
Abstract
Long-term anticoagulation in patients with metallic prosthetic valve disease is required according to current guidelines. We describe a patient with a functioning mitral mechanical valve without anticoagulation for 27 years. A 46-year-old man admitted to the emergency department with complains of palpitation. The patient had a mitral valve replacement because of severe mitral stenosis. He discontinued warfarin treatment 1 month after surgery because of the unavailability of this drug in Turkey. Transthoracic echocardiography revealed functioning metalic mitral valve with a mean gradient of 9 mm Hg. Fluoroscopy showed normal excursions of the mechanical mitral valve. Transesophageal echocardiography was performed and revealed fresh thrombus formation in the left atrial appendix. Admission international normalized ration (INR) level was 1.79. Due to the higher INR level and long-term survival, genetic analysis of warfarin polymorphism was performed. There was a homozygous mutation in the vitamin K epoxide reductase complex 1 (VKORC1) 1173C>T and 1639G>A genotypes. The possible explanations of long-term survival and baseline higher INR level were linked to the mutation in warfarin metabolism. We also briefly review the literature.
Keywords
Introduction
Anticoagulation is necessary and vital for mechanical heart valves to prevent thromboembolic complications, which may also cause fatal bleedings. 1 Although survival without anticoagulation has been reported before, it is of utmost importance that patients with a metallic mitral valve are at increased risk of lethal complications, such as valve thrombosis and systemic embolism, when they are without anticoagulation. 1 The cause of long-term survival without anticoagulation has not been well explained in previous reports. In this article, we analyzed warfarin gene polymorphism and found a mutation in the vitamin K epoxide reductase complex (VKORC1) locus which points to a coagulation abnormality. Warfarin gene polymorphism is very important in either cases with warfarin overdose to reduce the dosage or warfarin resistance to increase dosage.
The conversion of inactivated vitamin K to the reduced form of vitamin K (activated) is carried out by vitamin K epoxide reductase (VKOR). Warfarin inhibits VKOR, resulting in less activated vitamin K. In cases with VKORC1 mutation, warfarin could not inhibit VKOR and result in inactivation of coagulation process.
Case Report
A 46-year-old man presented at the emergency department (ED) with complains of palpitations. He has no previous history of diabetes mellitus, hypertension, or usage of any medication and smoking. He underwent mitral valve replacement (St Jude Medical) prior to 27 years because of severe mitral stenosis. Although he was recommended warfarin, due to the unavailability of this drug in Turkey, he had no anticoagulation since then.
The patient’s initial physical examination was normal and the sound of the prosthetic valve was audible. His functional capacity was class I, according to the New York Heart Association functional classification. His blood pressure was 110/70 mm Hg, with an irregular heart rate of 112 beats/min. The 12-lead electrocardiography revealed atrial fibrillation with a rapid ventricular response.
The hemoglobin level was12.2 g/dL, hematocrite was 38.1%, and white blood cell count (WBC) was 6010/mm3. The biochemical investigation was within normal limits. Thyroid functional tests and cardiac enzymes including troponin I and creatine kinase-MB were also normal. Baseline international normalized ratio (INR) was 1.79.
Transthoracic echocardiography was performed and revealed normal left ventricular systolic and diastolic function. The peak and mean pressures of mitral prosthesis were measured as 16 and 9 mm Hg, respectively using Doppler echocardiography. There were no findings of thrombus or pannus formation in the metallic mitral valve. Pulmonary arterial pressure was measured as 35 mm Hg. Although the patient was recommended direct current cardioversion for atrial fibrillation, the process was omitted because of thrombus formation in the left atrial appendix revealed by transesophageal echocardiography (Figure 1). He was immediately initiated with 5 mg warfarin daily. Fluoroscopy showed normal motion of the mitral valve prosthesis. Due to the baseline higher INR level and long-term survival, genetic analysis of warfarin polymorphism was performed, which identified a homozygous mutation in the VKORC1 1173C>T and 1639G>A genotypes. After warfarin initiation, INR level was increased to 2.77 and the patient was discharged after 3 days of admission on warfarin 5 mg daily.
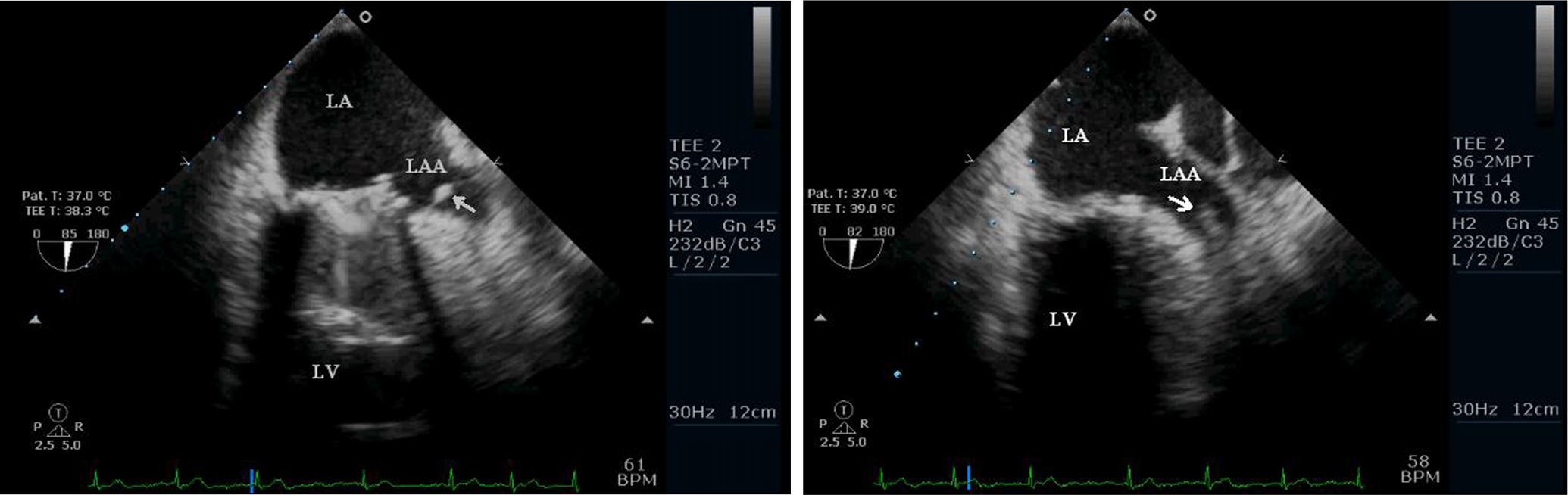
Transesophageal echocardiograms of normal mitral prostheses. Note the thrombus (arrow) in the left atrial appendix. LV indicates left ventricle; LA, left atrium; LAA; left atrial appendix.
Discussion
Prosthetic valve thrombosis is a well-known complication of mechanical valves and requires the patient to use long-term anticoagulation therapy. 1 In particular, prosthetic mitral valve has much worse survival rates without embolic episodes than those aortic valve. 2 These complications occur most frequently in the first 6 months after operation.
Some reports in the literature demonstrated cases with no anticoagulation in the long term without significant embolic events. Most of the reported cases involved an aortic metallic valve and it is well known that a prosthetic aortic valve has much better chances of survival without embolic events than the mitral valve. 2 To the best of our knowledge, there are 6 cases of aortic,3–8 2 cases of mitral,9–10 and 1 case of tricuspid prosthetic valve 11 without embolic episodes who were not under anticoagulation treatment in the literature (Table 1 ). The protection of these valves thus far has been reported as unknown and the potential factors underlying the normal valvular mechanics in these patients are still unknown. Furthermore, Perez-Zaldivar et al 10 contributed a long-term survival without anticoagulation to the “good luck” of the patient. Our case differs from the previous reports in 3 aspects. First, this case showed the longest survival in a human with a prosthetic mitral valve. In the case of Perez-Zaldivar and colleagues, survival without anticoagulation was 10 years in patients with metallic mitral valve. 12 Second, in contrast to the previous cases, we first demonstrated a genetic mutation in the coagulation cascade, which may contribute to and explain long-term survival with no anticoagulation. Thus, this mutation may be attributed to the so-called good luck of our patient. Third, previous cases reported survival without any systemic or local complications. Only, 1 case examined by Perez-Zaldivar et al 10 presented with an embolism in the cerebellum. However, our patient presented with thrombus in the left atrial appendix, and we think that this is “the end of good luck.”
Reported Cases with Mechanical Heart Valves Without Anticoagulation Therapy
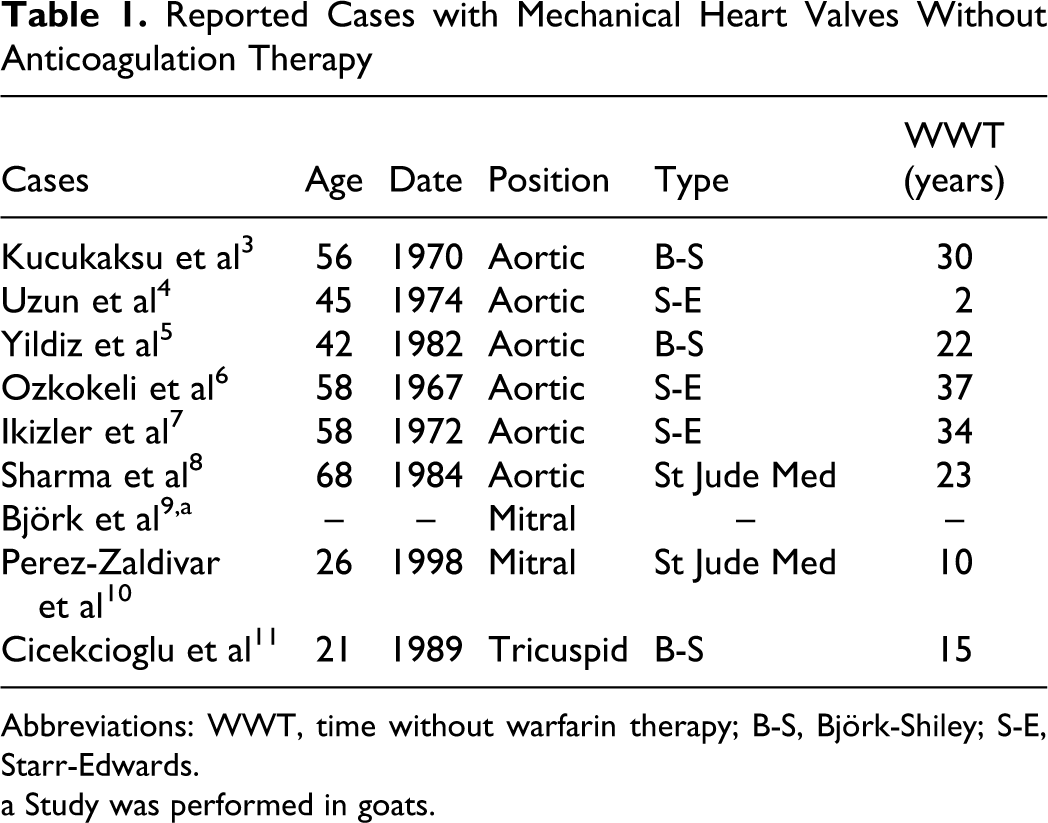
Abbreviations: WWT, time without warfarin therapy; B-S, Björk-Shiley; S-E, Starr-Edwards.
a Study was performed in goats.
Genetic polymorphisms can affect an individual’s response to pharmacologic agents. Increasing evidence suggests that genetic variations of CYP2C9 and VKORC1 greatly influences effective warfarin dose. 12 Vitamin K epoxide reductase is the target enzyme of warfarin and encoded by VKORC1 gene. 13 Warfarin exerts its anticoagulating effect by inhibiting the efficiency of VKORC1 at the level of producing reduced vitamin K from its epoxide form. Functional anomalies in VKORC1 are seen clinically as resistance to coumarin-type anticoagulants (warfarin resistance). 14 In addition, as a result of mutations at VKORC1, vitamin K fails to be hydroxylated and activated, so the coagulation is impeded. In our case, homozygous mutation in VKORC1 resulted in the inhibition of coagulation and hence the patient survived for 27 years without anticoagulation, having none of the thromboembolic complications.
In conclusion, the long-term survival without anticoagulation is good luck for the patient, and genetic analysis may explain the possible mechanism. Patients with metallic prosthetic heart valves have to use anticoagulations lifelong and this case report and brief review of the literature demonstrate the underlying mechanism of long-term survival without therapy as genetic mutations.
Footnotes
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) received no financial support for the research, authorship, and/or publication of this article.