
Abstract
Differences in warfarin maintenance dosages based on the presence of polymorphisms in VKORC1, CYP2C9, CYP4F2, and ORM1 can be determined through dosage adjustment according to routine guidelines. Little is known about whether routine therapy could provide consensus anticoagulation control for patients with different genotypes. This study was carried out to compare anticoagulant control in patients with different genotypes. Six hundred seventy patients using warfarin according to Chinese guidelines were enrolled. Warfarin dosages and monitored international normalized ratios (INRs) were recorded. Genotypes of VKORC1 rs9923231, CYP4F2 rs2108622, CYP2C9 rs1057910, and ORM1 rs17650 polymorphisms were determined. Warfarin dosages and INR were compared between genotypes. Patients with the AGCC*F*F*1*1 polymorphism took longer than patients with the AACC*F*F*1*1 polymorphism (20 vs 5 days, P < .001) to achieve the targeted INR range. The INR values of patients with AACC*F*F*1*3 were unstable and did not enter the stable state control phase until after 35 days. The peak INR of patients with the AACC*F*F*1*3 polymorphism was exceedingly high, with some values exceeding the control range limit of 3.0. Patients with the AACC*F*S*1*1 or AACT*F*F*1*1 polymorphisms exhibited similar INR values as the patients with the AACC*F*F*1*1 polymorphism. This study found that routine medication with warfarin provides significantly different levels of anticoagulant control between patients with wild-type genotypes and patients with heterozygous polymorphism genotypes of VKORC1 rs9923231 or CYP2C9 rs1057910. Patients with heterozygous polymorphism genotypes of VKORC1 or CYP2C9 require genotype-directed therapy with warfarin to increase efficacy and safety in anticoagulant treatment.
Introduction
Warfarin is the most commonly used oral anticoagulant by patients with atrial fibrillation, artificial heart valves, deep venous thrombosis, and pulmonary embolism. Although periodically monitored, the prothrombin time, the international normalized ratio (INR), and the practical dosage of warfarin used must be adjusted accordingly to ensure an effective and safe therapy. 1 –3 Warfarin has been reported to be one of the top 10 drugs with the largest number of serious adverse events. 4 –6 The clinical use of warfarin is very complicated because it has a narrow therapeutic index and large person-to-person variation in clinical response. The largest reported difference in effective stable dosages of warfarin among patients was more than 10-fold. 7
Genetic variations were reported to be the most important factor affecting warfarin therapy response among all possible variable factors, such as age, gender, and weight. Polymorphisms of VKORC1 rs9923231 and CYP2C9 rs1057910 were found to account for approximately 30% of dosage variation. 8 The CYP4F2 rs2108622 polymorphism was reported to cause 2% to 7% of dosage variation, and the ORM1 rs17650 polymorphism accounted for 2% of dosage differences according to our early findings. 9 Based on numerous published reports, the Food and Drug Administration has suggested practicing genotype-guided (pharmacogenetically based) dosing for anticoagulation control with warfarin. 10 However, Kimmel et al found that genotype-guided dosing of warfarin did not improve anticoagulation control. 11 However, the study by Pirmohamed et al found that pharmacogenetic-based dosing was associated with a higher percentage of time in the therapeutic INR range than was standard dosing during initial warfarin therapy. 12 These inconsistent conclusions reflect the imperfect nature of gene-directed therapeutic methods.
Warfarin stable dosage differences between genotypes can usually be matched by the practice of routine dosage adjustment in clinical therapy. We carried out this study to observe whether routine therapeutic warfarin treatment could produce consensus anticoagulant control in patients with different heterozygous polymorphisms of VKORC1, CYP2C9, CYP4F2, and ORM1.
Methods
Participants
A total of 670 patients were enrolled in this study from October 2013 to December 2014 after signing an informed consent form. The patients began anticoagulant therapy with warfarin according to Chinese guidelines after a heart valve replacement operation. They began warfarin therapy at a daily dosage of 2.5 mg. Dosage adjustments were made to maintain their INR values within 2.0 to 3.0. Five percent to 20% dosages were recommended to be added or decreased when the monitored values of INR were distributed outside the target range and when their doctors thank dosage adjustment necessary by their clinical experience. 13
Patients were excluded from the study if they were pregnant or if they had cancer, a history of severe bleeding, heart failure, cardiomyopathy, or diseases related to blood coagulation. They were also excluded for concomitant administration of medications that were reported to interact with warfarin and/or were reported to affect the coagulation process. This study was approved by the ethics committee of the Institute of Clinical Pharmacology at Central South University (Changsha, Hunan, China).
Study Design
Genotypes for VKORC1 rs9923231 and CYP2C9 rs1057910 were determined by using a pyrosequencing method as described previously, 9 and genotypes for CYP4F2 rs2108622 and ORM1 rs17650 were determined through a Polymerase Chain Reaction (PCR)-restriction fragment length polymorphism method as described previously. 9 The CYP4F2 rs2108622 genotypes were differentiated using PvuII enzyme restriction digestion. The ORM1 rs17650 genotypes were differentiated using EcoNI enzyme restriction digestion. PCR primers are listed as follows. VKORC1: forward primer: 5′-TGTTGGCCAGGCTTGTCTTAAACT-3′, reverse primer: 5′-biotin-CCAGAAG-GGTAGGTGCAACAGTA-3′; CYP2C9: forward primer: 5′-biotin-ATGCAAGACAGGAGCCACATG-3′, reverse primer: 5′-GGGACTTCGAAAACATGGAGT-TG-3′; CYP4F2: forward primer: 5′-TGAGGGAGGTGATGTTGGATACTCCTG-3′, reverse primer: 5′-TGAAGGAGGCCTTCTCCTGACTGCT-3′; ORM1: forward primer: 5′-GAACTGAATCTATGTTTGTCTTCC-3′, reverse primer: 5′-CGACCACAGCCAGCAGGG-3′. All genotype results were confirmed by double-blind detection.
International normalized ratio values were determined every day in the first 7 days, every week in the first 30 days, and then every month. Values of INR within 30 days and stable state warfarin dosages (2.0 > INR < 3.0) were recorded and compared between groups of patients with different genotypes.
Statistical Analysis
The results are presented as the means (standard deviation; SD). Gene allelic frequencies were calculated by the numbers of specific alleles, and genotype frequencies for all polymorphic genes were tested for deviation from Hardy-Weinberg equilibrium by χ2 goodness-of-fit analysis. Differences between groups were detected using the Mann-Whitney U test or the H test of Kruskal and Wallis, as appropriate. Associations between INR and age, weight, height, and valve types were evaluated using nonparametric partial correlation. Stepwise linear regression was performed to model the relationships between warfarin dosage and other variables measured and was used to develop a novel warfarin dosing algorithm. Survival analysis for patients without INR values with which to target the therapeutic range was performed using the Kaplan-Meier method. Data analysis was performed on SPSS 17.0 for Windows (SPSS Inc, Chicago, Illinois). A P value of less than .05 was considered to be statistically significant.
Results
A total of 670 patients were enrolled in this study. The mean age of these patients was 47.6 (11.2) years (range 15-73 years). Of the patients, 256 (38.2%) were male. All patients began warfarin therapy after an artificial valve replacement operation. Stable state therapy with warfarin was defined as the state when the INR of a patient had been successfully controlled to remain within the range of 2.0 to 3.0 with a stable daily warfarin dose for 3 months or longer.
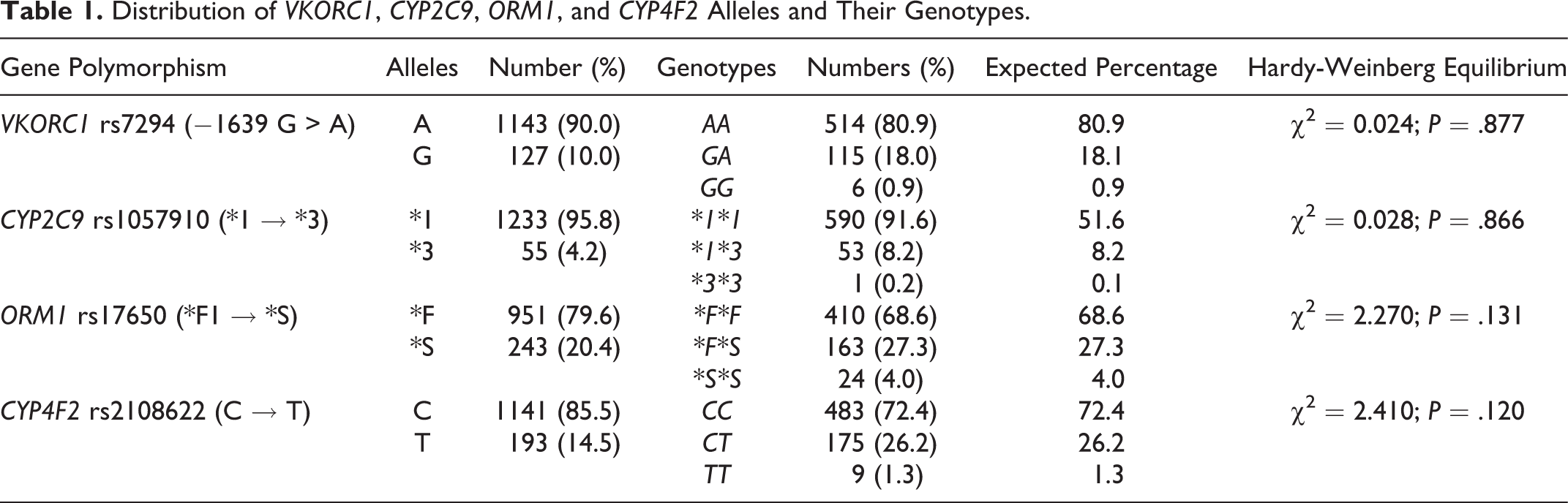
As shown in Table 1, polymorphisms of VKORC1 rs9923231, CYP2C9 rs1057910, and ORM1 rs17650 were all distributed in accordance with Hardy-Weinberg equilibrium, with their minor allele frequencies of 10.0%, 4.2%, 20.4%, and 14.5%, respectively.
Distribution of VKORC1, CYP2C9, ORM1, and CYP4F2 Alleles and Their Genotypes.
As shown in Table 2, warfarin stable dosages of 191 patients with wild-type genotypes and 4 heterozygous genotypes were found to be partially correlated with VKORC1 rs9923231, CYP2C9 rs1057910, and ORM1 rs17650 genotypes and with gender. Combined contribution of VKORC1 rs9923231, CYP2C9 rs1057910, and ORM1 rs17650 polymorphisms to dosage variation was 14.8%. Box plot distributions of warfarin dosage taken by patients with wild-type genotypes and heterozygous polymorphism genotypes of VKORC1 rs9923231, CYP2C9 rs1057910, ORM1 rs17650, and CYP4F2 rs2108622 are shown in Figure 1.
A Model of Warfarin Dosage Regression Equations Based on Age, Weight, Height, Sex, and Genotypes of CYP2C9, VKORC1, CYP4F2, and ORM1.a,b,c
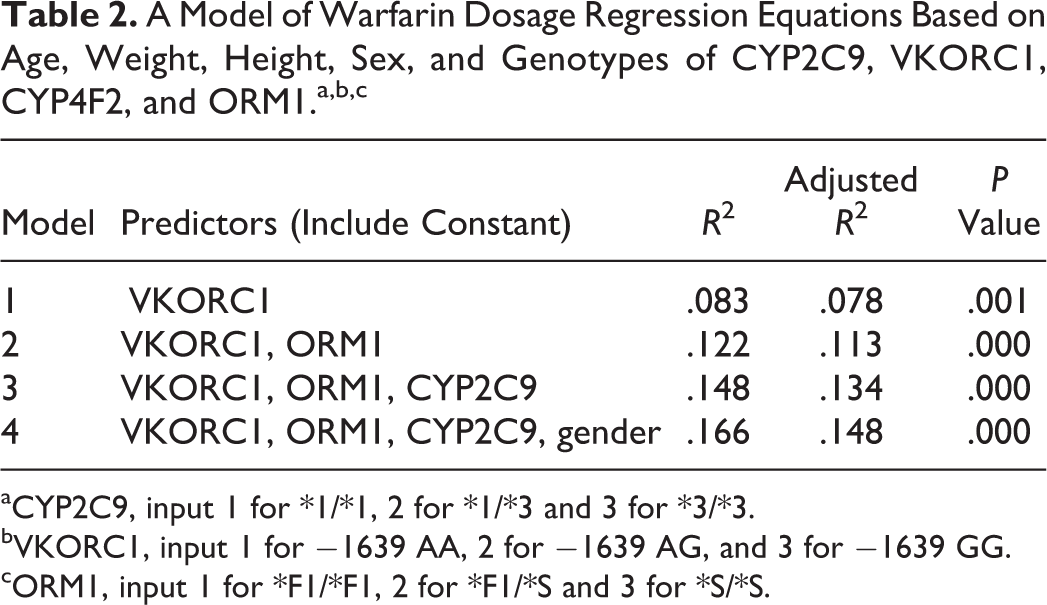
aCYP2C9, input 1 for *1/*1, 2 for *1/*3 and 3 for *3/*3.
bVKORC1, input 1 for −1639 AA, 2 for −1639 AG, and 3 for −1639 GG.
cORM1, input 1 for *F1/*F1, 2 for *F1/*S and 3 for *S/*S.
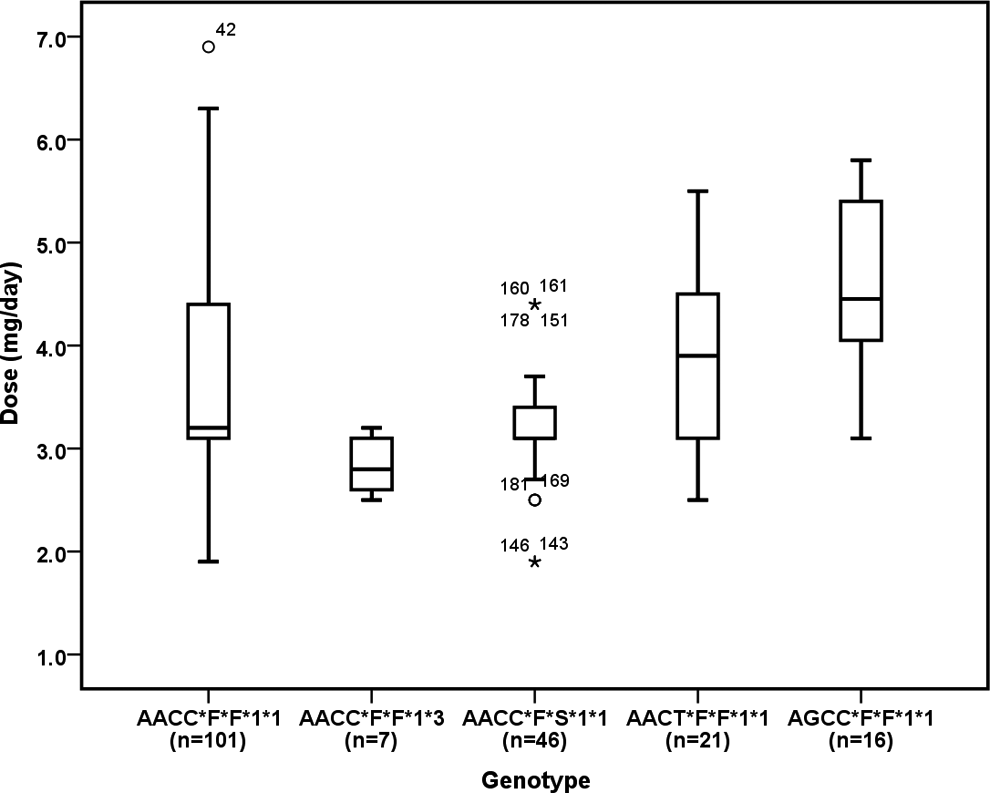
Box plot distributions of warfarin dosage taken by patients with wild-type genotype and heterozygous polymorphism genotypes of CYP2C9 rs1057910, ORM1 rs17650, CYP4F2 rs2108622, and VKORC1 rs9923231. Boxes: median and interquartile range of the 25th to 75th percentiles, vertical lines above and below boxes: maximum and minimum values, respectively. The maximum length of each whisker is 1.5 times the interquartile range. Each outlier is denoted with a circle and a data number.
Demographics, warfarin daily doses, and P values of comparisons between patients with wild-type genotypes and heterozygous polymorphism genotypes of 4 polymorphic genes are shown in Table 3. At the warfarin therapy stable state condition, there were significant differences in warfarin maintenance dosage between patients with wild-type genotypes and patients with heterozygous polymorphism genotypes of VKORC1 rs9923231 (P = .001), CYP2C9 rs1057910 (P = .022), and ORM1 rs17650 (P = .003; Tables 2 and 3). Patients with heterozygous polymorphism genotypes of CYP4F2 rs2108622 required a dosage similar to that of wild-type patients (P = .577).
Demographics, Warfarin Daily doses, and P Values of Comparisons Between Patients With Wild-Type Genotypes and Heterozygous Polymorphism Genotypes.
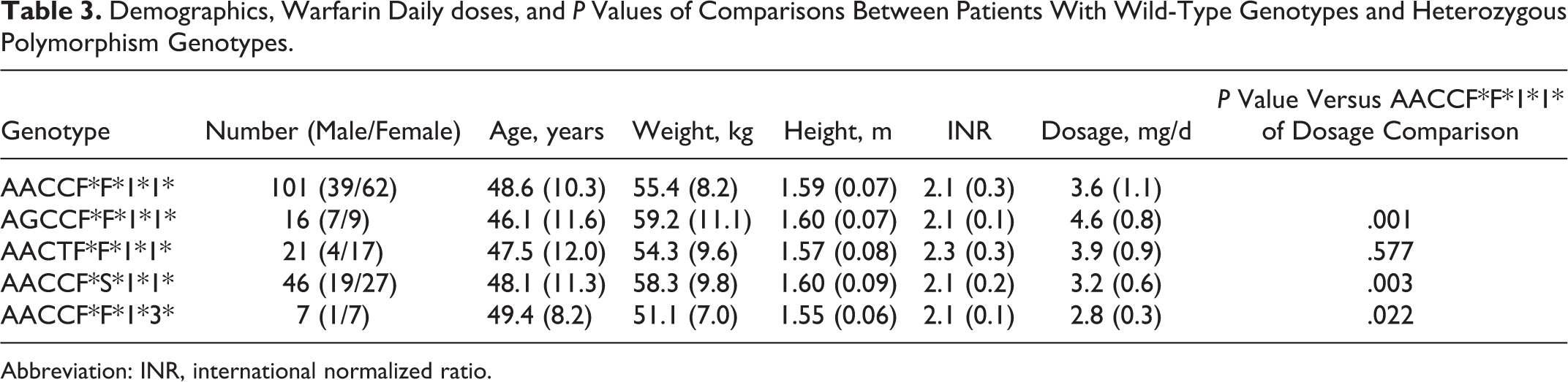
Abbreviation: INR, international normalized ratio.
Comparisons of anticoagulant control between patients with wild-type genotypes and heterozygous polymorphism genotypes of 4 polymorphic genes are shown in Figures 2 and 3. The INR curves of patients with heterozygous polymorphism genotypes of VKORC1 rs9923231 and CYP2C9 rs1057910 were significantly different from that of the patients with wild-type genotypes. We found that the patients with heterozygous polymorphism genotypes of ORM1 rs17650 and CYP4F2 rs2108622 exhibited an INR curve almost overlapping on that of the patients with wild-type genotypes. There were significant difference in the proportion of patients who did not reach the target INR therapeutic range between patients with the wild-type genotype and the heterozygous polymorphism genotypes of VKORC1 rs9923231 (P < .001), CYP2C9 rs1057910 (P = .003), and CYP4F2 rs2108622 (P < .001).
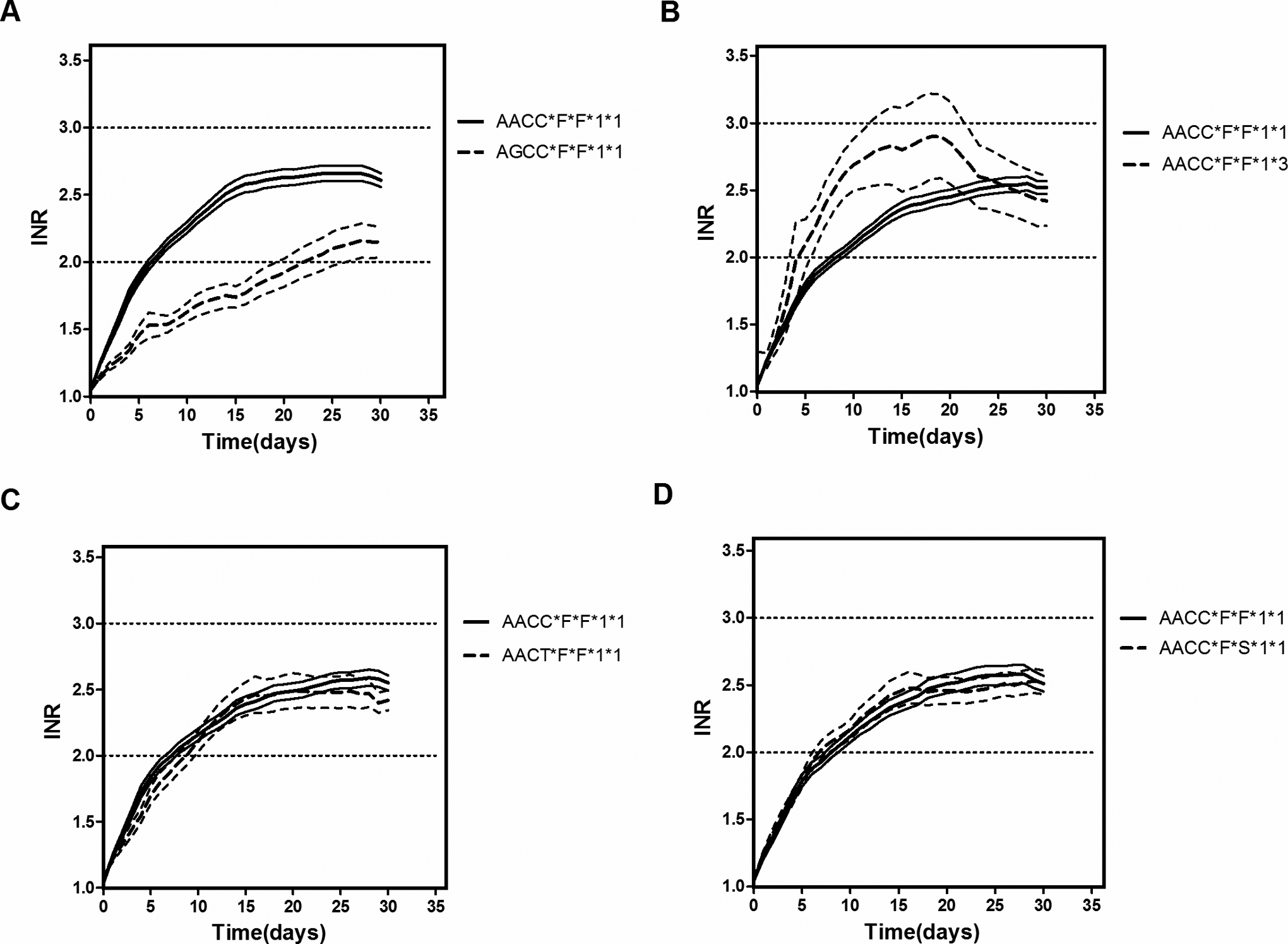
Comparison of the curves of INR between patients with wild-type genotype and heterozygous polymorphism genotypes of VKORC1 rs9923231 (A), CYP2C9 rs1057910 (B), CYP4F2 rs2108622 (C), and ORM1 rs17650 (D).
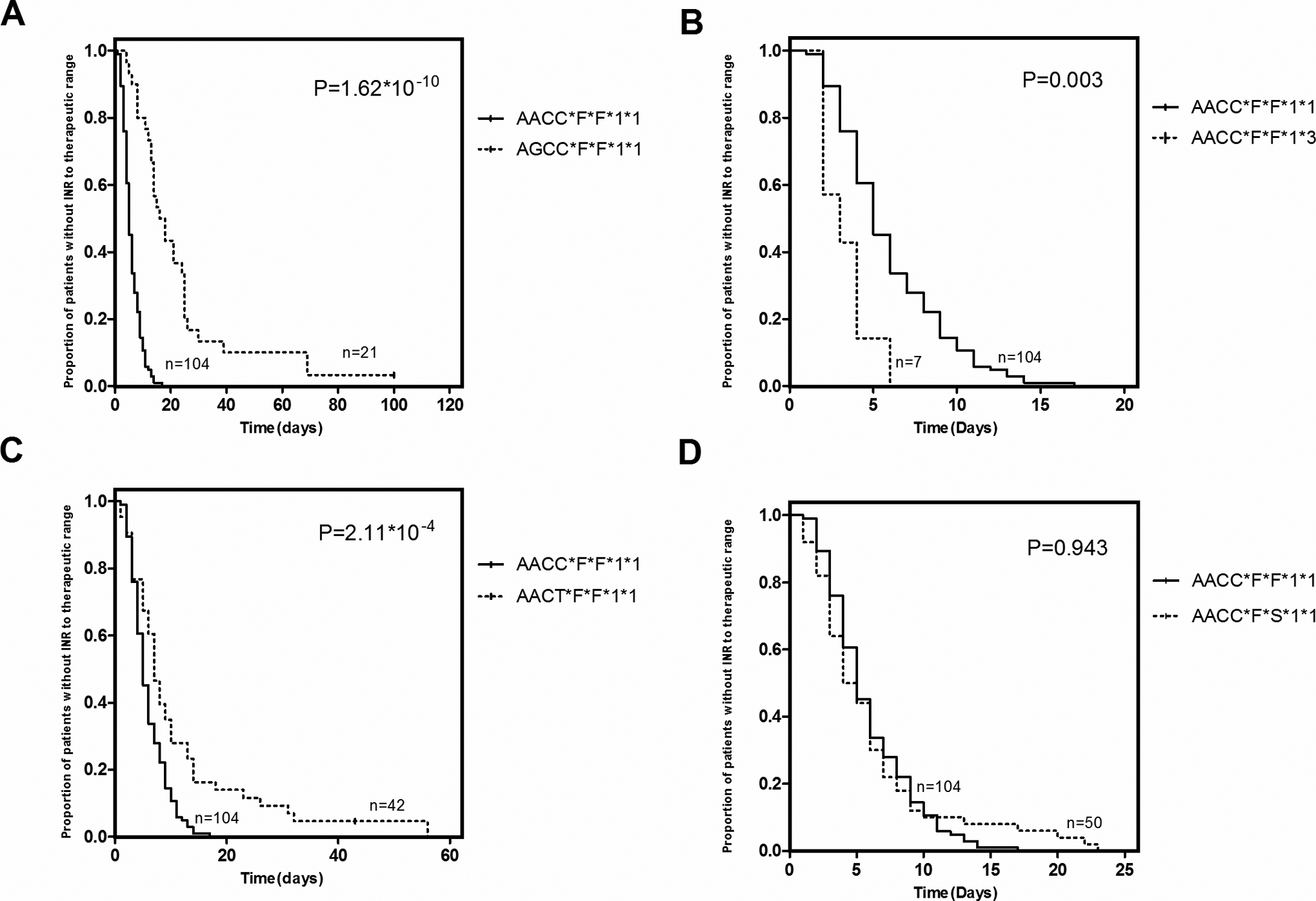
Comparison of the proportion of patients who did not reach the target INR therapeutic range between patients with wild-type genotype and heterozygous polymorphism genotypes of VKORC1 rs9923231 (A), CYP2C9 rs1057910 (B), CYP4F2 rs2108622 (C), and ORM1 rs17650(D).
Discussion
All participants in this study began anticoagulant therapy in accordance with the guidelines for warfarin treatment of Chinese patients. 13 In line with previous findings, 8,9 there were significant differences in warfarin maintenance dosage between patients with wild-type genotypes and patients with heterozygous polymorphism genotypes of VKORC1 rs9923231, CYP2C9 rs1057910, and ORM1 rs17650 (Table 3). Patients with heterozygous polymorphism genotypes of CYP4F2 rs2108622 required a dosage similar to that of wild-type patients. In this study, participants with homozygous genotype for the minor allele and participants with variant allele of 2 or more genes were excluded in data analyzed. Therefore, combined contribution of VKORC1 rs9923231, CYP2C9 rs1057910, and ORM1 rs17650 polymorphisms to dosage variation in this study with a narrow participant population of specific genotypes was lower than those in our early study (14.8% vs 25.3%). 9 According to the INR records for our data (Figure 2), current warfarin treatment practices provided effective and safe anticoagulant therapy for the patients with wild-type genotypes in the first month. The INR of these patients rose quickly and remained steady within the target range. It took 5 days, on average, for wild-type patients to achieve effective anticoagulant control. 14 At the same time, in the first month of warfarin treatment, INR values were above 3.0 for only 5% of wild-type patients’ total therapeutic time.
However, for the patients with the heterozygous polymorphism genotype VKORC1 rs9923231, current warfarin therapy was shown to provide poor INR control (Figure 2A). The INR values of patients with the VKORC1 rs9923231 polymorphism were significantly lower than those of patients with wild-type genotypes. It took patients with the VKORC1 rs9923231 polymorphism 20 days on average to achieve INR values in the target range, which is 4 times long as it took for patients with the wild-type genotype. There was a significant difference in the proportion of patients with the heterozygous polymorphism genotype of VKORC1 rs9923231 in reaching the target INR range compared to patients with the wild-type genotype (Figure 3A). There were several inflection points during the INR rising phase for patients with the VKORC1 rs9923231 polymorphism that were signs of dosage adjustment, but these dosage adjustments clearly did not effectively lead to the INR reaching the target range rapidly. The final INR values for patients with the VKORC1 rs9923231 polymorphism stabilized on the lower side of the therapeutic range, which was still significantly lower than the INR values of the wild-type genotype patients. VKORC1 is the drug target of warfarin. The presence of the rs9923231 polymorphism seriously impaired the function of VKORC1 and led to resistance to warfarin. 15,16 Patients with the rs9923231 G allele may have a different dosage versus effect relationship than wild-type patients. Therefore, these patients need a larger initiation dosage to affect anticoagulant time, and they may also need a larger dosage adjustment than the current routine dosage adjustment to bring an abnormal INR value into the target range.
International normalized ratio control in patients with the 1*/3* genotype was also shown to be unsuccessful using the routine model of warfarin administration (Figure 2B). The INR curve of these patients was unstable, with largest fluctuation in amplitude occurring in patients with different genotypes. The peak INR was significantly higher in patients with the 1*/3* genotype than in patients with the wild-type genotype, with the INR values of some patients reaching above the upper limit of 3.0. The INR curve of patients with the 1*/3* genotype lacks a platform phase until after 35 days, the longest of the groups analyzed. The inflection points in the INR curve of patients with the 1*/3* genotype indicated that these patients experienced several dosage adjustments. However, these dosage adjustments clearly did not effectively lead to a stable state INR value in the targeted INR range. CYP2C9 is the major elimination enzyme of warfarin, and the CYP2C9 rs1057910 mutation significantly impaired the activity of CYP2C9. Patients with the 1*/3* genotype had a lower elimination rate and displayed hypersensitivity to warfarin compared to wild-type patients. 17 Therefore, these patients need a lower initiation dosage to begin warfarin therapy to avoid some of the effects of overtreatment with an anticoagulant, and these patients also need to be dosage adjusted with a smaller dosage adjustment than the current routine to modify an abnormal INR value.
CYP4F2 is a vitamin K1 metabolic enzyme. The rs2108622 polymorphism impaired the enzyme activity of CYP4F2 and led to elevated hepatic vitamin K1 levels, which caused an increased warfarin dosage requirement to elicit the same anticoagulant response in warfarin therapy. 18 –20 We found that it took 2 days longer on average for patients with the CYP4F2 rs2108622 mutation to reach the target INR range. There was a significant difference in the proportion of patients with the CYP4F2 rs2108622 mutation that did not reach the target INR range compared to patients with the wild-type genotype (Figure 3C). Additionally, patients with the CYP4F2 rs2108622 CT genotype displayed a similar INR curve to patients with the wild-type genotype. Generally, other anticoagulant measures in addition to warfarin therapy are utilized during the first 7 days in the hospital for patients after heart valve replacement operations. Therefore, the 2-day delay to enter the INR target range within the initial 7 days of hospitalization did not affect clinical therapy. Therefore, the current practice of warfarin administration was suitable for patients with the CYP4F2 rs2108622 CT genotype. There was no need to perform genotype-directed therapy for patients with the CYP4F2 rs2108622 CT genotype. However, whether this conclusion still stands for the patients with the TT genotype remains to be elucidated.
ORM1 rs17650 is another polymorphism affecting warfarin dosage requirements. ORM1 *S carriers require lower maintenance dosages to achieve and maintain an optimal level of anticoagulation. We found that the patients with the *F*S genotype exhibited an INR curve almost overlapping on that of the patients with the *F*F genotype. In addition, there was no significant difference in the time to first INR in the therapeutic range or in the time spent above the target INR between patients with the *F*S genotype or the *F*F genotype. Together, these data indicate that the current therapeutic model of warfarin administration was suitable for the patients with the *F*S genotype. However, this conclusion did not stand for patients with the *S*S genotype because our early study found that some of these patients were hypersensitive to warfarin and needed a lower initial dosage for therapy.
In conclusion, this study found that the current model of empirical medication with warfarin provides consensus anticoagulant control between patients with wild-type genotypes and patients with the heterozygous polymorphism genotypes of CYP4F2 rs2108622 and ORM1 rs17650 and provides significantly different anticoagulant control between patients with wild-type genotype and patients with the heterozygous polymorphism genotypes of VKORC1 rs9923231 and CYP2C9 rs1057910. Patients with the mutations VKORC1 rs9923231 or CYP2C9 rs1057910 require genotype-directed therapy with warfarin to optimize efficacy and safety.
Footnotes
Authors’ Note
Hai He Jiang and Jia Liu contributed equally to this work. Lian Sheng Wang designed this study and organized the research. Hai He Jiang recruited the patients and wrote the paper. Jia Liu performed the major part of the research and analyzed data. Yi Chen Wang recruited participants. Hui Ming Ye analyzed data and provided advice. Xi Li performed statistical analysis. Wei Zhang gave advice.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Natural Science Foundation of China grants 81072707, 81472031, and 81503563.