
Abstract
High platelet to lymphocyte ratio (PLR) and neutrophil to lymphocyte ratio (NLR) are associated with an increased risk of arterial thrombosis, but their role in venous thromboembolism (VTE) has not been fully investigated. A case–control study, of 486 patients with VTE, 100 with cerebral vein thrombosis (CVT), and 299 healthy individuals, was carried out to investigate whether high PLR or NLR values are associated with an increased risk of VTE. Patients with high PLR or NLR did not have an increased risk of VTE (odds ratio [OR] 0.89, 95% confidence interval [CI]: 0.46-1.76; OR: 0.69, 95% CI: 0.34-1.39, respectively) or CVT (OR: 1.65, 95% CI: 0.68-4.00; OR: 0.39, 95% CI: 0.09-1.72, respectively). Subgroups analysis showed that high PLR values were associated with the risk of provoked CVT (OR: 2.65, 95% CI: 1.02-6.92), and there was an interaction with thrombophilia abnormalities (OR: 7.67, 95% CI: 1.67-35.27) in patients with CVT. In conclusion, high PLR and NLR values are not associated with an overall increased risk of VTE or CVT. High PLR values increase the risk of provoked CVT and interact with thrombophilia abnormalities in patients with CVT.
Keywords
Introduction
Venous thromboembolism (VTE) is a major cause of morbidity and mortality worldwide. 1 The identification of acquired or inherited risk factors for VTE has the potential to improve the management of patients and the general health of the population, helping to adopt the best preventive strategies in subgroups of individuals at particularly high risk.
There is a close link between inflammation and thrombosis 2 and growing evidence that platelets and neutrophils play an important role in the development of VTE. 3,4 Platelet to lymphocyte ratio (PLR) is considered a novel marker that integrates the information about primary hemostasis and inflammation pathways and seems to be more informative than platelet count alone. 5 So far, high PLR value has been associated with poor overall survival in several type of malignancies, 6 –9 found to be an independent predictor of mortality in patients with ST-elevated myocardial infarction, 10 and considered a prognostic marker in coronary artery disease, predicting severe atherosclerosis. 11 In addition, the neutrophil to lymphocyte ratio (NLR) is an established marker of subclinical inflammation, and high NLR value has been associated with the presence and the severity of coronary artery disease, 12 suggested as predictor of cardiovascular risk and mortality and considered a prognostic inflammatory marker in various vascular disorders, including severe atherosclerosis. 13
The role of PLR and NLR as risk factors for venous thrombosis has been poorly investigated, although both PLR and NLR indexes were found able to discriminate the risk of 30-day mortality in patients admitted for pulmonary embolism, 14 only 1 study investigate the association between levels of NLR and future risk or recurrent VTE, finding no association. 15
In light of the recent findings on the association between some alterations of whole blood count, such as red cell distribution width 16,17 and an increased risk of VTE, in this case–control study of exploratory nature, we aimed to investigate whether high PLR or NLR values, defined as exceeding the 95th percentile of the distribution among controls, were associated with an increased risk of VTE (deep vein thrombosis of the lower limbs and/or pulmonary embolism) or cerebral vein thrombosis (CVT).
Potential interactions between high PLR or NLR values and thrombophilia abnormalities were also investigated.
Patients and Methods
Study Population
Patients referred to the Angelo Bianchi Bonomi Thrombosis Center from January 2007 to December 2013 for thrombophilia screening after a first, symptomatic, objectively confirmed episode of VTE or CVT were included in the study. Deep vein thrombosis was diagnosed by compression ultrasound or venography; pulmonary embolism by ventilation/perfusion lung scan, spiral computed tomography (CT) scan, or pulmonary angiography; and CVT by cerebral CT scan, angio-nuclear magnetic resonance, or angiography. Venous thromboembolism or CVT episodes were considered provoked if they occurred in the presence of such transient risk factors as surgery, prolonged immobilization, trauma, pregnancy, puerperium, or oral contraceptive use and unprovoked in their absence. Patients with overt hematological or systemic neoplasms, inflammatory, hepatic or autoimmune disease and those with antiphospholipid antibodies were excluded from the study because all these conditions may affect platelet or leukocyte count. Also patients with hemoglobin levels below normal values (13.5 g/dL for men and 12.5 g/dL for women), who may consequently have an increased platelet count, were excluded.
Controls were partners or friends of patients referred to the Thrombosis Center in the same time period of patients for a thrombophilia work-up, in whom previous episodes of thrombosis were excluded by means of a validated questionnaire, 18 avoiding potential selection bias. Demographic and clinical data were collected at the time of the first visit at the Thrombosis Center. The study was approved by the Hospital institutional review board, and all patients and controls signed the informed consent before inclusion in the study.
Laboratory Tests
Blood samples were collected in vacuum tubes with EDTA as anticoagulant for automated complete blood count. For the thrombophilia, screening samples were collected into 3.2% sodium citrate and centrifuged within 15 minutes at 20°C for 20 minutes at 2880 ×g. The plasma obtained was aliquoted and snap-frozen in liquid nitrogen and then stored at −80°C until analysis. Thrombophilia testing included (i) DNA analysis for the 1691 guanine to adenine substitution in coagulation factor V gene (factor V Leiden) and for the 20210 guanine to adenine substitution in the 3′-untranslated region of the prothrombin gene 19,20 ; (ii) functional and immunoassays (when required) for plasma fibrinogen, antithrombin, protein C and protein S 21 ; (iii) antiphospholipid antibodies (lupus anticoagulant, anticardiolipin, and anti-β2 glycoprotein I immunoglobulin [Ig]G and IgM antibodies) 22 ; (iv) plasma factor VIII levels 23 with high levels defined when exceeded the 95th percentile of the distribution among controls; (v) fasting and postmethionine load (3.8 g per square meter of body surface area) homocysteine levels with hyperhomocysteinemia defined when exceeded the 95th percentile of the distribution among controls. 24
Serum creatinine and C-reactive protein were also measured. Creatinine clearance was calculated as a measure of renal function, according to the Cockroft-Gault formula. All samples were collected at least 3 months after VTE or CVT, in order to avoid changes in biological parameters related to the event, and for controls at the time of the visit.
Statistical Analysis
Continuous variables are presented as mean and standard deviation or median and interquartile range and categorical variables as count and percentage. Patients with VTE or CVT were compared to controls for high PLR and NLR values. Platelet to lymphocyte ratio and NLR medians were compared between groups with nonparametric Mann-Whitney U test and P values <.05 were considered statistically significant. The analyses were based on dichotomous exposures with cutoff values at the 95th percentile of the PLR and NLR distribution of controls, and individuals with values below the 95th percentile were used as reference category. The 95th percentile was chosen arbitrarily as cutoff value for both PLR and NLR. We estimated that with this prevalence exposure (5%), to detect a minimum clinically relevant OR of 2.5, with an α error of 0.05 and a power of 80%, 270 VTE cases and 107 CVT (case–control ratio of 1:3) were needed. The association between PLR or NLR with VTE or CVT were expressed in terms of odds ratios (ORs) as a measure of relative risk with corresponding 95% confidence intervals (CIs). Analyses were adjusted for possible confounders such as sex, age, and body mass index using a multivariable logistic regression model. Subgroup analyses were performed, stratifying according to the etiology of VTE or CVT (provoked or unprovoked). Finally, interaction analysis was performed to calculate the risk of VTE or CVT associated with the presence of high PLR or NLR values (above 95th percentile) and thrombophilia abnormalities. All analyses were performed with the statistical software SPSS (release 23.0, IBM SPSS Statistics for Windows, IBM Corp, Armonk, New York).
Results
The initial study cohort included 1159 patients with VTE, 234 patients with CVT, and 655 healthy controls. After exclusion of individuals with missing whole blood count, comorbidities, or low hemoglobin levels, 486 patients with VTE, 100 with CVT, and 299 controls remained (Figure 1). Demographic and clinical characteristics of patients excluded were similar to those of patients included in the final analysis and shown in Table 1. Patients with CVT were younger than those with VTE and controls and were mainly women, as CVT typically affects women in reproductive age. As expected, thrombophilia abnormalities were more frequent in patients than controls. Platelet, neutrophil, and lymphocyte mean count did not differ between groups as well as PLR and NLR median values, except for PLR was lower in patients with VTE than controls (P = .024). Single hematological parameters determining PLR or NLR, such as platelet, lymphocyte, and neutrophil count, did not influence the risk of VTE or CVT (data not shown).
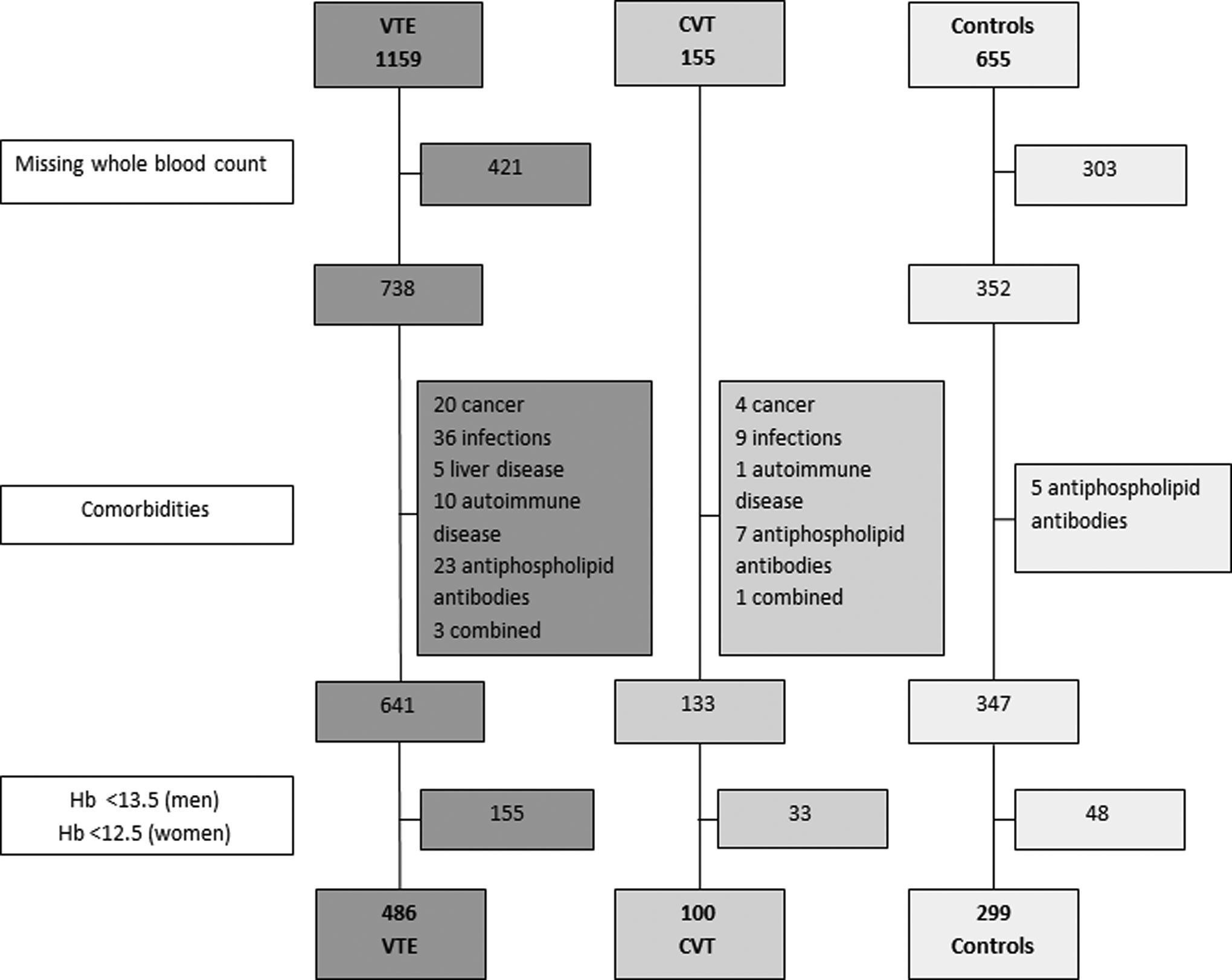
Selection of the study population.
Demographic and Clinical Characteristics of Patients With Venous Thromboembolism, Cerebral Venous Thrombosis, and Controls.
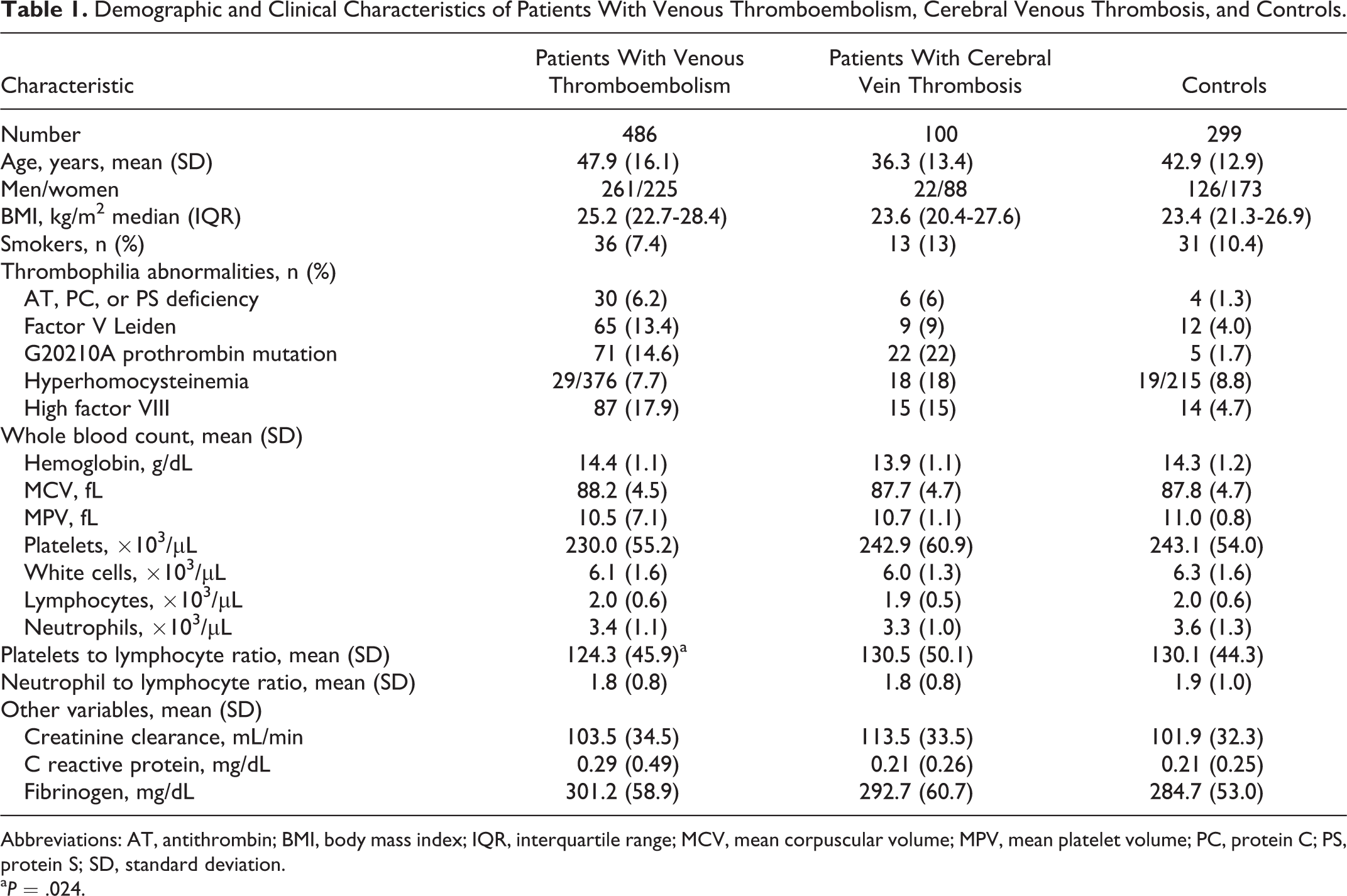
Abbreviations: AT, antithrombin; BMI, body mass index; IQR, interquartile range; MCV, mean corpuscular volume; MPV, mean platelet volume; PC, protein C; PS, protein S; SD, standard deviation.
aP = .024.
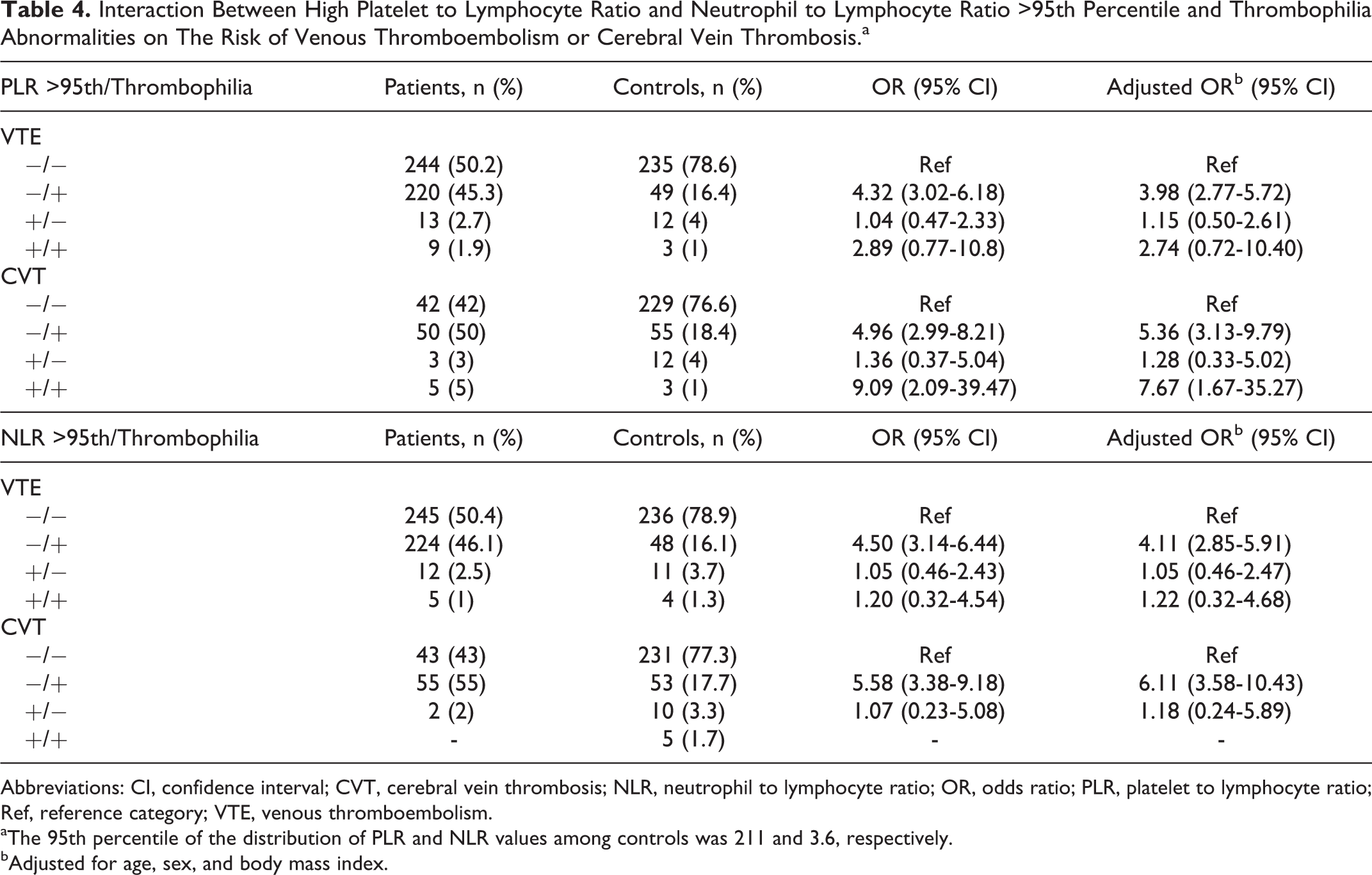
The risk of VTE or CVT was not increased with PLR >211 or NLR >3.6, corresponding to the 95th percentile of the distribution of values among controls (Table 2), also after adjustment for possible confounders. When provoked and unprovoked events were considered separately, high PLR values were associated with an increased risk of provoked CVT (adj. OR: 2.65, 95% CI: 1.02-6.92; Table 3), whereas high NLR values did not influence neither the risk of provoked nor unprovoked VTE or CVT. No association was observed when patients were divided into those with blood taken within (patients with 166 VTE and 14 CVT) and after (patients with 320 VTE and 86 CVT) 3 months from thrombosis (data not shown). Table 4 shows the interaction analysis of high PLR or NLR values and thrombophilia abnormalities. An interaction was observed only for high PLR values and thrombophilia in patients with CVT (adj. OR: 7.67, 95% CI: 1.67-35.27). This estimate is 30% greater than the expected risk in the absence of interaction between the 2 variables [(5.36 + 1.28)−1=5.64].
Risk of Venous Thromboembolism or Cerebral Vein Thrombosis for Strata of Platelet to Lymphocyte Ratio and Neutrophil to Lymphocyte Ratio.a
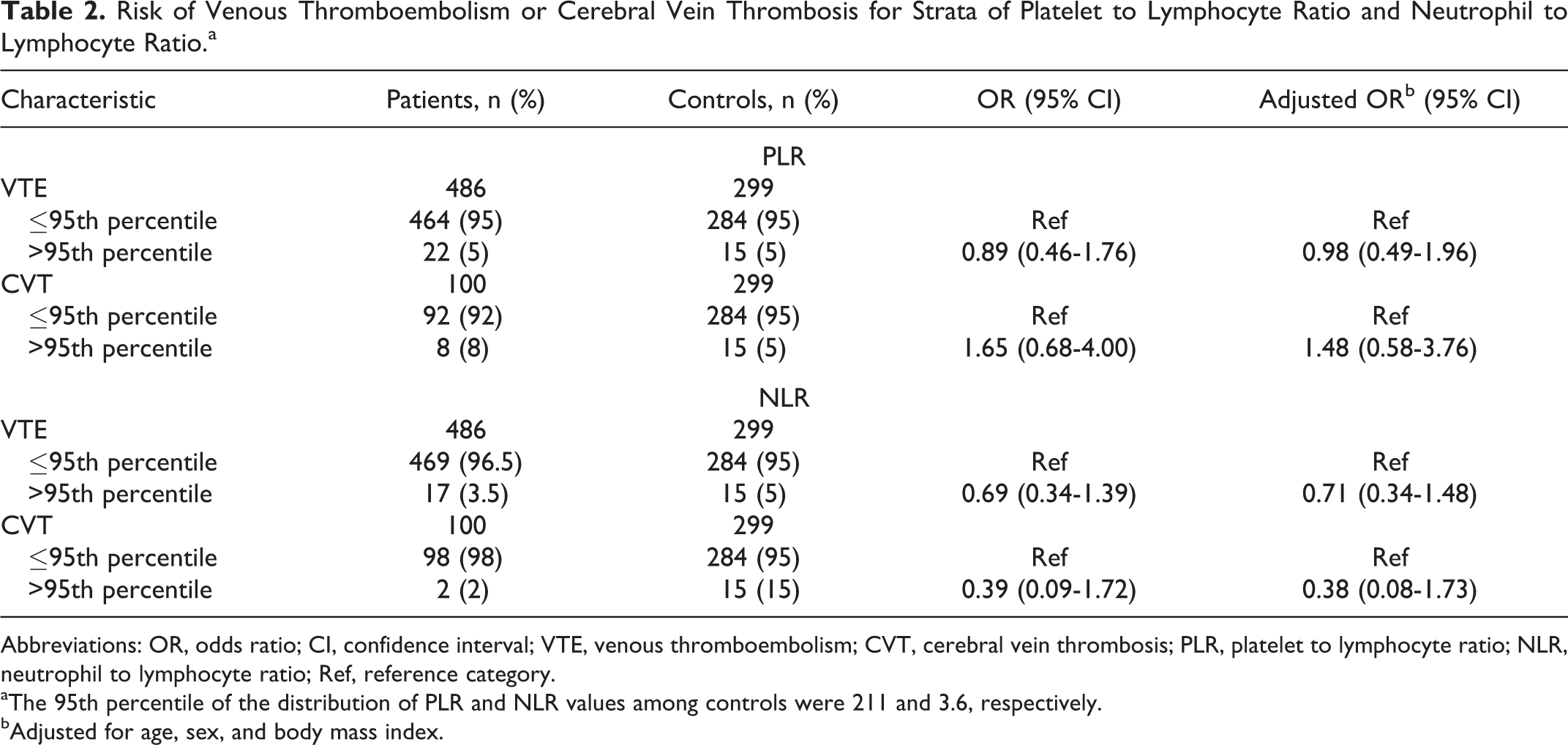
Abbreviations: OR, odds ratio; CI, confidence interval; VTE, venous thromboembolism; CVT, cerebral vein thrombosis; PLR, platelet to lymphocyte ratio; NLR, neutrophil to lymphocyte ratio; Ref, reference category.
aThe 95th percentile of the distribution of PLR and NLR values among controls were 211 and 3.6, respectively.
bAdjusted for age, sex, and body mass index.
Risk of Provoked or Unprovoked Venous Thromboembolism or Cerebral Vein Thrombosis for Platelet to Lymphocyte Ratio Above the 95th Percentile.a
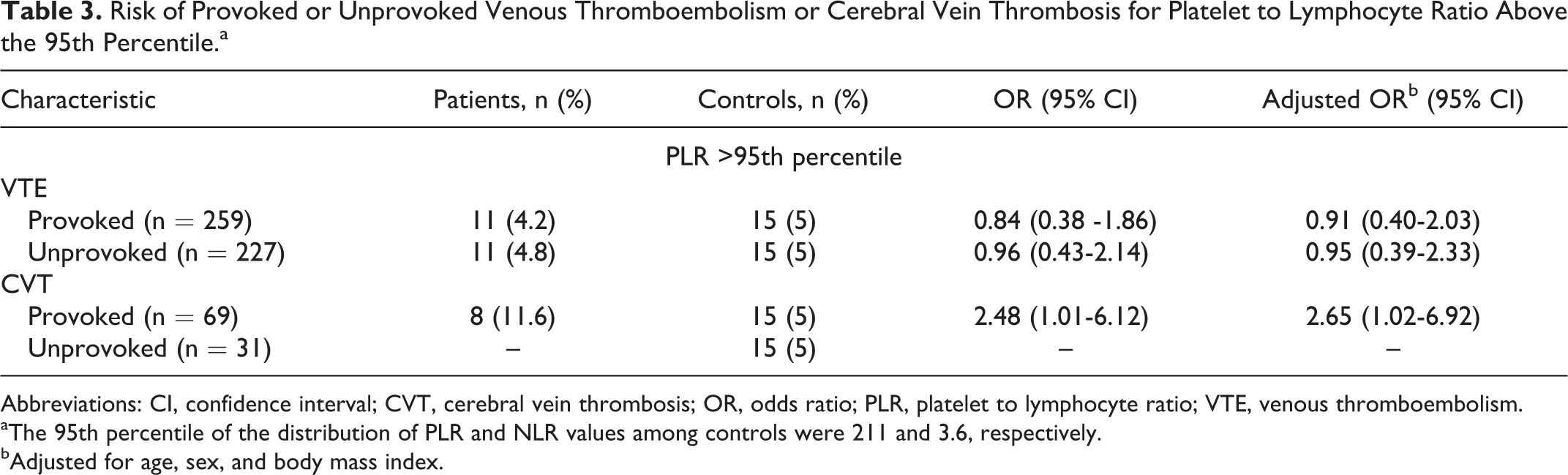
Abbreviations: CI, confidence interval; CVT, cerebral vein thrombosis; OR, odds ratio; PLR, platelet to lymphocyte ratio; VTE, venous thromboembolism.
aThe 95th percentile of the distribution of PLR and NLR values among controls were 211 and 3.6, respectively.
bAdjusted for age, sex, and body mass index.
Interaction Between High Platelet to Lymphocyte Ratio and Neutrophil to Lymphocyte Ratio >95th Percentile and Thrombophilia Abnormalities on The Risk of Venous Thromboembolism or Cerebral Vein Thrombosis.a
Abbreviations: CI, confidence interval; CVT, cerebral vein thrombosis; NLR, neutrophil to lymphocyte ratio; OR, odds ratio; PLR, platelet to lymphocyte ratio; Ref, reference category; VTE, venous thromboembolism.
aThe 95th percentile of the distribution of PLR and NLR values among controls was 211 and 3.6, respectively.
bAdjusted for age, sex, and body mass index.
Discussion
The identification of risk factors for venous thrombosis is important to optimize therapeutic and preventive measures in individuals at risk. Platelet to lymphocyte ratio and NLR are simple laboratory parameters easily obtained with the whole blood count and have the advantage to pool information about primary hemostasis and inflammation. Their prognostic value has been widely investigated in coronary artery 10,11 and cardiovascular 12,13 diseases To our knowledge, this is the first study aiming to investigate PLR and NLR as risk factors for VTE or CVT. The main finding is the lack of association between high values of PLR and NLR and an increased risk of venous thrombosis. The large sample allowed us to stratify the analysis for the presence or absence of transient risk factors for thrombosis, and a 3-fold increased risk of provoked CVT was found for high PLR values. Finally, an interaction between high PLR values and the presence of at least 1 marker of thrombophilia on the risk of CVT was observed.
In the past few years, several studies investigated the sequence of events linking inflammation to venous thrombosis. 4,25,26 An in vivo study identified a cross talk between monocytes, neutrophils, and platelets; neutrophils provide the initiating stimuli necessary for thrombus formation and platelets contribute to the propagation of venous thrombus. 27 A recent study in mouse model showed that platelets, neutrophils, and coagulation factor XII play a role in the pathophysiology of venous thrombosis. 3 Other than composing the majority of the arterial thrombus, aggregates of platelets are located in the core of the venous thrombus. 28 Indeed, a high platelet count is strongly associated with an increased risk of VTE 5,29 and, in response to prohemostatic stimuli, platelets generate circulating microparticles that are an independent risk factor for VTE. 30 Concerning neutrophils, they get entrapped in the growing thrombus and, through the extrusion of neutrophils extracellular traps , are able to recruit other cells that are active in the coagulation cascade, especially in venous valves where the flow is minimal. 25 Neutrophilia, when persistent over a 3-year period, has been associated with an increased risk of VTE in patients with such comorbidities as heart, liver, or renal diseases. 31 In addition, leukocytosis influences the thrombotic risk in patients with myeloproliferative neoplasms, 32 and high PLR and NLR values enhance the risk of cancer-related VTE. 29,33,34 Despite the growing evidence supporting the hypothesis of the role of platelets, leucocytes, and neutrophils in thrombus formation, we were not able to demonstrate an association between high PLR or NLR values and the risk of VTE or CVT. The 3-fold increased risk of CVT for high PLR but not NLR values is consistent with other studies in patients with VTE 33 or prosthetic valves thrombosis. 35
Some limitations of this study need to be addressed. First, about one-third of patients with VTE or CVT and half controls were excluded from the analysis because the information on blood count was missing. This could have reduced the power of the study, but not the main conclusion on the lack of association between high PLR or NLR values and venous thrombosis, since missing data were random and increasing sample size would have only improved the precision, but not the size of the risk estimate. Second, although this is a large sample of CVT patients from a single Center, it remains relatively small because of the rarity of the disease. Hence, a weak effect of high PLR and NLR values on the risk of VTE cannot be excluded, and further data possibly stemming from prospective studies are warranted. Third, whether high PLR or NLR values are causally related to thrombosis in particular subgroups of patients or are a mere epiphenomenon of the acute phase is still to be elucidated. It can be speculated that in the presence of other major risk factors in brain vessels, activated platelets might enhance the thrombotic risk, especially in the presence of thrombophilia abnormalities. Moreover, the PLR and NLR values assessed 3 months after the thrombotic event could have led to an underestimation of the association, but the lack of association between thrombosis and PLR and NLR values measured in the acute phase (ie, within 3 months from the event) makes unlikely a possible causal relationship, although the number of patients in the subgroup analysis was further reduced, particularly for CVT. Finally, being our Thrombosis Center, a tertiary care center where patients are referred for thrombophilia work-up, our population might not be representative of the general population of patients with VTE or CVT nor can be generalized to arterial thrombosis. In conclusion, our study may not support high PLR and NLR values as risk factors for VTE. Whether high PLR values have a role in provoked CVT, particularly in patients with thrombophilia abnormalities, remains to be confirmed by further observations, considering the exploratory nature of this study.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.