
Abstract
Thrombate III is a human plasma-derived antithrombin III (AT-III) often utilized in patients on extracorporeal membrane oxygenation (ECMO) with suspected AT-III-mediated heparin resistance. It is supplied as 500-U and 1000-U vials, costing US$4.66 per unit. Literature is limited in describing the clinical value of AT-III in relation to its high cost. The primary objective was to determine conditions of use and associated cost of potentially unnecessary utilization of AT-III at The Johns Hopkins Hospital. Secondary objectives included evaluating the effect of AT-III on anticoagulation parameters and the overall cost utilized and wasted on AT-III. A retrospective cohort study was performed. The primary end point was the total cost associated with potentially unnecessary utilization of AT-III. There were 326 doses of AT-III administered to 65 patients in 2014. There were 177 (54%) potentially unnecessary doses associated with a cost of US$541 634. Antithrombin III repletion significantly increased median AT-III levels in non-ECMO and ECMO patients compared to baseline (non-ECMO: 62% vs 81%, P < .01; ECMO: 63% vs 81%, P < .01); however, 37.3% of ECMO and 49% of non-ECMO patients had therapeutic anticoagulation monitoring parameters prior to administration. A total cost of US$688 478 was spent on administered AT-III and US$417 194 (38%) was wasted. Utilizing restriction criteria and a new dosing strategy potentially results in estimated annual savings of US$556 000. Utilizing restriction criteria and alternative dosing strategies to mitigate waste and unnecessary use has the potential to result in significant cost savings.
Introduction
The coagulation cascade consists of clotting factors and natural anticoagulants that regulate the balance between clotting and bleeding. 1 Antithrombin III (AT-III) is a protease inhibitor that plays a central role in the body’s natural anticoagulation system. It primarily inhibits thrombin (factor IIa) and factor Xa and, to a lesser extent, factors IXa, XIa, XIIa, tissue plasminogen activator, plasmin, and kallikrein. The normal AT-III activity in adult plasma ranges from 80% to 120%, with a value of 100% correlating with 1 U of AT-III in 1 mL of plasma. There are a variety of factors that may affect the AT-III level including sex, use of medications, specifically heparin, and clinical status of the patient. In addition, neonates and pediatric patients congenitally have lower levels of AT-III, and adult levels are not reached until approximately 6 months to 1 year of age.
In its natural form, AT-III has a low level of anticoagulant activity; when bound to heparin, the anticoagulant effect is enhanced 1000-fold. 2 In a state of AT-III deficiency, heparin’s efficacy is diminished due to dependence on AT-III in order to exert its anticoagulant effect, which may be reflected as an inability to achieve therapeutic activated partial thromboplastin time (aPTT) and anti-Xa levels. 2,3 Acquired AT-III deficiency may occur in patients on extracorporeal membrane oxygenation (ECMO) or cardiopulmonary bypass (CPB) due to hemodilution, consumption of AT-III by the ECMO or CPB circuit, and utilization of large doses of heparin. 1,3 In these situations, repletion of AT-III may be warranted. 4
Thrombate III is a human plasma-derived AT-III product. It is supplied as 500-U and 1000-U vials, with an approximate cost of US$2330 and US$4660 per vial, respectively. The current practice for repletion of AT-III at The Johns Hopkins Hospital (JHH) for most patients (excluding adult cardiac surgery) is to use a calculation-based dosing strategy, which is the Food and Drug Administration (FDA)–approved calculation to use in patients with inherited AT-III deficiency. 5,6 Dose rounding to the nearest vial size is often not performed, which often leads to the use of partial vials. Other dosing strategies for AT-III repletion in pediatric patients with acquired AT-III deficiency have been reported anecdotally from various institutions, including a weight-based dose of 50 U/kg and rounding to the nearest vial size when possible. Alternatively, in adult cardiac surgery, a single 500- or 1000-U vial is most often administered. 7
This study first aimed to describe the current AT-III utilization strategies implemented across various populations at our institution because AT-III use has not been previously described at JHH and its use is unrestricted. In addition, because AT-III has a limited number of known indications and carries a high price, this study intended to determine the clinical conditions of use of AT-III in adult and pediatric patients and the potential cost associated with unnecessary utilization. We also sought to describe dosing strategies and their effects on AT-III levels and anticoagulation parameters in order to further elucidate AT-III’s clinical utility in relation to cost. Finally, this study aimed to evaluate the overall cost utilized and wasted on AT-III and to identify potential opportunities for cost savings.
Methods
This retrospective cohort study included patients identified through a transfusion medicine dispensing report. Adult and pediatric patients were included in the study if they were admitted to JHH, a 1051-bed academic medical center, and received AT-III therapy from January 2014 to December 2014. Adult patients were defined as patients at least 18 years of age. No patients were excluded from the analysis.
All data were collected through chart review. Data were collected for each dose of AT-III given per patient. Pre- and postrepletion levels of AT-III, anti-Xa, aPTT, activated clotting time (ACT), fibrinogen, and heparin infusion rates were collected. Values recorded within 24 hours prior to AT-III administration were considered prerepletion values, and values recorded within 24 hours postadministration of AT-III were considered postrepletion values. All adult cardiac surgery patients received AT-III in the operating room (OR), and data were collected from perfusionist and anesthesiologist records during the time of the procedure. Table 1 displays therapeutic ranges for the anticoagulation monitoring parameters utilized for analysis.
Therapeutic Ranges for Anticoagulation Parameters.
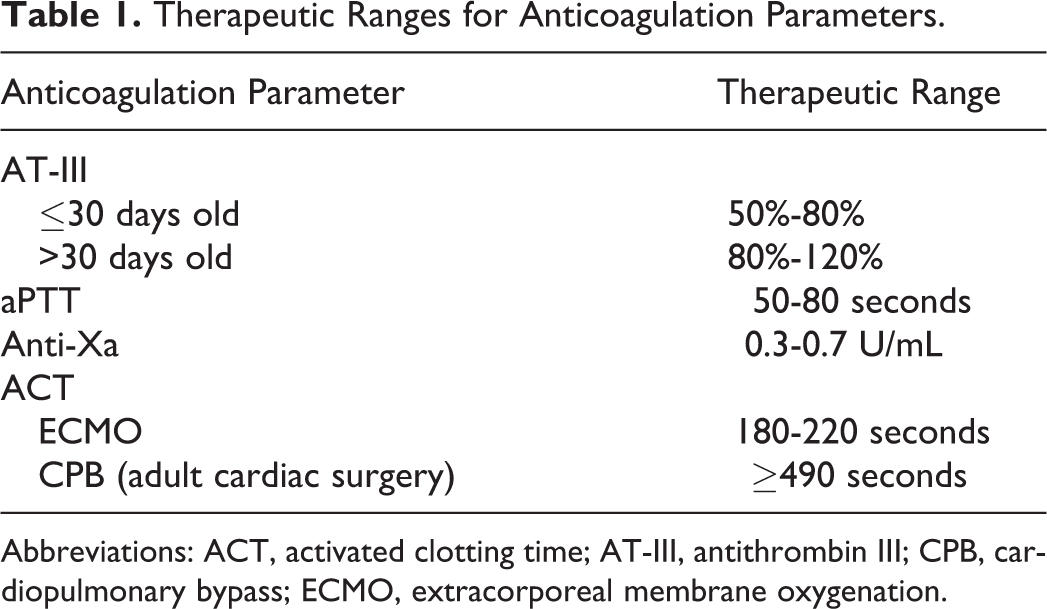
Abbreviations: ACT, activated clotting time; AT-III, antithrombin III; CPB, cardiopulmonary bypass; ECMO, extracorporeal membrane oxygenation.
The primary end point was the total cost associated with unnecessary utilization of AT-III. In order to determine what doses of AT-III were given for unnecessary indications, a set of criteria were formulated for ECMO and non-ECMO patients (Table 2) and adult cardiac surgery patients (Table 2) based on standard practice, anticoagulation monitoring parameters, and current guidelines for repletion in the institutional ECMO protocol. In order for a dose to be considered “appropriate,” all non-ECMO patients had to meet criteria 1 to 4 in Table 2, ECMO and non-ECMO. Pediatric patients undergoing ECMO had to meet all criteria in Table 2, ECMO and non-ECMO. For adult cardiac surgery patients, all criteria in Table 2, Adult Cardiac Surgery Patients, had to be met. 8 –10
Study Criteria for Determination of Appropriate Indications for AT-III Repletion.
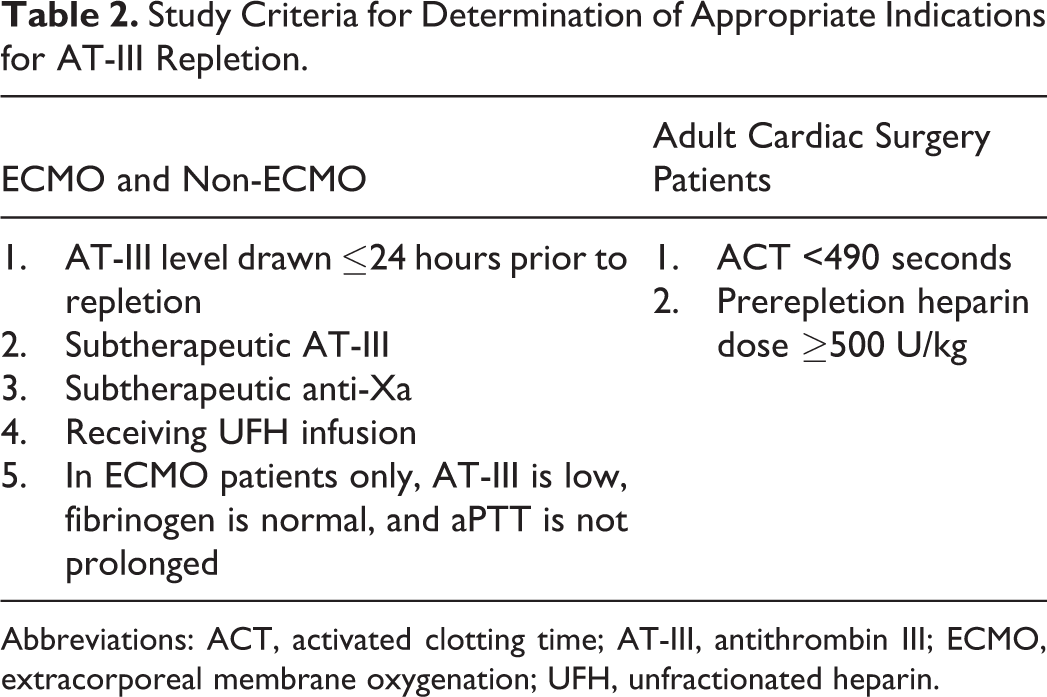
Abbreviations: ACT, activated clotting time; AT-III, antithrombin III; ECMO, extracorporeal membrane oxygenation; UFH, unfractionated heparin.
Overall, AT-III utilization practices and the effect of AT-III repletion on AT-III levels and anticoagulation parameters were evaluated as secondary end points. Various data were evaluated, including the percentage change in AT-III level from prerepletion to postrepletion, the median dose (U/kg) of AT-III given, and the median heparin infusion rate pre-AT-III and post-AT-III repletion. For adult cardiac surgery patients, data collection included the cumulative heparin dose prerepletion, time from first heparin dose to AT-III dose, and the percentage of subtherapeutic ACTs pre- and postrepletion.
Other secondary end points included the cost of administered and wasted AT-III as well as potential cost savings associated with alternative dosing strategies and implementation of proposed restriction criteria. An acquisition cost of US$4.66 per unit of AT-III was utilized for the analysis. The cost administered was defined as the cost associated with the total number of units the patient received, and the cost wasted was defined as the cost associated with the total number of units remaining in the vial that was not used.
Statistical Analysis
Descriptive statistics were performed for demographic data as well as characterizing AT-III repletion and associated anticoagulation monitoring parameters. Categorical data were reported as counts and percentages. Statistical analysis for dependent categorical variables was performed using the McNemar test. Nonparametric continuous data were reported as medians and ranges. Statistical analysis for dependent continuous variables was performed using the Wilcoxon signed rank test. All analyses were performed using STATA Statistical Software, version 13 (Stata Corp LP, College Station, Texas).
Results
Patient Population
A total of 65 patients (15 ECMO, 34 non-ECMO, and 19 adult cardiac surgery) received 326 doses of AT-III during the study period. The majority (65%) of patients were pediatric patients in the pediatric intensive care unit. Table 3 displays the demographic characteristics of all patients. Three patients received AT-III while both on and off ECMO, and these patients were included in both groups for baseline demographics. Overall, patients on ECMO were younger than those not on ECMO, and non-ECMO patients were more likely to be post-CPB. There were 19 adult cardiac patients who received 20 AT-III doses. Adult cardiac surgery patients were a median of 62 years old, and the majority were male.
Patient Demographics.a,b
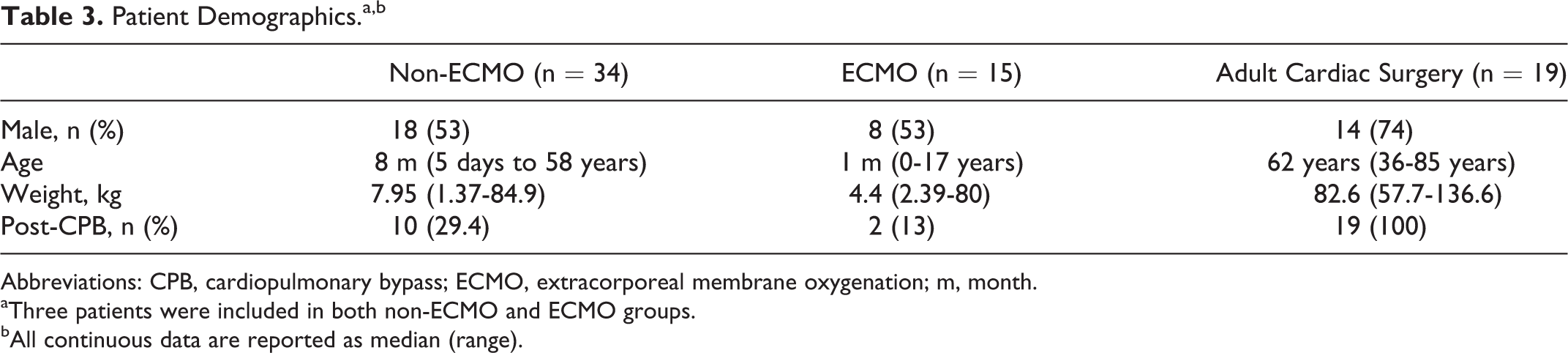
Abbreviations: CPB, cardiopulmonary bypass; ECMO, extracorporeal membrane oxygenation; m, month.
aThree patients were included in both non-ECMO and ECMO groups.
bAll continuous data are reported as median (range).
Primary End Point
Overall, 177 (54%) of the total 326 doses of AT-III administered during the study period were determined to be potentially unnecessary based on the criteria in Table 2, which represented a cost of US$541 634. Administration of unnecessary doses, defined by failure to meet criteria as discussed above, included 171 ECMO and non-ECMO doses and 6 adult cardiac surgery doses. Table 4 displays the reasons and associated cost of unnecessary AT-III use. The primary reason for unnecessary use of AT-III was administration in patients with therapeutic anti-Xa levels. Antithrombin III was also administered to some non-ECMO and ECMO patients in light of normal AT-III levels. In addition, 12% of non-ECMO patients were not receiving unfractionated heparin (UFH) at the time of repletion (were receiving either low-molecular-weight heparin or bivalirudin). There was a total cost of US$527 468 spent on non-ECMO and ECMO AT-III doses deemed potentially unnecessary based on the criteria in Table 2. In adult cardiac surgery patients, 6 (30%) of the 20 doses administered to adult cardiac surgery patients were unnecessary, largely due to a therapeutic ACT prerepletion, and associated with a cost of US$14 166.
Unnecessary Use of AT-III.
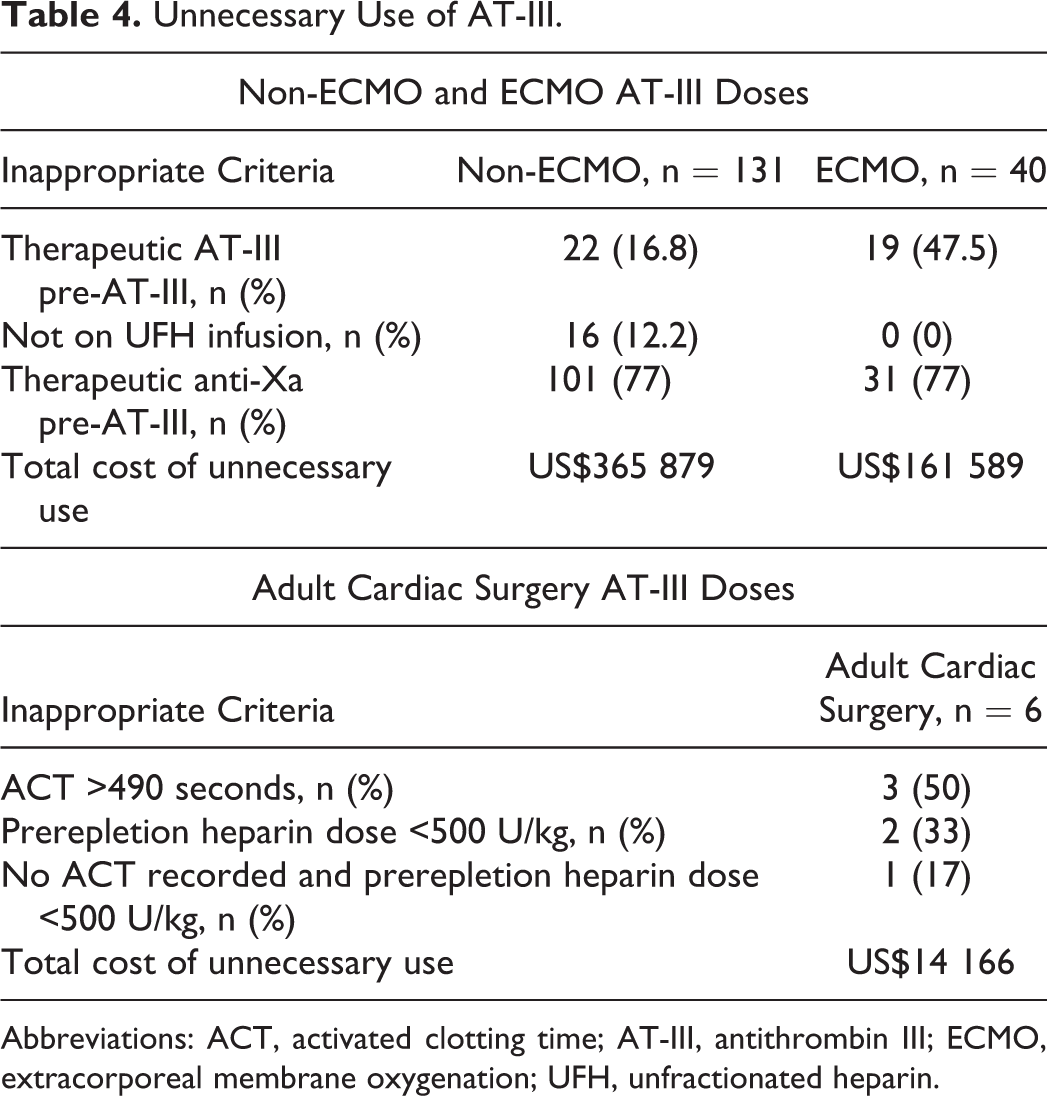
Abbreviations: ACT, activated clotting time; AT-III, antithrombin III; ECMO, extracorporeal membrane oxygenation; UFH, unfractionated heparin.
Secondary End Points
Non-ECMO patients received a higher median AT-III dose (38 vs 33.5 U/kg) and a higher median number of total doses per patient (16 vs 6) compared to ECMO patients. In general, adult cardiac surgery patients received 1 dose (equivalent to 1 vial, 500-550 U, 6.96 U/kg) of AT-III in the OR. More AT-III doses were preceded by fresh frozen plasma (FFP) administration in ECMO patients compared to non-ECMO patients (39 [47%] vs 23 [10.3%]), and 15% of adult cardiac surgery patients received FFP prior to AT-III repletion.
There were 223 doses of AT-III administered to 34 non-ECMO patients and 83 doses administered to 15 ECMO patients (see Supplemental Tables S1 and S2). Repletion of AT-III resulted in a significant increase in therapeutic AT-III levels in non-ECMO and ECMO patients (58.6% and 60.2%, respectively, P < .001 for both groups). Although a high percentage of patients had therapeutic anti-Xa levels prior to repletion, there was a significant increase in therapeutic anti-Xa levels from pre- to postrepletion in both non-ECMO and ECMO patients (non-ECMO: prerepletion 49% vs postrepletion 64.9%, P < .001; ECMO: prerepletion 37.3% vs postrepletion 60.2%, P < .001). There was a significant increase in the percentage of patients with a supratherapeutic aPTT in both groups postrepletion (non-ECMO: prerepletion 25.6% vs postrepletion 40.3%, P < .001; ECMO: prerepletion 22.9% vs postrepletion 31.3%, P = .03). Finally, in patients on and off ECMO, there was no change in the heparin infusion rate after AT-III administration.
Table 5 displays the effects of AT-III administration on various parameters in adult cardiac surgery patients. The median dose of heparin prior to AT-III repletion was 756 U/kg. Seventeen (85%) doses of AT-III were preceded by heparin doses of at least 500 U/kg. All patients had subtherapeutic ACT levels at the time of AT-III repletion. The percentage of patients with a subtherapeutic ACT level was significantly decreased after AT-III repletion (prerepletion 100% vs postrepletion 50%; P < .001).
AT-III in Adult Cardiac Surgery Patients.a,b
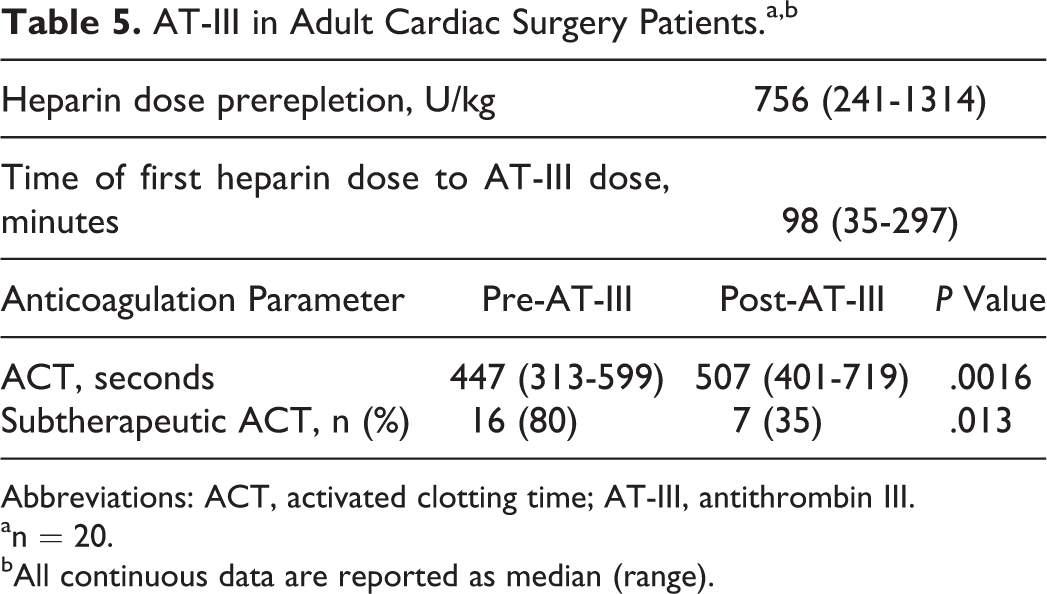
Abbreviations: ACT, activated clotting time; AT-III, antithrombin III.
an = 20.
bAll continuous data are reported as median (range).
A total of US$688 478 was spent on AT-III administration and US$417 194 was wasted due to unused medication from partial vials (Table 6). A median of 57% of the vial was wasted in non-ECMO and ECMO patients. When further analyzed, the waste was most apparent particularly in patients under 10 kg.
AT-III Cost Data.a,b
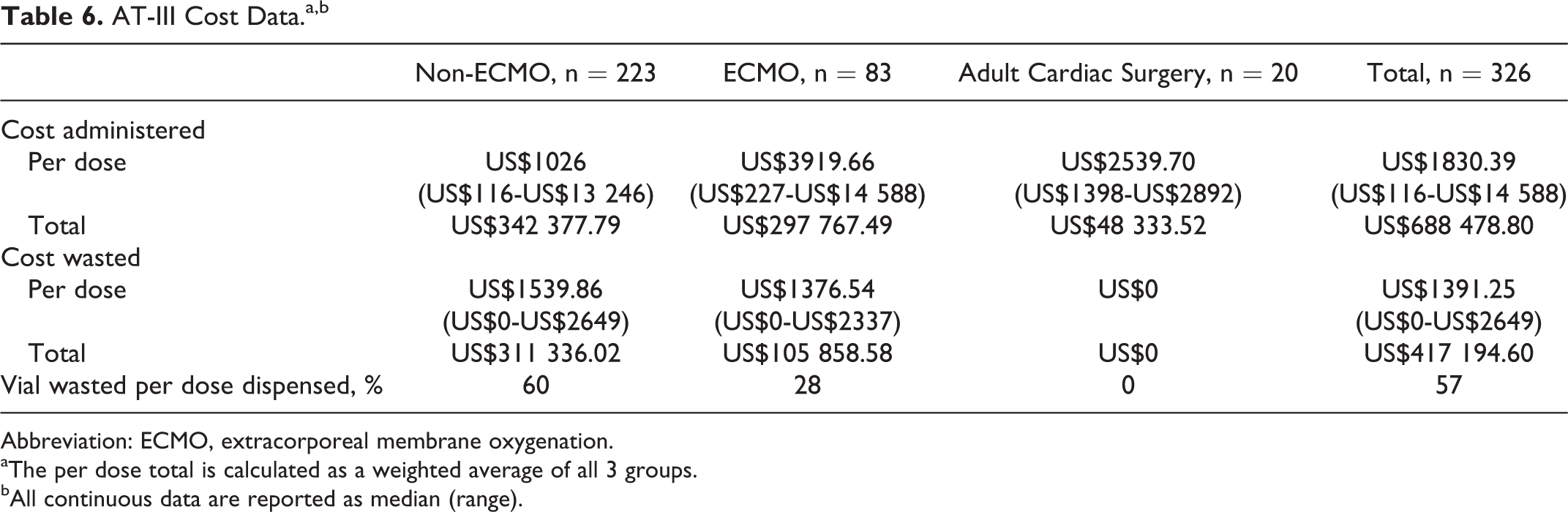
Abbreviation: ECMO, extracorporeal membrane oxygenation.
aThe per dose total is calculated as a weighted average of all 3 groups.
bAll continuous data are reported as median (range).
Figure 1 displays the cost and associated waste of the current, unrestricted practices and dosing strategy. It also shows the estimated cost per year if restrictions were implemented to avoid unnecessary use (refer to Table 2) in addition to utilizing a weight-based dosing range strategy of 30 to 50 U/kg in order to mitigate waste. If both strategies are implemented, there could be an estimated cost savings of US$556 000 per year (based on 2014 data).
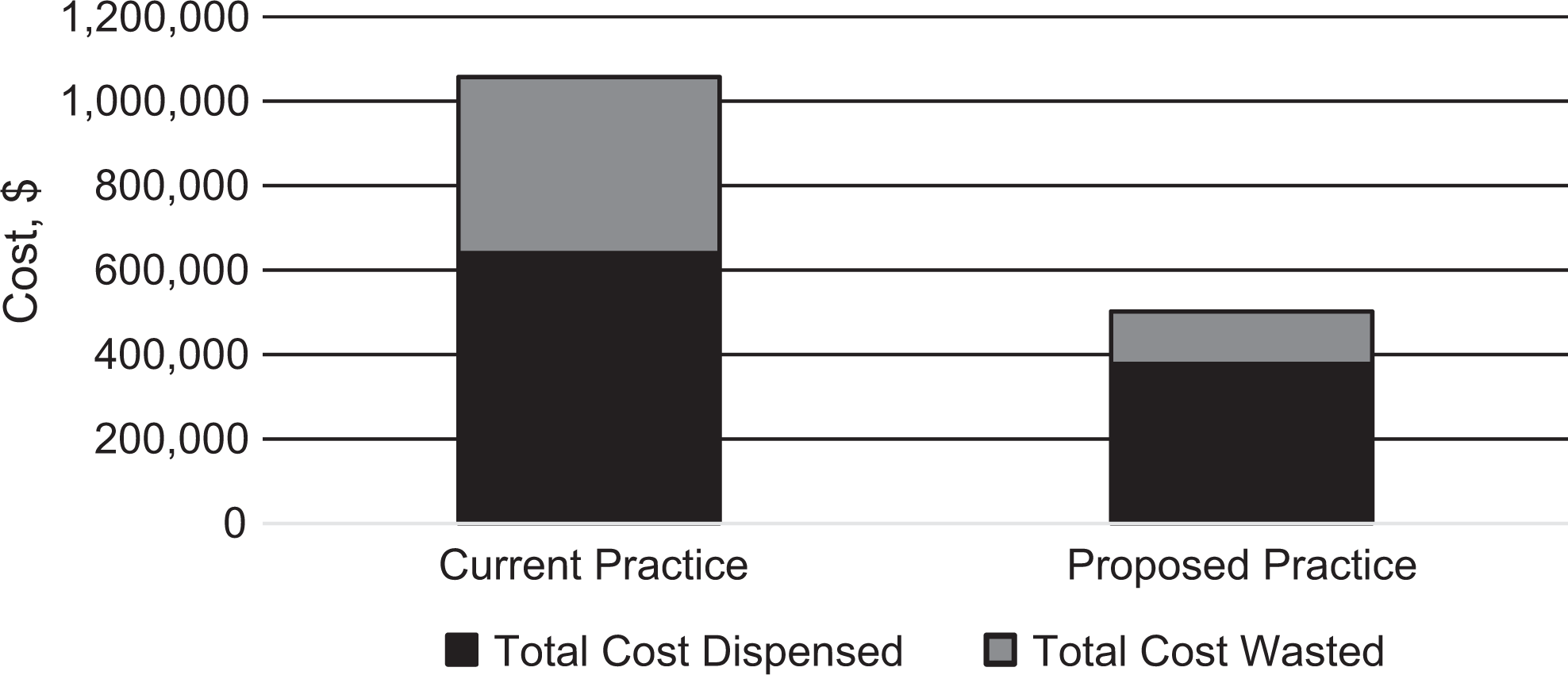
Costs dispensed and wasted associated with current versus proposed strategy.
Discussion
It is estimated that approximately 20% of patients undergoing CPB 11 and an unknown (although likely higher) percentage of ECMO patients are heparin resistant due to acquired AT-III deficiency. 12 The ultimate goal of AT-III repletion is to enhance the effect of UFH. Failure to correct heparin resistance due to AT-III deficiency is associated with an increased risk of thromboembolic events, prolonged intensive care unit stay, and surgical reexploration. 13 Administration of AT-III to correct heparin resistance does not come without risks. Antithrombin III is made from human blood, so there is a risk of transmitting infectious diseases, specifically the Creutzfeldt-Jakob disease agent. The risk of bleeding associated with AT-III administration is controversial. In a study conducted by Niebler et al, 14 the authors concluded that there was no increased frequency of bleeding when administering AT-III to pediatric patients on ECMO. In patients with hereditary antithrombin deficiency, however, there is a reported 5% incidence of hematomas. 5,6 Intra-abdominal hemorrhage and hemarthrosis have also been reported. 5,6 In this study, repleting AT-III was not indicated in the majority of cases and was associated with high cost, increase in supratherapeutic aPTT levels, and no significant change in the heparin infusion rate. In light of a therapeutic anti-Xa or ACT, despite a low AT-III level, such as was seen in this study, the benefit of AT-III supplementation remains undetermined. It is therefore important to consider the risks and benefits when giving AT-III and that, perhaps, if anti-Xa or ACT levels are therapeutic, low AT-III levels do not necessarily need to be treated.
Not only was there a high cost associated with unnecessary use of AT-III but also there was a high cost associated with wasted AT-III. The current practice at JHH in all patients except adult cardiac surgery is to use a calculation-based dosing strategy, which is the FDA-approved calculation to use in patients with inherited AT-III deficiency. Other dosing strategies have been anecdotally reported, including a weight-based dose of 50 U/kg. The average dose of AT-III in this study was 35 U/kg. In addition, the doses are not rounded to the nearest vial size when applicable. Targeting a higher weight-based dose and rounding to the nearest vial size, if possible within this dosing range, can help to mitigate waste. If restriction criteria were implemented to reduce unnecessary use of AT-III in addition to a weight-based dosing strategy as described above, it could save an estimated US$556 000 per year (based on 2014 data). While using a higher weight-based dose might decrease the amount of drug wasted, it is not known how this would affect AT-III level, anticoagulation parameters, potential bleeding risk, and need for subsequent doses of AT-III.
The Extracorporeal Life Support Organization recommends to maintain AT-III levels within the normal range in patients on ECMO by repleting with either FFP or AT-III concentrate. 4 In our study, approximately half of patients received FFP prior to AT-III. In non-ECMO patients, the use of FFP prior to AT-III was much lower. This is to be expected, because FFP is administered in a significant amount of volume that may not be tolerated by fluid-overloaded or fluid-sensitive patients, such as those with cardiac disease. In patients on ECMO, however, administration of volume may not be as great a concern because the volume can be removed from the circuit via ultrafiltration. FFP costs approximately US$43 per unit (1 U = 250 mL), which is significantly less money than AT-III (US$4.66 per unit). In a 25-kg patient, for example, the dose of FFP would be 1 U (10 mL/kg), costing $43. The dose of AT-III would be 1250 U (50 U/kg), costing US$5825. From a cost savings perspective, it may be reasonable to require the use of FFP prior to AT-III repletion in patients who can tolerate the volume, particularly in ECMO patients.
This study had several limitations. The retrospective nature does not allow for the determination of other factors that may have affected anti-Xa, aPTT, and other anticoagulation parameters. The accuracy of coagulation laboratory values in critically ill patients should be taken into account, such as presence of coagulopathy, liver and/or kidney dysfunction, and inflammation, as these conditions may impact the results of such testing. Due to the unrestricted use of AT-III, AT-III repletion practices were left up to the discretion of the provider, such that we do not know the actual reasons for repletion. Finally, for those with anticoagulation values available, the time to collect pre- and postrepletion anticoagulation parameters varied for each patient (up to a 24-hour window), and so some of the postrepletion levels may be more or less reflective of the effects of AT-III repletion depending on how quickly AT-III was being consumed in relation to when it was repleted and when the levels were drawn.
Conclusion
In conclusion, AT-III repletion was associated with high cost, significant increases in anticoagulation parameters, and no significant change in the heparin infusion rate. Unnecessary or ineffective utilization of AT-III was primarily due to doses being given to patients with therapeutic anticoagulation parameters at baseline. In addition, there was a high amount of waste with each dose based on the current dosing strategy. Through the development of uniformly accepted criteria for AT-III administration and utilization of a revised dosing strategy, unnecessary doses and waste could be mitigated, resulting in significant cost savings. Future research involving the use of AT-III in critically ill patients is warranted, as there is a significant amount of administration, yet both use and effectiveness of administration remain highly variable both within and across institutions.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.