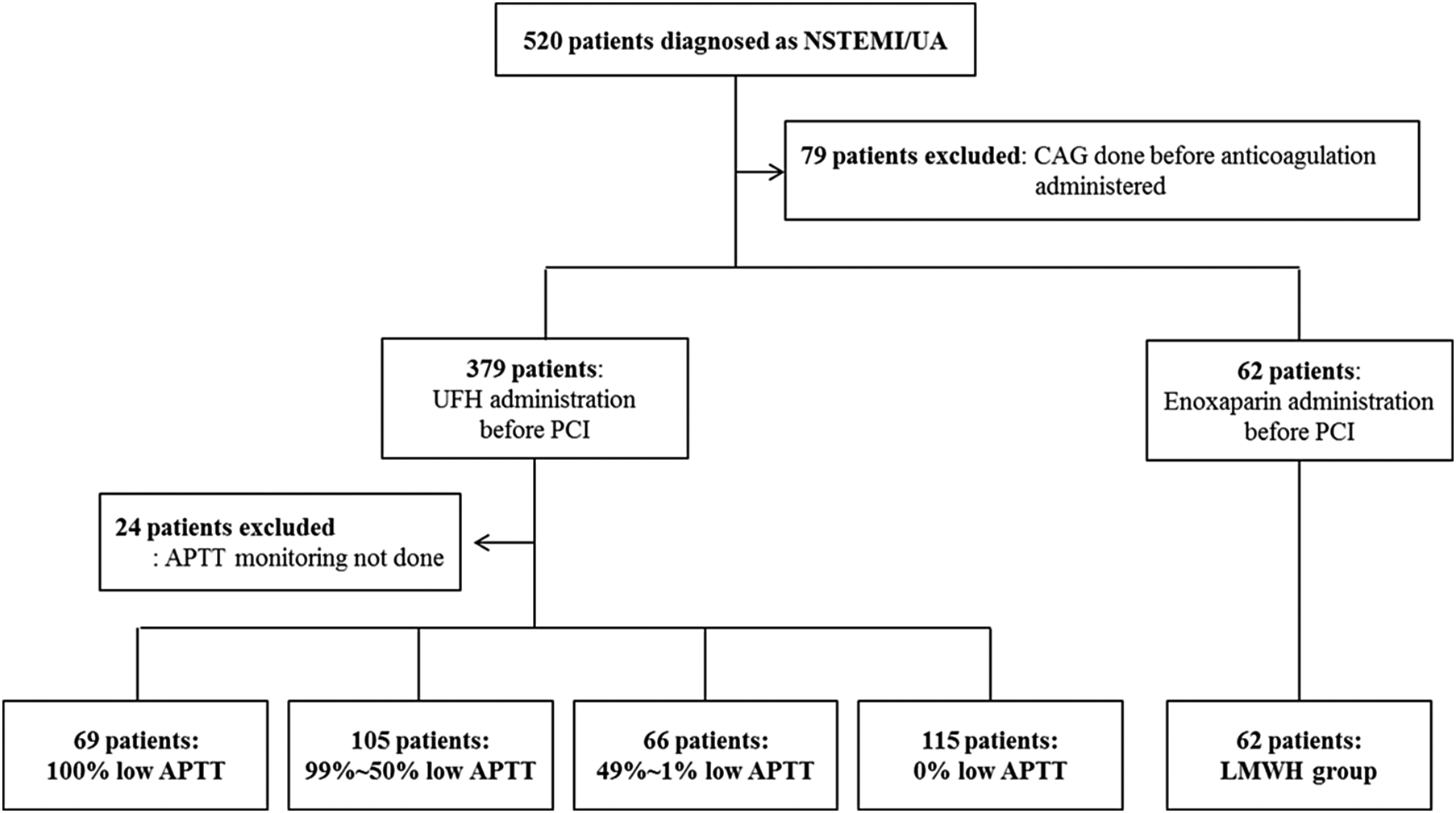
Of the 520 patients enrolled, 79 patients underwent PCI before anticoagulant medication was started. Among the 379 patients who received unfractionated heparin, 355 patients had an APTT level checked and were divided into the 100% low APTT group (69 patients), 99%∼50% low APTT group (105 patients), 49%∼1% low APTT group (66 patients), and the 0% low APTT group (115 patients). Sixty-two patients received LMWH. NSTEMI indicates non-ST segment elevation myocardial infarction; UA, unstable angina; PCI, percutaneous coronary intervention; UFH, unfractionated heparin; APTT, activated partial thromboplastin time; LMWH, low-molecular-weight heparin.
Baseline Characteristics According to Anticoagulation.a
Abbreviations: LMWH, low-molecular-weight heparin; BMI, Body mass index; UA, unstable angina; NSTEMI, non-ST elevation myocardial infarction; CAD, coronary artery disease, PCI, percutaneous coronary intervention, MI, myocardial infarction; TIMI, thrombolysis in myocardial infarction; HDL-cholesterol, high-density lipoprotein cholesterol; LDL-cholesterol, low-density lipoprotein cholesterol; CK-MB, creatinine kinase MB type; TnI, troponin-I; ED, emergency department; VD, vessel disease; GP inh, glycoprotein IIb/IIIa inhibitor; CRP, C-reactive protein; NT-ProBNP, N-terminal probrain natriuretic peptide; LAD, left anterior descending; LCX, left circumflex; RCA, right coronary artery; LM, left main coronary artery; NA, not available; SD, standard deviation.
a Data are presented as mean value ± SD or number and percentage of patients.
b P value of trend was acquired from the 100% low, 99%∼50% low, 49%∼1% low, and 0% low APTT group.
c Culprit lesions in order of LAD/LCX/RCA/LM.
Coronary Blood Flow According to Anticoagulation
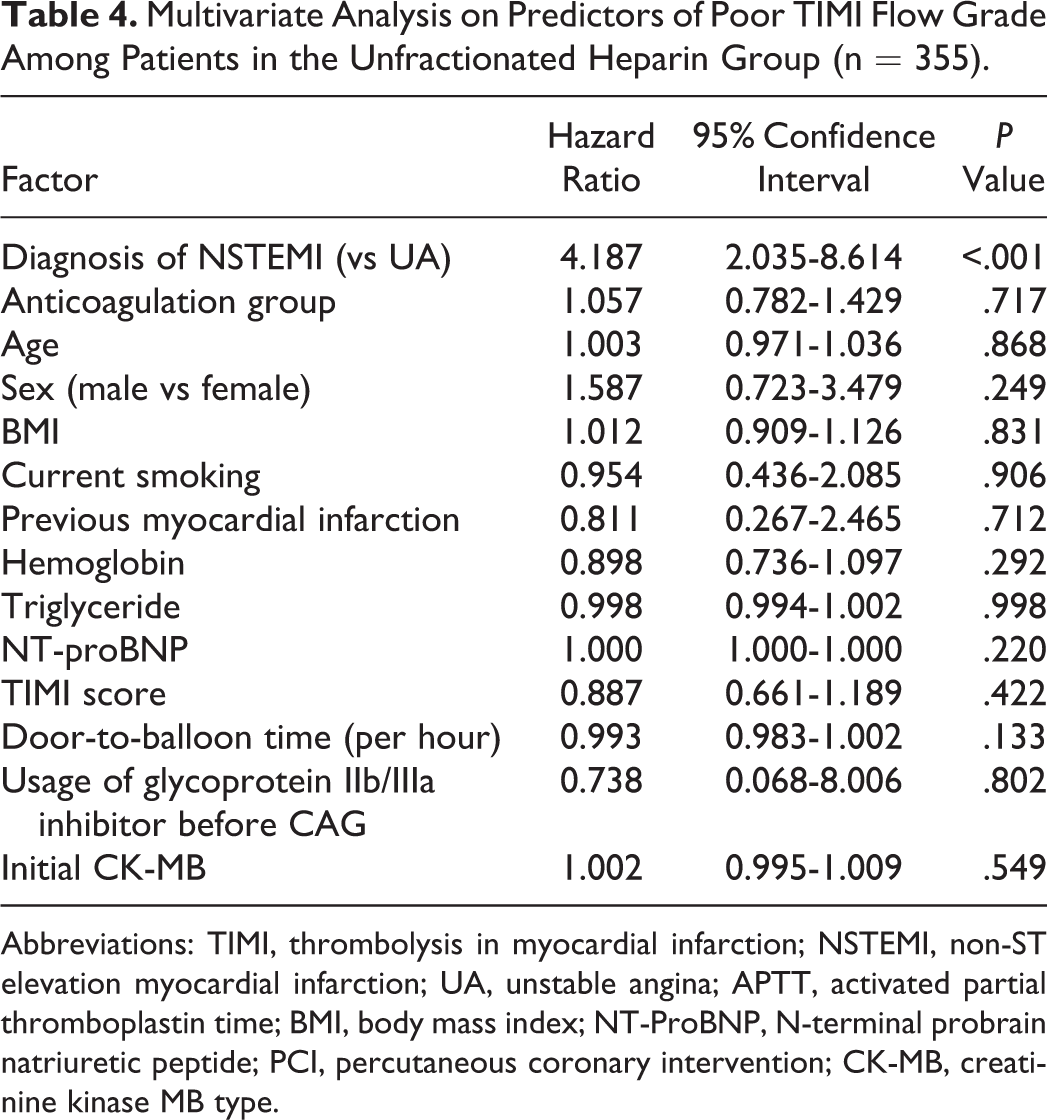
At CAG, 62.4% had normal preprocedural coronary blood flow (TIMI flow grade 3) and 14.3%, 5.5%, and 17.7% had a TIMI flow grade 2, 1, and 0, respectively. The proportion of poor coronary blood flow (TIMI flow grade <3) was 39.1% in the 100% low APTT group, 30.5% in the 99%∼50% low APTT group, 30.3% in the 49%∼1% low APTT group, and 33.9% in the 0% low APTT group, which had no significant difference (P for trend = .632; Figure 4). A multivariate logistic regression analysis was performed to determine the factors affecting TIMI flow grade. As a result, the diagnosis of non-ST elevation MI compared to unstable angina was an independent predictor of poor coronary blood flow, and the adequacy of anticoagulation was not an independent predictor of poor coronary blood flow (Table 4).
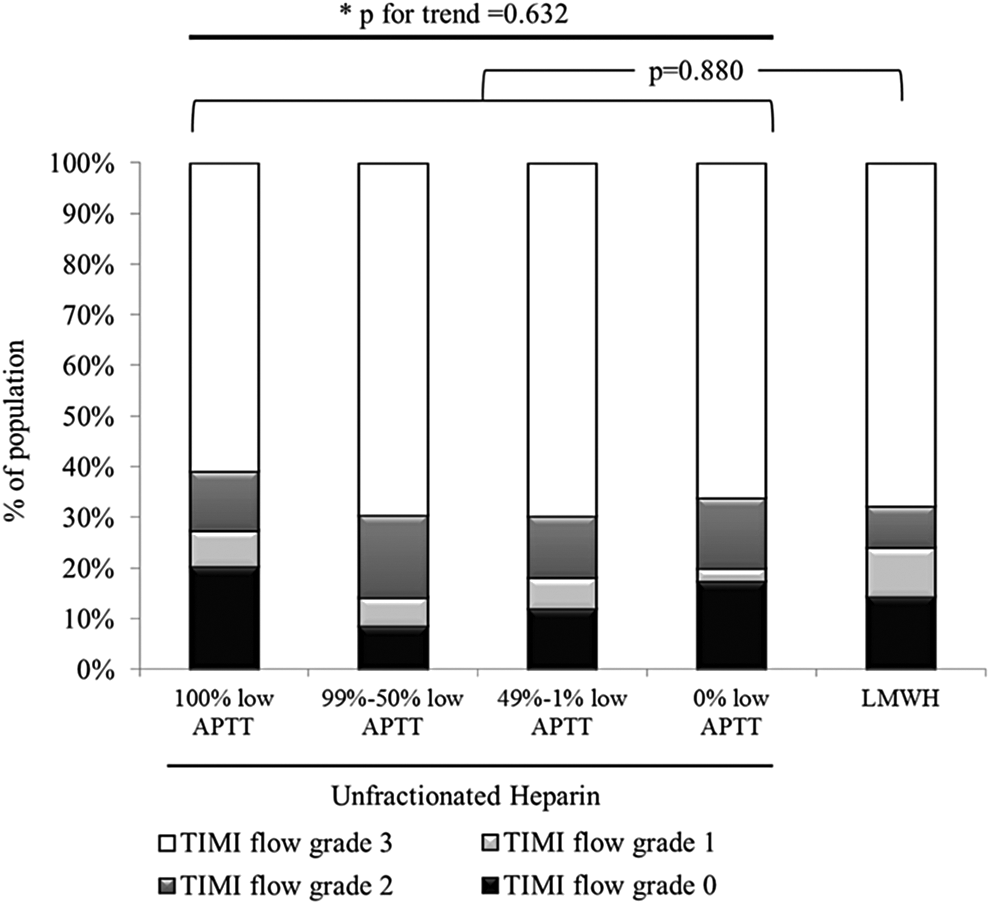
Preprocedural coronary flow difference between the groups. TIMI indicates thrombolysis in myocardial infarction; LMWH, low-molecular-weight heparin.
Multivariate Analysis on Predictors of Poor TIMI Flow Grade Among Patients in the Unfractionated Heparin Group (n = 355).
Abbreviations: TIMI, thrombolysis in myocardial infarction; NSTEMI, non-ST elevation myocardial infarction; UA, unstable angina; APTT, activated partial thromboplastin time; BMI, body mass index; NT-ProBNP, N-terminal probrain natriuretic peptide; PCI, percutaneous coronary intervention; CK-MB, creatinine kinase MB type.
For secondary end points, the proportion of visible thrombus, which was present in 34.8% of the whole population, did not differ according to the adequacy of anticoagulation (P for trend = .508). Periprocedural MI measured by cardiac troponin-I (P for trend = .523) and 30-day MACEs (P for trend = .867) also were not significantly different between the groups (Table 5). Moreover, when comparing the outcomes between the UFH (355 patients) and LMWH (62 patients) groups, no significant difference was found (Figure 4; Table 5).
Outcomes According to Anticoagulation.a
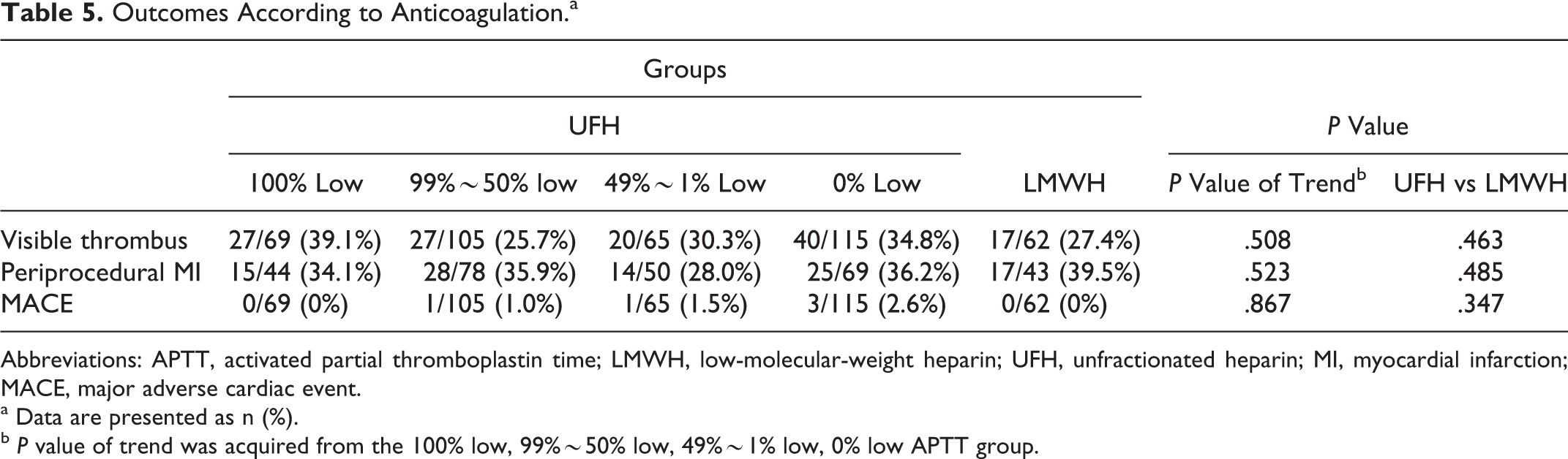
Abbreviations: APTT, activated partial thromboplastin time; LMWH, low-molecular-weight heparin; UFH, unfractionated heparin; MI, myocardial infarction; MACE, major adverse cardiac event.
a Data are presented as n (%).
b P value of trend was acquired from the 100% low, 99%∼50% low, 49%∼1% low, 0% low APTT group.
Bleeding Events
Overall, 14 bleeding events occurred during the 30 days after PCI. Among them, there were 2 BARC type 1 bleeding events and 12 BARC type 3 bleeding events. To determine the factors affecting bleeding events, a multivariate logistic regression analysis was done using variables with a P value < .1 on univariate analysis and the percentage of high APTT levels as an additional variable. Results showed usage of glycoprotein IIb/IIIa inhibitors was the only independent predictor of bleeding events (HR: 8.040, 95% CI: 1.437-44.994, P = .018). It was also noted that no bleeding events occurred in the LMWH group, although there was no statistical significance compared with the UFH group (14 of 355 [3.9%] vs. 0 of 62 [0.0%], P = .112 in the UFH group and LMWH group, respectively).
Discussion
Our study investigated the effect of adequate anticoagulation in patients with NSTE-ACS, by grouping patients according to the anticoagulant (UFH or LMWH) and the adequacy of anticoagulation tested by APTT (percentage of low APTT during anticoagulation period). There were 3 major findings from this analysis. First, after the starting dose of UFH, only 23.1% of the patients achieved the prespecified target anticoagulation level on the 6-hour APTT test. Second, there was no significant difference in primary and secondary outcomes (preprocedural coronary blood flow, presence of visible thrombus, periprocedural MI, and 30-day MACE) between the groups. Finally, bleeding events were affected by the usage of glycoprotein IIb/IIIa inhibitors, whereas the anticoagulation level did not have a significant effect.
Adequacy of Anticoagulation
As seen in the results, although the use of anticoagulation in the treatment of patients with NSTE-ACS is routine, the proportion of patients with therapeutic APTT levels is low. Less than a quarter of patients had an optimal 6-hour APTT (23.1%), and this percentage did not increase significantly in subsequent APTTs. The low proportion of optimal APTT was similar to the previous reports, where Cheng et al reported only 33.8% of the initial APTT in patients with ST elevation MI were in the therapeutic range, 13 and Thomas et al reported less than 50% of patients with NSTE-ACS achieved the target anticoagulation at any point during the initial 72 hours of treatment with UFH. 7 Patients who are likely to be inadequately anticoagulated could be monitored for optimal APTT levels more frequently or be administered with LMWH that do not require APTT monitoring.
Effect of Inadequate Anticoagulation
Patients did not show a uniform trend even though the heparin dose was adjusted according to the nomogram. Regardless of the 6-hour APTT level, the proportion of patients who showed optimal APTT levels was similar in the 12-hour and 18-hour tests. Therefore, we grouped patients by the percentage of low APTT levels during the anticoagulation period.
In our study, 62.4% of the patients had normal preprocedural coronary blood flow (TIMI flow grade 3) which was similar to the previous studies in Korea. 14,15 However, the type of anticoagulant or the adequacy of anticoagulation was not associated with angiographic and periprocedural outcomes such as poor coronary blood flow, presence of visible thrombus in CAG, and periprocedural MI. Although adequate anticoagulation with UFH had a favorable outcome in ST elevation MI, 16 this is not so clear in NSTE-ACS. 7 The lack of significant difference according to the adequacy of anticoagulation may also be due to the pre-PCI treatment, in which loading doses of aspirin 300 mg and clopidogrel 300 mg were given as soon as possible in the emergency department, and other adjunctive medications such as glycoprotein IIb/IIIa inhibitors. Inhibiting platelet activity is well known to contribute to the improvement in coronary blood flow in NSTE-ACS. 16 –18
Along with the angiographic and periprocedural outcomes, there was no significant difference in MACE according to anticoagulation. Clinical outcomes could have been influenced by various factors other than anticoagulation, such as administration of glycoprotein IIb/IIIa inhibitors, use of thrombus aspiration devices during PCI, concomitant medications with dual antiplatelets, 19 and clinical risk factors. 20 Previous studies have also shown inconsistent effect of anticoagulation with clinical outcomes. 5 –7,14,21 –23
It was noteworthy that outcomes in the LMWH group were numerically similar to the UFH group. This is consistent with a large systematic overview comparing the effect of LMWH and UFH, where LMWH has been proved to be equivocal to UFH, especially in those who received glycoprotein IIb/IIIa inhibitors. 24
Various Factors Affect Bleeding Events
For hemorrhagic complications, the anticoagulation level had no significant effect and instead, the usage of glycoprotien IIb/IIIa inhibitors significantly increased bleeding events by 8-fold. Although excessive anticoagulation by UFH was associated with increased bleeding events in the previous studies, 3,6 the effect may not be as substantial as before, when more powerful antithrombotic agents are currently used. Glycoprotein IIb/IIIa inhibitors are known to be a strong antithrombotic agents, 25 used in a cautious manner to decrease ischemic events in the risk of hemorrhagic events. 26 It was also remarkable that none of the patients in the LMWH group experienced bleeding events within the 30 days follow-up period. Previous reports have shown conflicting effects on bleeding rates in patients receiving LMWH or UFH before PCI, 21,22 whereas a recent large real-world trial showed less bleeding events in the LMWH group. 27
Limitations
Our study has some limitations. First, the current study was not a randomized trial but rather a post hoc analysis; therefore, all clinical variables could not be adequately controlled. However, the differences in baseline characteristics were not so big, and a multivariate analysis was performed to compensate for the differences. Second, the study sample size might not be large enough to fully evaluate the subtle differences in end points. For further investigation, studies with larger sample size are warranted. Third, the use of UFH may be outdated in the treatment of patient with NSTE-ACS. The European Society of Cardiology (ESC) Guidelines for the management of ACS in patients presenting without persistent ST-segment elevation recommend UFH with a target APTT of 50 to 70 seconds only if fondaparinux or enoxaparin is not available (class I, Level of Evidence C). 28 However, UFH is still the most commonly used anticoagulant in patients with ACS, in South Korea.
Conclusion
Although UFH is a commonly used anticoagulant, the adequacy of anticoagulation is quite low. Our findings highlight the insignificant difference in adverse outcomes, such as poor preprocedural coronary blood flow, visible thrombus, and periprocedural MI, according to the subtherapeutic anticoagulation. The benefit of adequate anticoagulation may be insignificant in patients with NSTE-ACS, when adjunctive medications such as dual antiplatelet therapy and glycoprotein IIb/IIIa inhibitors are administered concomitantly.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.