
Abstract
This study aimed to examine the hemostatic abnormalities in patients with systemic
sclerosis (SSc) and the relationship between these abnormalities and thrombotic events
(THEs), focusing on the difference in diffuse cutaneous SSc (dcSSc) and limited cutaneous
SSc (lcSSc). The plasma levels of ADAMTS-13 (a disintegrin-like and metalloproteinase with
thrombospondin type 1 motifs 13), von Willebrand factor (VWF), VWF propeptide (VWFpp),
Introduction
Connective tissue diseases (CTDs), especially systemic lupus erythematosus (SLE), 1 are well known to be accompanied by a high-risk disease of developing various thrombotic events (THEs), including deep vein thrombosis (DVT), pulmonary embolism (PE), cerebral thrombosis, acute coronary syndrome, and thrombotic microangiopathy (TMA). 2 While the reported frequency of THEs is low in non-SLE CTD patients, including those with systemic sclerosis (SSc), 3 the risk of THEs in patients with SSc is still higher than in non-SSc individuals. 4 –6 Indeed, cardiovascular disease accounts for 20% to 30% of all SSc deaths. 7 Various biomarkers of inflammation, thrombophilia, and organ dysfunction have been identified in patients with SSc. 8 –12 It is also known that around half of patients with SSc having renal crisis develop TMA. 13
ADAMTS-13, a disintegrin-like and metalloproteinase with thrombospondin type 1 motifs 13, cleaves unusual large multimers of von Willebrand factor (VWF) to inhibit the pathological activation of platelets. Thrombotic thrombocytopenic purpura, caused by a severe deficiency of ADAMTS-13, 14 is a major complication in CTD and causes around 20% of TMA in patients with CTD. 15 The serum levels of the vascular endothelial cell injury markers VWF, VWF propeptide (VWFpp), 16 and thrombomodulin (TM), 17 are elevated in patients with TMA or disseminated intravascular coagulation.
As we reported previously, the plasma levels of VWF and VWFpp are elevated in patients with SSc and antiphospholipid antibody syndrome (APS), 18 suggesting the presence of vascular endothelial cell injury. In the present study, we measured the plasma levels of ADAMTS-13, VWF, VWFpp, and several other hemostatic biomarkers in 233 patients with SSc and evaluated the relationship between these hemostatic biomarkers and several manifestations of SSc, including the spread of skin involvement, THE, interstitial lung disease (ILD), and complication of other CTDs.
Materials and Methods
The patients who consulted the clinics of dermatology or hematology at Mie University Hospital from January 1, 1994, to December 31, 2016, were enrolled in the present study. We diagnosed SSc according to the 2013 Classification Criteria for Systemic Sclerosis (American College of Rheumatology/European League Against Rheumatism [ACR/EULAR]) 19 and classified patients as having limited cutaneous SSc (lcSSc) and diffuse cutaneous SSc (dcSSc) based on the definition of LeRoy and Medsger. 20 Systemic lupus erythematosus was diagnosed by the 1997 update of the 1982 American College of Rheumatology Revised Criteria for Classification of Systemic Lupus Erythematosus. 21 Dermatomyositis and polymyositis were diagnosed based on the criteria of Bohan and Peter. 22,23 Sjögren syndrome was diagnosed based on the 2012 American College of Rheumatology Classification Criteria for Sjögren Syndrome. 24 Rheumatoid arthritis was diagnosed based on the 2010 Rheumatoid Arthritis Classification Criteria: ACR/EULAR. 25 As controls, healthy volunteers matched for age and sex were randomly selected.
Thrombosis was diagnosed based on the clinical manifestations and was confirmed by appropriate clinical and radiological examinations. The presence of PE and DVT was diagnosed by a whole-leg compression ultrasound examination and/or contrast computed tomography (CT). Cerebral and other organ thromboses were diagnosed by CT or magnetic resonance imaging. Thrombotic events diagnosed within 3 days after the onset were classified as acute THE. Thrombosis that developed more than a month before was classified as past THE. The presence of ILD was defined by the radiology reports: the presence of any ground-glass appearance, fibrotic interstitial changes, or honeycombing. ILD was then confirmed by high-resolution CT. 26,27
The plasma samples were prepared as reported previously.
8
In brief, plasma was separated using a 0.38% sodium citrate preparation with
3000g centrifugation at 4°C for 15 minutes. The plasma was stored at
−80°C until use. The ADAMTS-13 activity was measured by Kokame method using a FRETS-VWF73
peptide (Peptide Institute, Inc, Osaka, Japan).
28
The plasma levels of VWF and VWFpp were measured by a VWF & Propeptide assay kit
(GTI Diagnostics, Waukesha, Wisconsin).
29
The plasma levels of soluble fibrin (SF) and
The study protocol was approved by the human ethics review committee of Mie University School of Medicine (approval number: 2629), and informed consent was obtained from all the patients. This study was carried out in accordance with the principles of the Declaration of Helsinki.
Statistical Analyses
The results were expressed as the median (25th-75th percentiles). Differences between groups were analyzed using the Mann-Whitney U test. P values of <.05 were considered to indicate a statistically significant difference. The significance of a frequency was examined by the χ2 test. All statistical analyses were performed using the SPSS Statistics software program (version 22; IBM, New York, New York).
Results
The laboratory data of 233 patients with SSc were serially investigated, including 173 patients with lcSSc (mean age, 64.5 [11.7] years) and 60 patients with dcSSc (mean age, 68.0 [11.3] years), 19 as shown in Table 1. All of THEs that developed in lcSSc and dcSSc are shown in Table 2. In patients with SSc, the plasma levels of ADAMTS-13 were significantly decreased and the plasma levels of VWF and VWFpp were significantly elevated compared to those of healthy controls (P < .001; Figure 1A–C).
Patients.
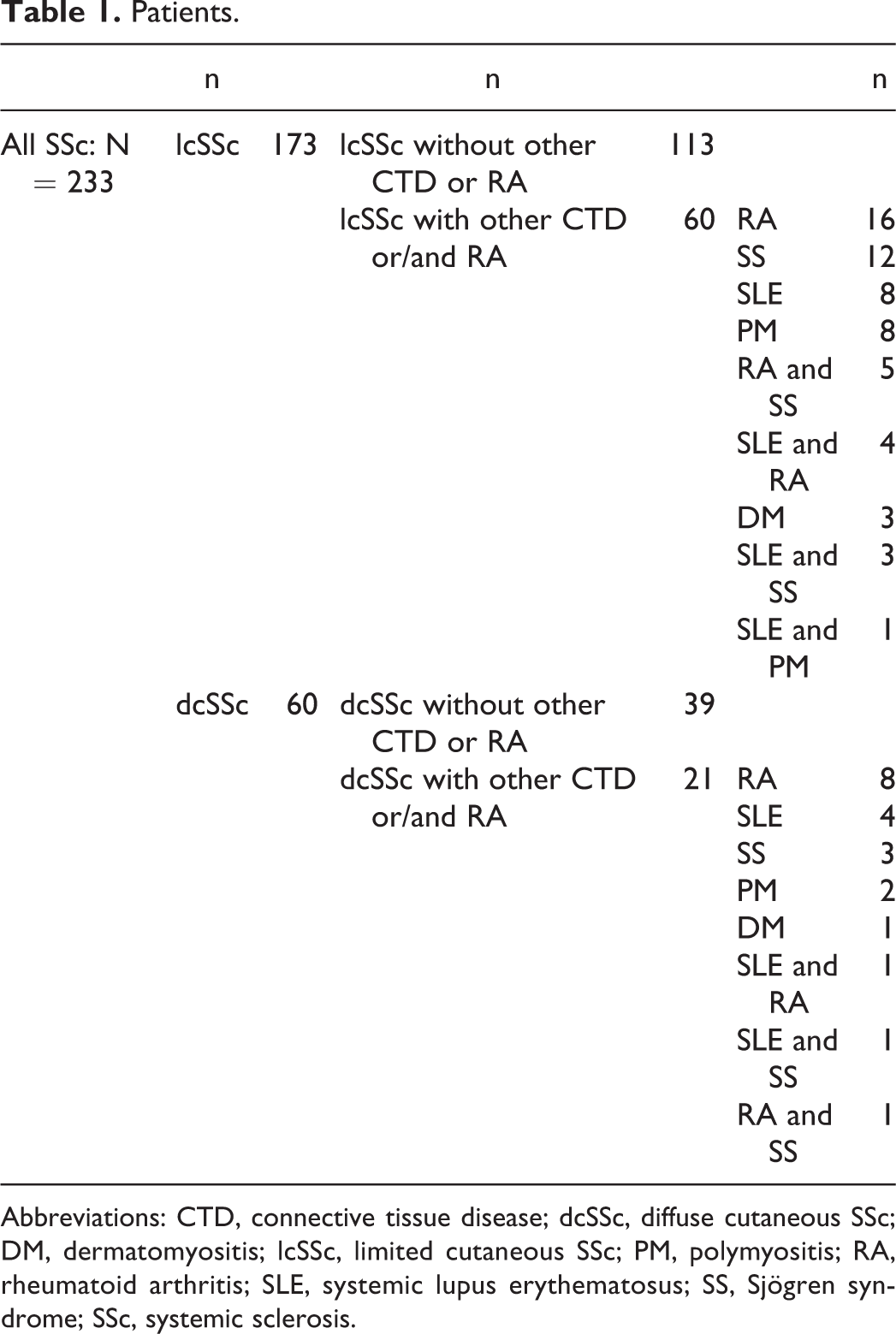
Abbreviations: CTD, connective tissue disease; dcSSc, diffuse cutaneous SSc; DM, dermatomyositis; lcSSc, limited cutaneous SSc; PM, polymyositis; RA, rheumatoid arthritis; SLE, systemic lupus erythematosus; SS, Sjögren syndrome; SSc, systemic sclerosis.
All THEs Developed in LcSSc and DcSSc.
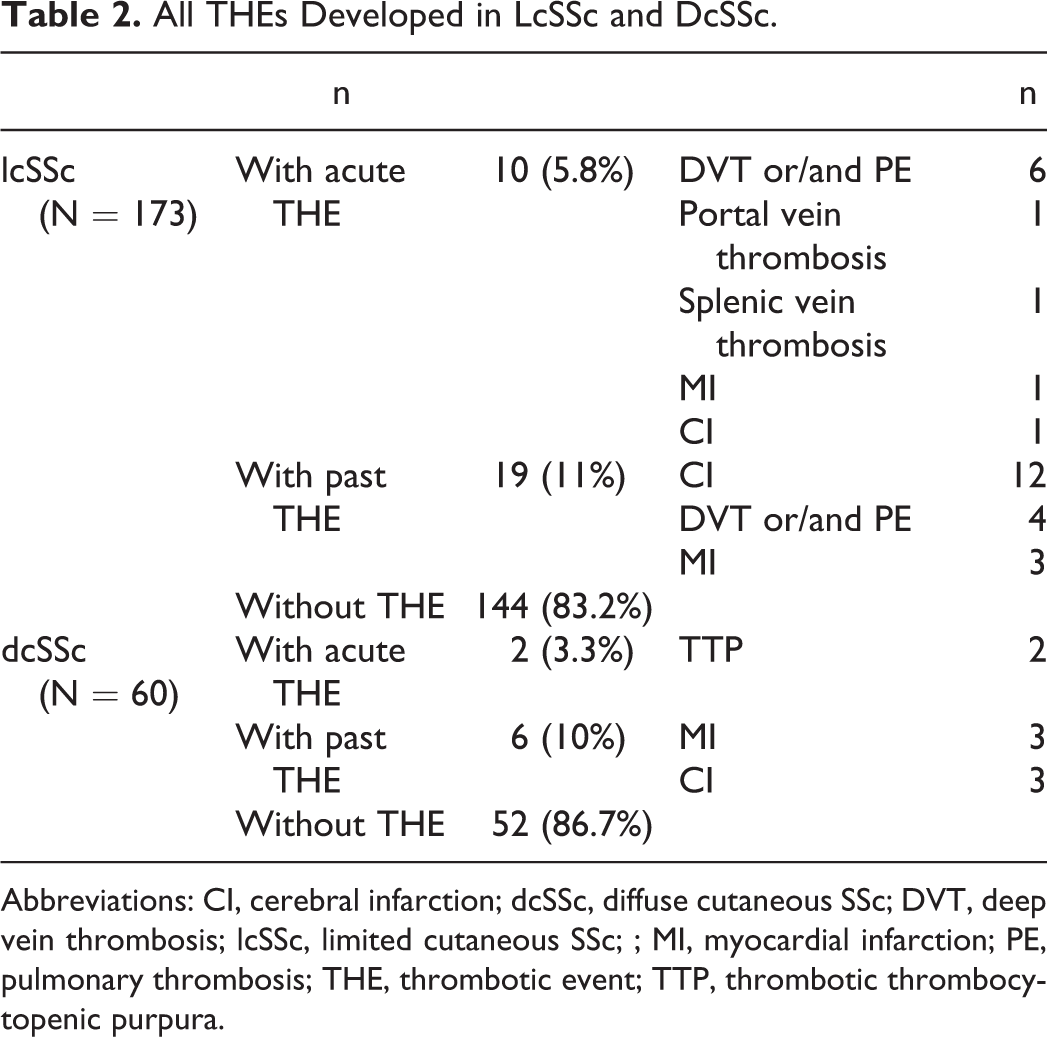
Abbreviations: CI, cerebral infarction; dcSSc, diffuse cutaneous SSc; DVT, deep vein thrombosis; lcSSc, limited cutaneous SSc; ; MI, myocardial infarction; PE, pulmonary thrombosis; THE, thrombotic event; TTP, thrombotic thrombocytopenic purpura.
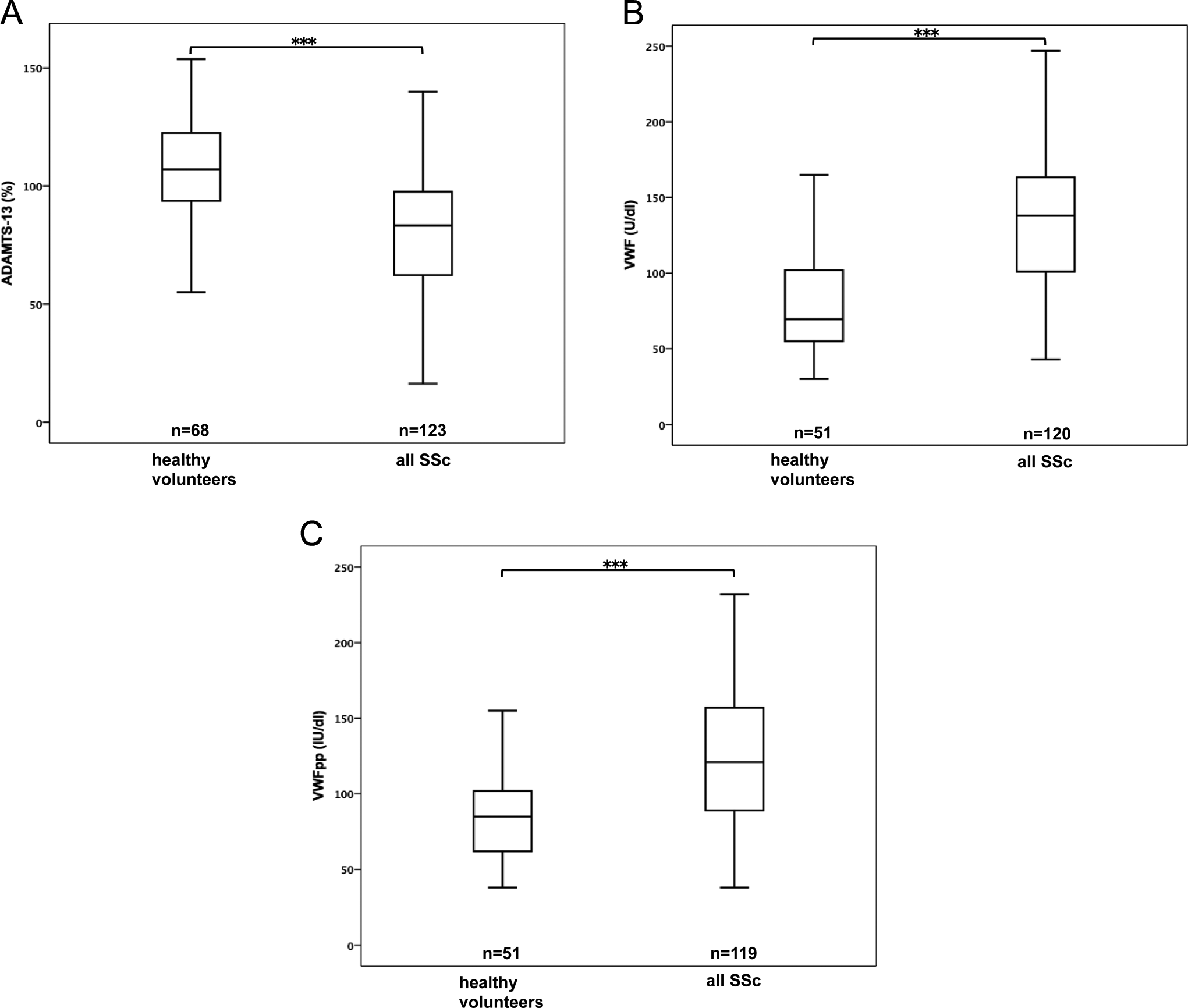
A, Plasma ADAMTS-13 activity in systemic sclerosis (SSc) and healthy volunteers. B, Plasma von Willebrand factor (VWF) levels in SSc and healthy volunteers. C, Plasma von Willebrand factor propeptide (VWFpp) levels in SSc and healthy volunteers. ***P < .001 (Mann-Whitney U test).
Between patients with lcSSc and dcSSc, no significant difference was detected in values of ADAMTS-13, VWF, D-dimer, SF, TM/estimated glomerular filtration rate (eGFR), or TRPG. However, the plasma levels of VWFpp and eGFR were significantly higher in patients with dcSSc than in those with lcSSc (P < .05). There were no significant differences in the risk of acute THE or past THE between lcSSc and dcSSc (Table 3).
A Comparison Between LcSSc and DcSSc.a
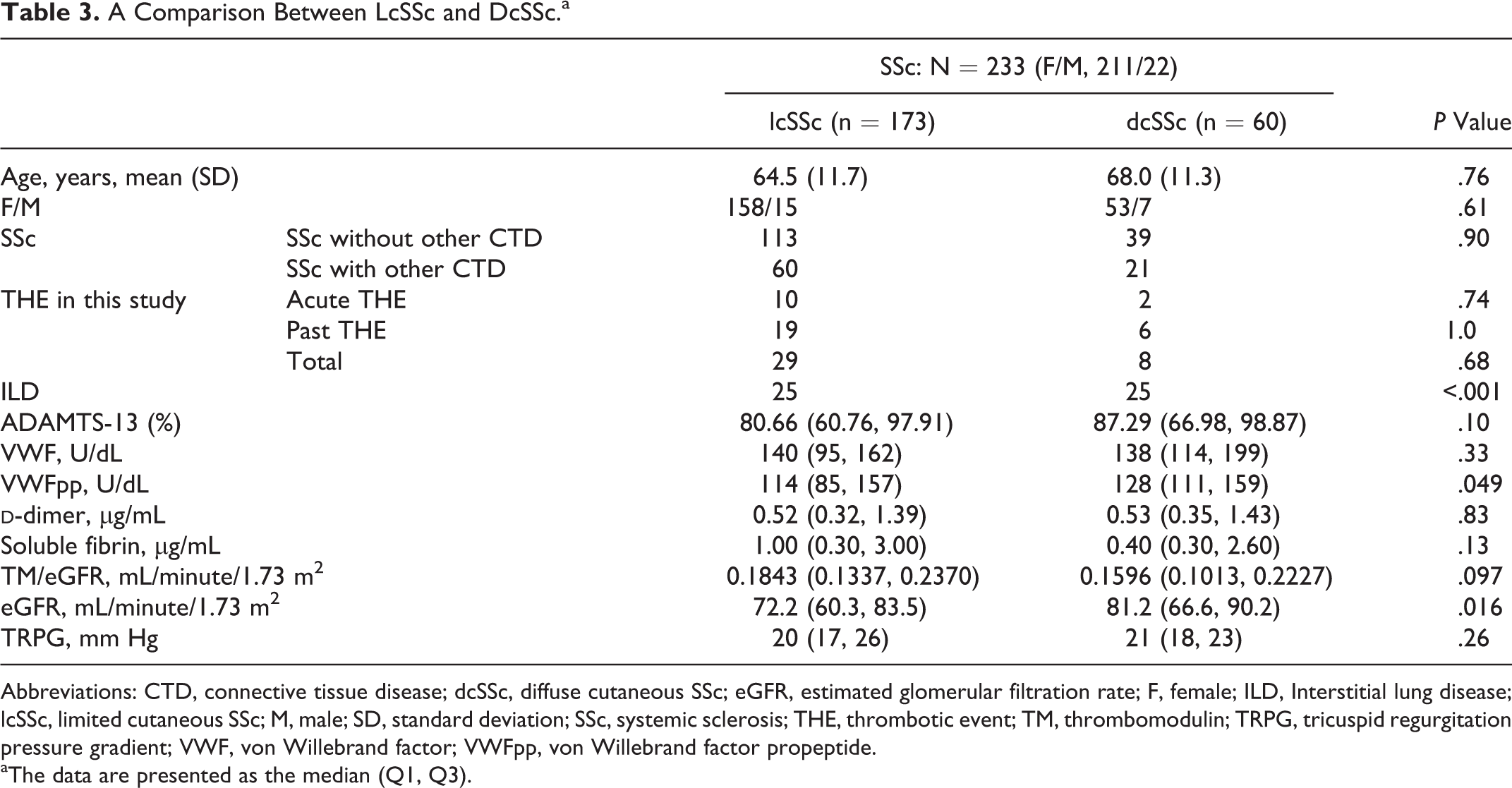
Abbreviations: CTD, connective tissue disease; dcSSc, diffuse cutaneous SSc; eGFR, estimated glomerular filtration rate; F, female; ILD, Interstitial lung disease; lcSSc, limited cutaneous SSc; M, male; SD, standard deviation; SSc, systemic sclerosis; THE, thrombotic event; TM, thrombomodulin; TRPG, tricuspid regurgitation pressure gradient; VWF, von Willebrand factor; VWFpp, von Willebrand factor propeptide.
aThe data are presented as the median (Q1, Q3).
The plasma levels of
A Comparison Between Patients Having SSc With and Without THE.a
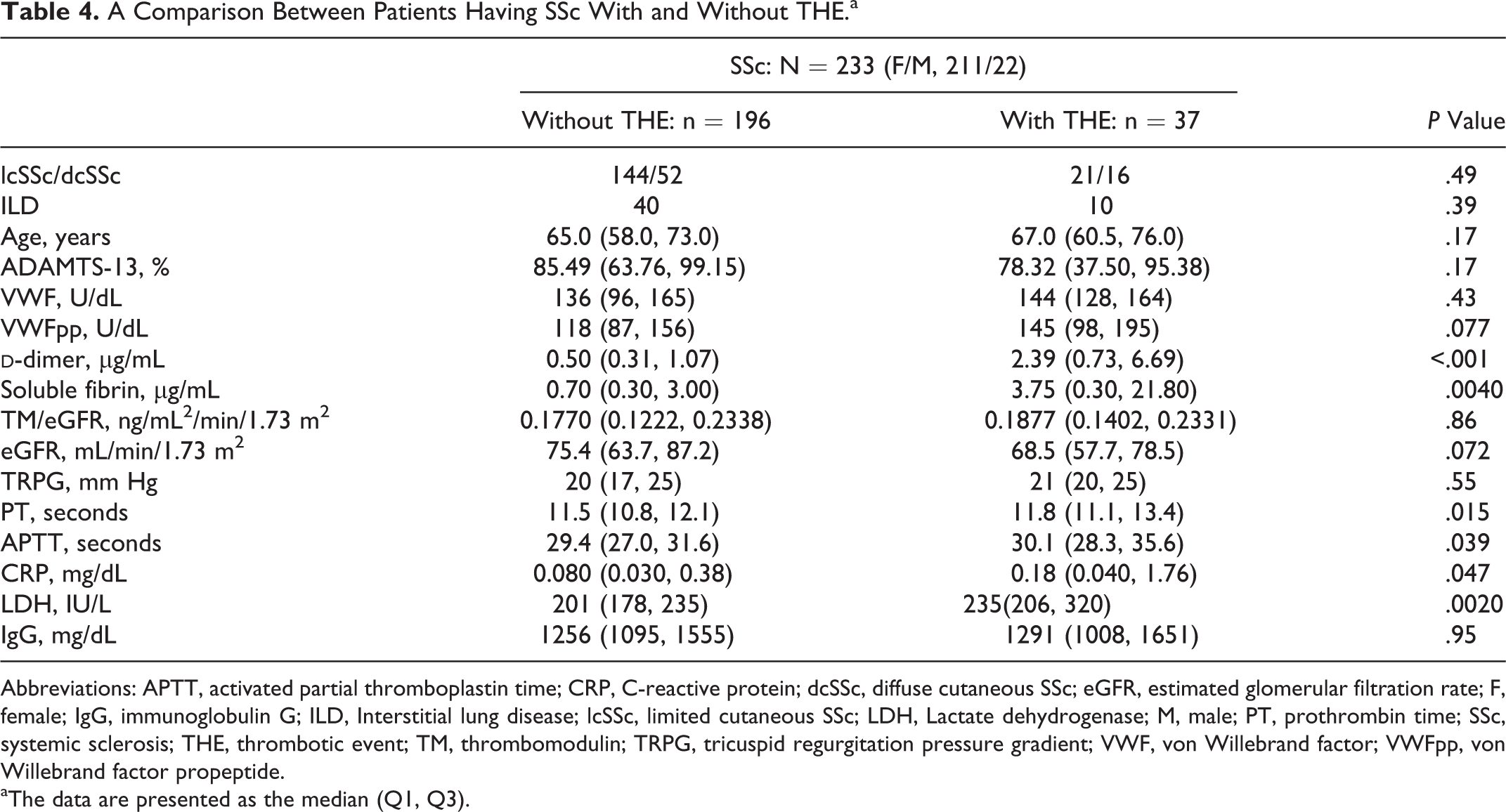
Abbreviations: APTT, activated partial thromboplastin time; CRP, C-reactive protein; dcSSc, diffuse cutaneous SSc; eGFR, estimated glomerular filtration rate; F, female; IgG, immunoglobulin G; ILD, Interstitial lung disease; lcSSc, limited cutaneous SSc; LDH, Lactate dehydrogenase; M, male; PT, prothrombin time; SSc, systemic sclerosis; THE, thrombotic event; TM, thrombomodulin; TRPG, tricuspid regurgitation pressure gradient; VWF, von Willebrand factor; VWFpp, von Willebrand factor propeptide.
aThe data are presented as the median (Q1, Q3).
The prevalence of ILD in patients with dcSSc was significantly higher than in those with lcSSc, in concordance with previous findings (P < .001; Table 3). Surprisingly, the plasma levels of VWF and VWFpp were significantly higher in the patients with SSc with ILD than in those without ILD (P < .05). In patients with SSc having other CTDs, the plasma levels of VWF and VWFpp in patients with SSc with ILD were significantly high than in those without ILD (P < .05; Table 5).
A Comparison Between Patients Having SSc With and Without ILD.a
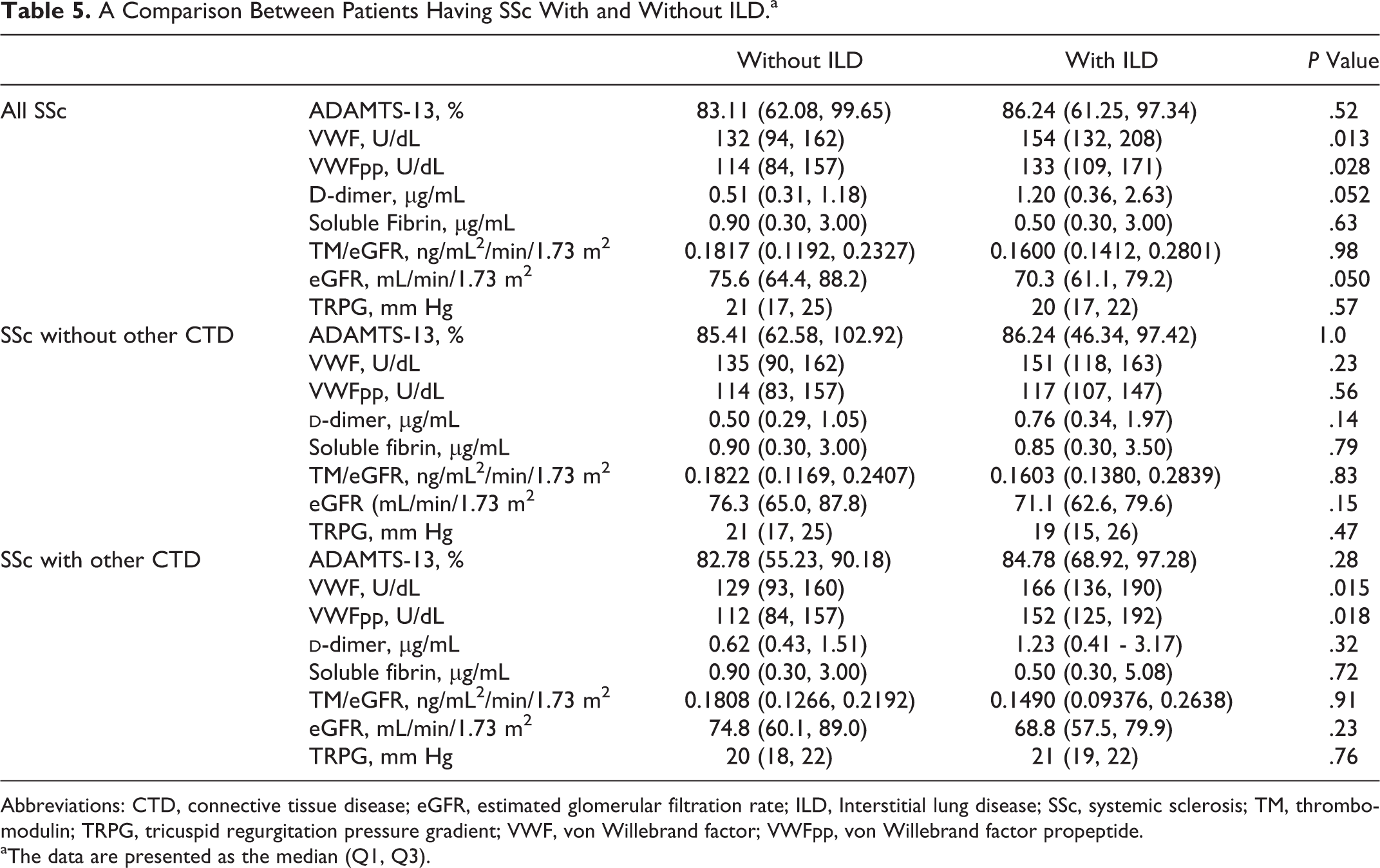
Abbreviations: CTD, connective tissue disease; eGFR, estimated glomerular filtration rate; ILD, Interstitial lung disease; SSc, systemic sclerosis; TM, thrombomodulin; TRPG, tricuspid regurgitation pressure gradient; VWF, von Willebrand factor; VWFpp, von Willebrand factor propeptide.
aThe data are presented as the median (Q1, Q3).
The plasma
A Comparison Between Patients Having SSc With and Without Other CTD.a
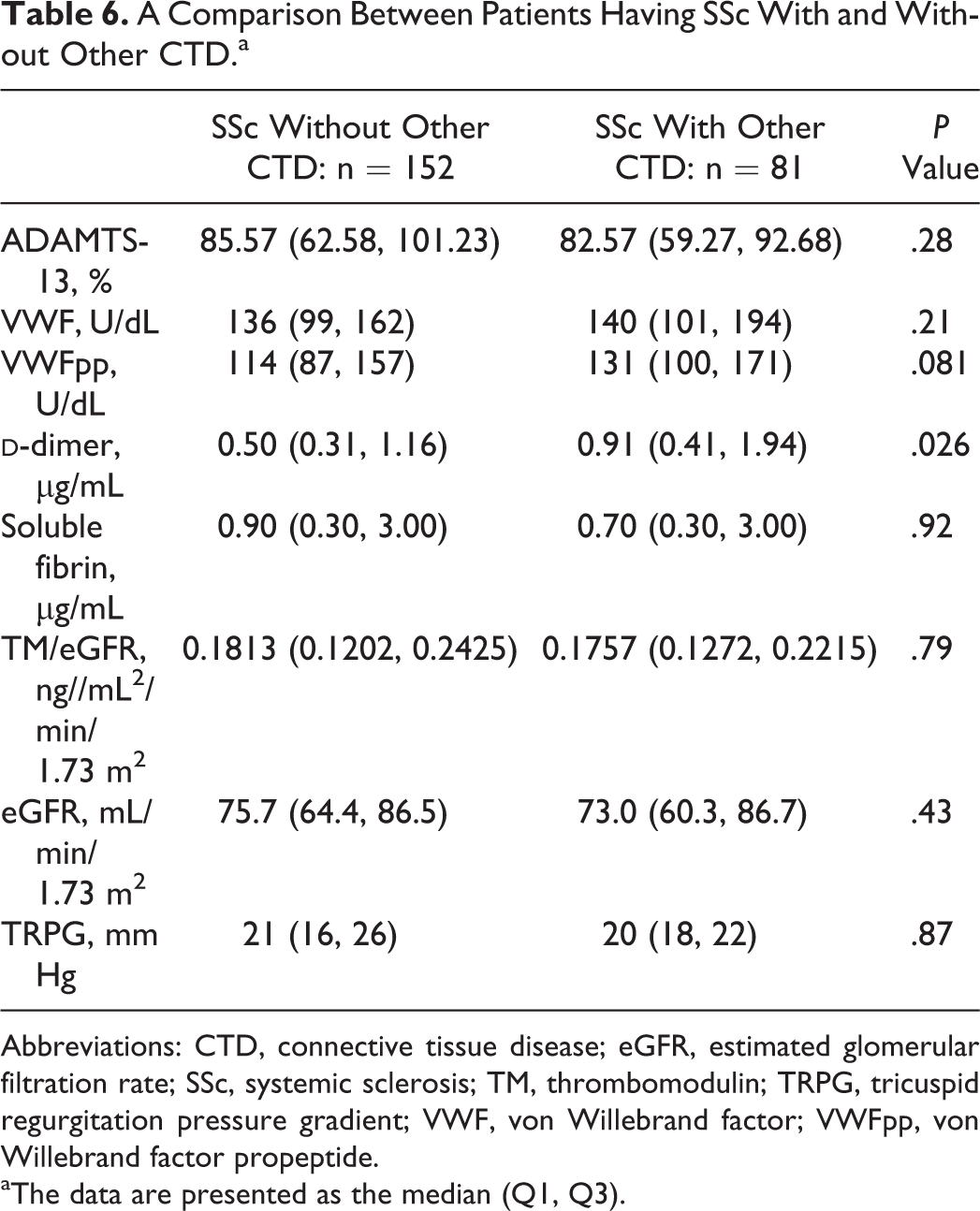
Abbreviations: CTD, connective tissue disease; eGFR, estimated glomerular filtration rate; SSc, systemic sclerosis; TM, thrombomodulin; TRPG, tricuspid regurgitation pressure gradient; VWF, von Willebrand factor; VWFpp, von Willebrand factor propeptide.
aThe data are presented as the median (Q1, Q3).
A Comparison Between Patients Having SSc With Low and High D-Dimer Level.a
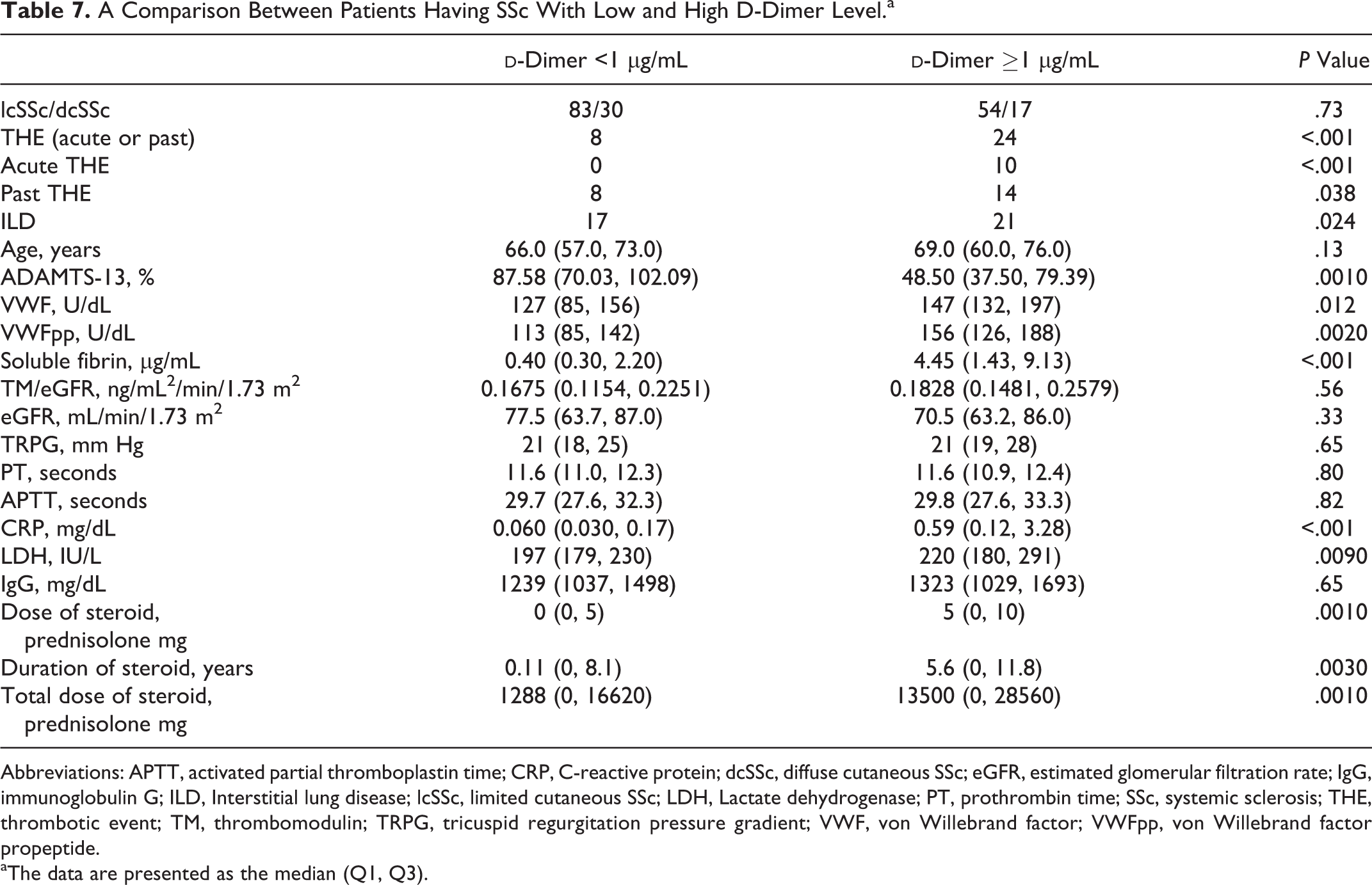
Abbreviations: APTT, activated partial thromboplastin time; CRP, C-reactive protein; dcSSc, diffuse cutaneous SSc; eGFR, estimated glomerular filtration rate; IgG, immunoglobulin G; ILD, Interstitial lung disease; lcSSc, limited cutaneous SSc; LDH, Lactate dehydrogenase; PT, prothrombin time; SSc, systemic sclerosis; THE, thrombotic event; TM, thrombomodulin; TRPG, tricuspid regurgitation pressure gradient; VWF, von Willebrand factor; VWFpp, von Willebrand factor propeptide.
aThe data are presented as the median (Q1, Q3).
Discussion
Systemic sclerosis induces systemic inflammation followed by severe vascular lesions of small arteries, smooth muscle involvement of digestive systems, and collagen deposition in skin, lung, and various internal organs. Clinically, typical skin lesions, including digital ulcers, nail fold capillary thrombosis, and digital pitting scars, are suggestive of the presence of ischemic vascular changes and hemostatic and/or coagulation abnormalities. In general, these changes are more apparent in dcSSc than in lcSSc.
However, in contrast to arterial vascular changes, the venous abnormalities associated with SSc have not been fully investigated. The incidence of venous thromboembolism (VTE) per 1000 person-years was reported to be 6.56 in patients with SSc, and the multivariable hazard ratio for VTE among patients with SSc was 3.47 in comparison to non-SSc patients. 4 Interestingly, the present study noted the development of acute THE in 5.8% of patients with lcSSc and 3.3% of patients with dcSSc and past THE in 11.0% of patients with lcSSc and 10.0% of patients with dcSSc. This suggests a high risk of THE in SSc. Surprisingly, the prevalence of THE showed no marked difference between patients with lcSSc and dcSSc. This implies the presence of other factors related to THE in patients with SSc. The overlap of other CTDs is common in patients with SSc, and CTDs other than SSc, especially SLE, induce the development of various THEs more often than does SSc. 3,30 The present study revealed an increase in the THE risk by the overlap of CTDs complicating hemostatic abnormalities.
Patients with SSc showed lower plasma levels of ADAMTS-13 and higher plasma levels of VWF
and VWFpp than healthy participants, suggesting that high coagulability exists in patients
with SSc. The plasma levels of
The plasma levels of VWFpp were significantly elevated in patients with dcSSc, suggesting the greater vascular endothelial cell injury in patients with dcSSc than in patients with lcSSc. The prevalence of ILD is known to be higher in patients with dcSSc than in patients with lcSSc. However, the pathogenesis of ILD has not been fully clarified. Surprisingly, the plasma levels of VWF and VWFpp were significantly higher in the patients with SSc with ILD than in those without ILD in the present study, suggesting a close relationship between ILD and vascular endothelial cell injury. Interestingly, very strong expression of VWF messenger RNA and the presence of immunoreactive VWF in the endothelial cells of murine small and microvessels of the lungs have been reported. 34 The present results suggest the involvement of VWF and VWFpp in pulmonary endothelial cells in the pathogenesis of ILD in patients with SSc.
In conclusion, SSc carries a high risk of THE, especially in patients with other CTDs. Plasma hemostasis-related markers are closely related to ILD and THE. These markers are important as markers of organ involvement as well as THE.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by a Grant-in-Aid from the Ministry of Health, Labor and Welfare and Research on intractable diseases of Japan for systemic sclerosis.