
Abstract
Portal vein thrombosis (PVT) is a common complication in cirrhosis. The aim of this study was to determine risk factors for PVT, assess the efficacy of anticoagulant therapy, and evaluate the effects of PVT on patients with cirrhosis undergoing elective transjugular intrahepatic portosystemic shunt (TIPSS). A total of 101 patients with cirrhosis undergoing elective TIPSS were prospectively studied. After TIPSS, all patients received preventive therapy for PVT and were followed up at 3, 6, 12, and 24 months. Clinical outcomes were compared between patients who developed PVT after TIPSS and those who did not. Multivariate analysis showed that white blood cell count (relative risk [RR]: 0.377; 95% confidence interval [CI]: 0.132-0.579; P = .001), Child-Turcotte-Pugh score (RR: 1.547; 95% CI: 1.029-2.365; P = .032), and ascites (RR: 1.264; 95% CI: 1.019-1.742; P = .040) were independent predictors for PVT. Warfarin treatment within 12 months achieved significantly higher rates of complete recanalization than aspirin or clopidogrel in patients with PVT (54.5% vs 31.3%; P = .013), although adverse events were similar between the 2 groups (P > .05). Patients without PVT had significantly lower 2-year cumulative rates of variceal rebleeding (15.9% vs 36.6%; P = .023), shunt dysfunction (27.0% vs 46.8%; P = .039), hepatic encephalopathy (24.1% vs 42.6%; P = .045), and hepatocellular carcinoma (11.4% vs 31.2%; P = .024) and markedly higher 2-year cumulative survival rates (89.8% vs 72.9%; P = .041) than those with PVT. The PVT is associated with poorer clinical outcomes in TIPSS-treated patients, and warfarin is both safe and more effective in recanalizing PVT than aspirin or clopidogrel.
Keywords
Introduction
Portal vein thrombosis (PVT) is defined as thrombosis within the trunk of portal vein, which may extend to intrahepatic portal branches, the splenic or mesenteric veins. 1 It is very common in patients with cirrhosis, with a prevalence varying from 16% to 26%. 2,3 It is frequent in decompensated cirrhosis, often associated with hepatocellular carcinoma, is less frequent in compensated cirrhosis, and is relatively rare in patients with a previously healthy liver, at least in developed countries. 1 Clinical features of PVT are heterogeneous, associated with the site and extension of its obstruction in the portal venous system. The PVT, in decompensated cirrhosis, was more frequently detected at the chronic stage because of complications of portal hypertension, such as variceal bleeding, thrombocytopenia, or symptomatic splenomegaly. 1
Optimal management of PVT in cirrhosis is currently not established in any consensus practice guideline. Treatment strategies mostly involve the use of anticoagulation, whereas thrombectomy and transjugular intrahepatic portosystemic shunts (TIPSS) are often considered second-line options. 3 The TIPSS was first attempted to treat 7 patients with noncavernomatous PVT and recurrent variceal bleeding, and recanalization of portal vein trunk was successful in all patients. 4 Since then, its efficacy in recanalizing PVT has been confirmed by many studies. 5 –7 However, the course and effects of PVT on clinical outcomes in patients with cirrhosis undergoing elective TIPSS have seldom been documented. Han et al 6 reported that occlusion of main portal vein by thrombosis was closely related to technical success and survival in patients undergoing TIPSS. Owing to technical difficulty and high cost, TIPSS has been severely restricted in its application. Therefore, optimal management of PVT in patients undergoing TIPSS has not been addressed in consensus clinical guidelines, either. Despite Han et al 6 reporting the use of warfarin for 6 months to 1 year and lifelong aspirin for preventing PVT recurrence and maintaining functional TIPSS stent, they didn’t further report the efficacy of this strategy in detail.
Therefore, we conducted the present study to determine the risk factors for PVT, compare the efficacy of anticoagulant therapy with antiplatelet therapy, and evaluate the effects of PVT on patients with cirrhosis undergoing elective TIPSS.
Patients and Methods
Patients
Between June 2012 and February 2016, 131 consecutive TIPSS-treated patients were identified and prospectively studied in our institution. Twenty-five patients were with PVT before TIPSS and were excluded from analysis in this study. Another 5 patients failed to come for follow-up visits after TIPSS and were thus not analyzed (Figure 1). All patients provided informed consent before participating in this study. The study protocol was approved by the institutional ethics committee.
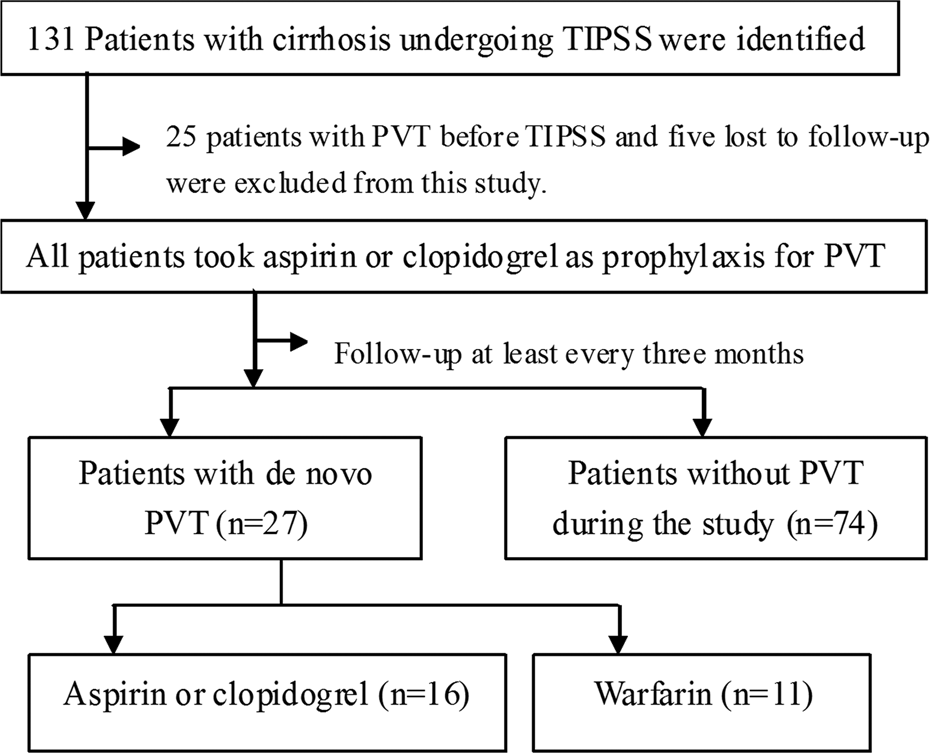
Disposition of the study population. PVT indicates portal vein thrombosis; TIPSS, transjugular intrahepatic portosystemic shunt.
Transjugular Intrahepatic Portosystemic Shunt Procedure
Before TIPSS, all candidates underwent Doppler ultrasonography and computed tomography (CT) portal venography to detect PVT, 8,9 with focus on patency of the portal trunk and its branches. For patients with hepatocellular carcinoma, malignant PVT was diagnosed by arterial phase enhancement of the thrombus on CT contrast-enhanced portal venography 10 or an arterial-like flow on Doppler ultrasonography. 11 Patients with malignant PVT were not considered for TIPSS placement.
The TIPSS was performed by 2 highly experienced interventional radiologists in our institution. RUPS 100 puncture kit (Cook Inc. Bloomington, Indiana) and expanded polytetrafluoroethylene (ePTFE)-covered and bare stents (Fluency stent graft, 8 mm × 60 mm, Angiomed GmbH Co. subsidiary of C.R. Bard, Inc., New Jersey, USA) were used in this study. A bare stent was added to an ePTFE-covered stent if required, depending on patients’ anatomical conditions. Stents were placed between the hepatic vein and portal vein. Dilated collaterals including short gastric vein and gastric coronary vein were embolized with spring coils of varying diameters (35-8/5 mm, 35-10/5 mm, 35-6/3 mm, 35-5/3 mm, 35-4/3 mm Cook Inc.) in the procedure.
Treatment and Follow-Up Protocols
After TIPSS procedure, our treatment protocol was that patients were initially given low-molecular-weight Ca heparin (4100 IU Qd or Q12 h subcutaneously) for 1 week; subsequently, patients were advised to take aspirin (100 mg/d) or clopidogrel (75 mg/d) if their platelets were above 50 × 109/L for preventing formation of PVT. All patients were followed up by caring physicians at 3, 6, 12, and 24 months in our institution. Then annual or additional visits were instituted if necessary. The follow-up study included clinical assessment, biochemical tests, CT contrast-enhanced portal venography, and Doppler ultrasonography. Data were documented in the computerized medical record system and were retrievable upon analysis.
During the follow-up, oral warfarin (1.5-3.0 mg/d) was administered to patients who developed PVT after written informed consent was obtained since the efficacy of warfarin in this scenario was not clear and with potential risks. Doses of warfarin were adjusted to achieve an international normalized ratio (INR) of 2.0 to 3.0, which was determined weekly for dose adjustments until it was stable. Then, INR was monitored at least every 3 months.
End Points
The primary end point was clinical outcomes, including variceal rebleeding, shunt dysfunction, hepatic encephalopathy, hepatocellular carcinoma, and survival, which were compared between patients who developed PVT after TIPSS and those who did not. Secondary end points include complete recanalization rates of PVT and associated side effects after antiplatelet and anticoagulation therapy.
Statistical Analysis
Statistical analysis was performed using the software SPSS version 17.0 for windows. Normal distribution was tested by the Kolmogorov-Smirnov test. Data were expressed as mean ± standard deviation, median (range), or proportions. The χ2 test, Student t test, or Mann-Whitney test were adopted to identify significant baseline factors for PVT after TIPSS in univariate analysis. In multivariate analysis for independent baseline predictors of TVT after TIPSS, a backward (Wald test) Cox proportional hazards regression analysis was executed. Survival analysis was performed by the Kaplan-Meier method and compared by log-rank test. All statistical tests were 2-sided, and a P value below .05 was accepted as statistically significant.
Results
Patient Characteristics
The baseline characteristics of the study population are shown in Table 1. In our study, TIPSS indications were variceal hemorrhage or refractory ascites. No TIPSS-treated patients had particular issues such as serum bilirubin above 100 µmol/L, a history of hepatic encephalopathy, tumoral or other lesions on the puncture tract, and occlusive PVT in the trunk of portal vein (including cavernoma). There were 66 (65.3%) males and 35 (34.7%) females. Mean age was 52 (11.0) years (range 29-80). Etiology of cirrhosis was as follows: hepatitis B virus in 51 (50.5%) patients, hepatitis C virus in 18 (17.8%), alcohol abuse in 7 (6.9%), primary biliary cirrhosis in 8 (7.9%), and cirrhosis of unknown origin in 17 (16.8%). Concomitant diseases include primary hypertension in 15 (14.9%) patients, diabetes in 3 (3.0%), and hepatocellular carcinoma in 6 (5.9%), though no TIPSS-treated patients had malignant PVT. For TIPSS procedure, 1 ePTFE-covered stent was placed in 88 (87.1%) patients and 1 ePTFE-covered plus 1 bared stent in 13 (12.9%) patients. The mean values of Child-Turcotte-Pugh (CTP) score and Model for End-Stage Liver Disease score were 9.8 and 11.3, respectively.
Baseline Characteristics of the Study Population.
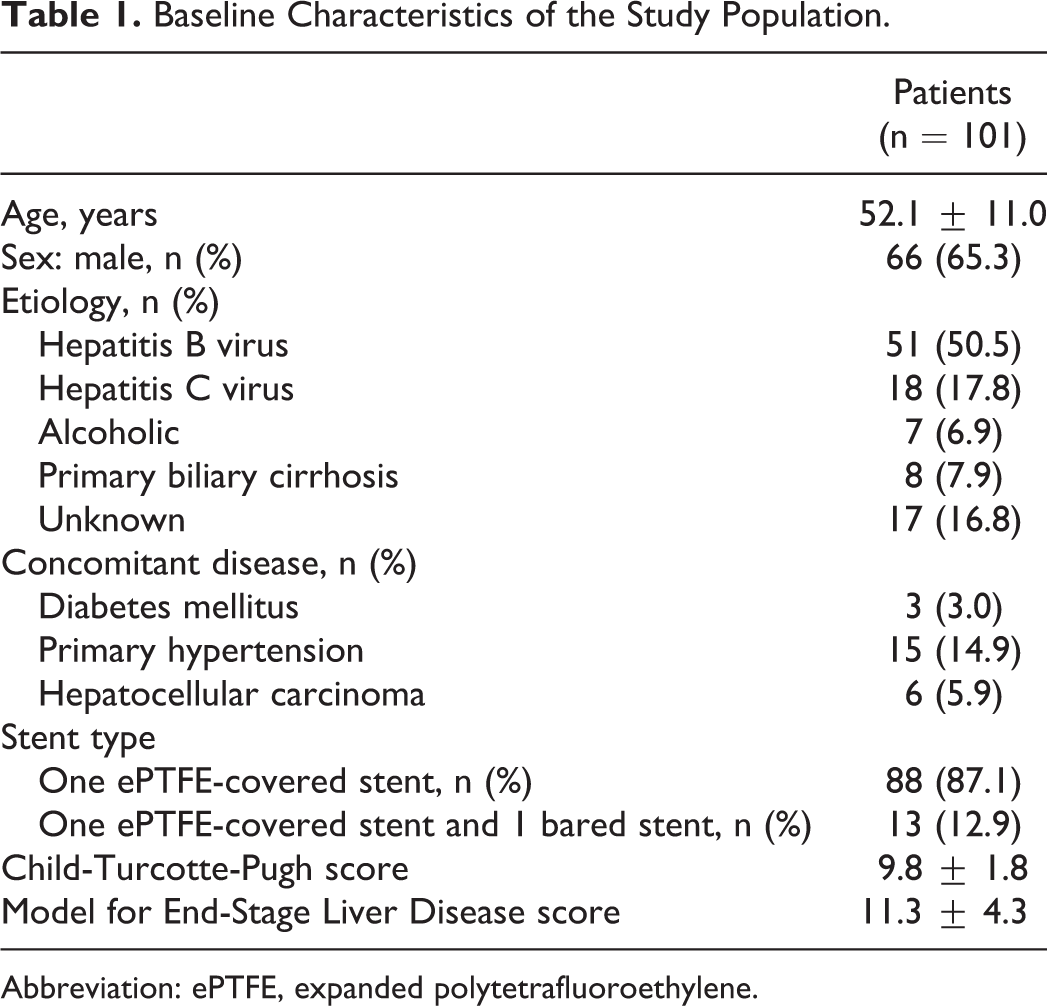
Abbreviation: ePTFE, expanded polytetrafluoroethylene.
Portal Vein Thrombosis Post-TIPSS
Twenty-seven (26.7%) patients developed PVT after a median of 6.0 (range 1-23) months after TIPSS. Eighteen of these 27 patients had PVT involving both the portal trunk and other branches: the left or right portal branch in 11, the superior mesenteric vein in 4, and the splenic vein in 3. Eight patients developed PVT involving only the portal trunk. All these PVT were partially occlusive. The 1 remaining patient developed occlusive PVT within the TIPSS stent. Overall, 74 (73.3%) patients did not develop PVT during the follow-up period.
Risk Factors for PVT Development Post-TIPSS
In univariate analysis (Table 2), compared to those without PVT, patients who had PVT after TIPSS demonstrated significantly lower white blood cell (WBC; 2.30 ± 0.61 vs 3.62 ± 1.91; P = .000) and platelet (58.5 ± 16.1 vs 70.4 ± 36.0; P = .025) but markedly higher prothrombin time (21.7 ± 3.2 vs 19.9 ± 3.8; P = .017) and INR (1.81 ± 0.31 vs 1.66 ± 0.33; P = .039). Interestingly, antiviral therapy choice was significantly different between the 2 groups (entecavir: 88.2% vs 50%; P = .025). Multivariate analysis by Cox proportional hazard model showed that WBC count (relative risk [RR]: 0.377; 95% confidence interval [CI]: 0.132-0.579; P = .001), CTP score (RR: 1.547; 95% CI: 1.029-2.365; P = .032), and ascites (RR: 1.264; 95% CI: 1.019-1.742; P = .040) were independent baseline predictors for PVT (Table 3).
Risk Factors for Portal Vein Thrombosis Post-TIPSS by Univariate Analysis.
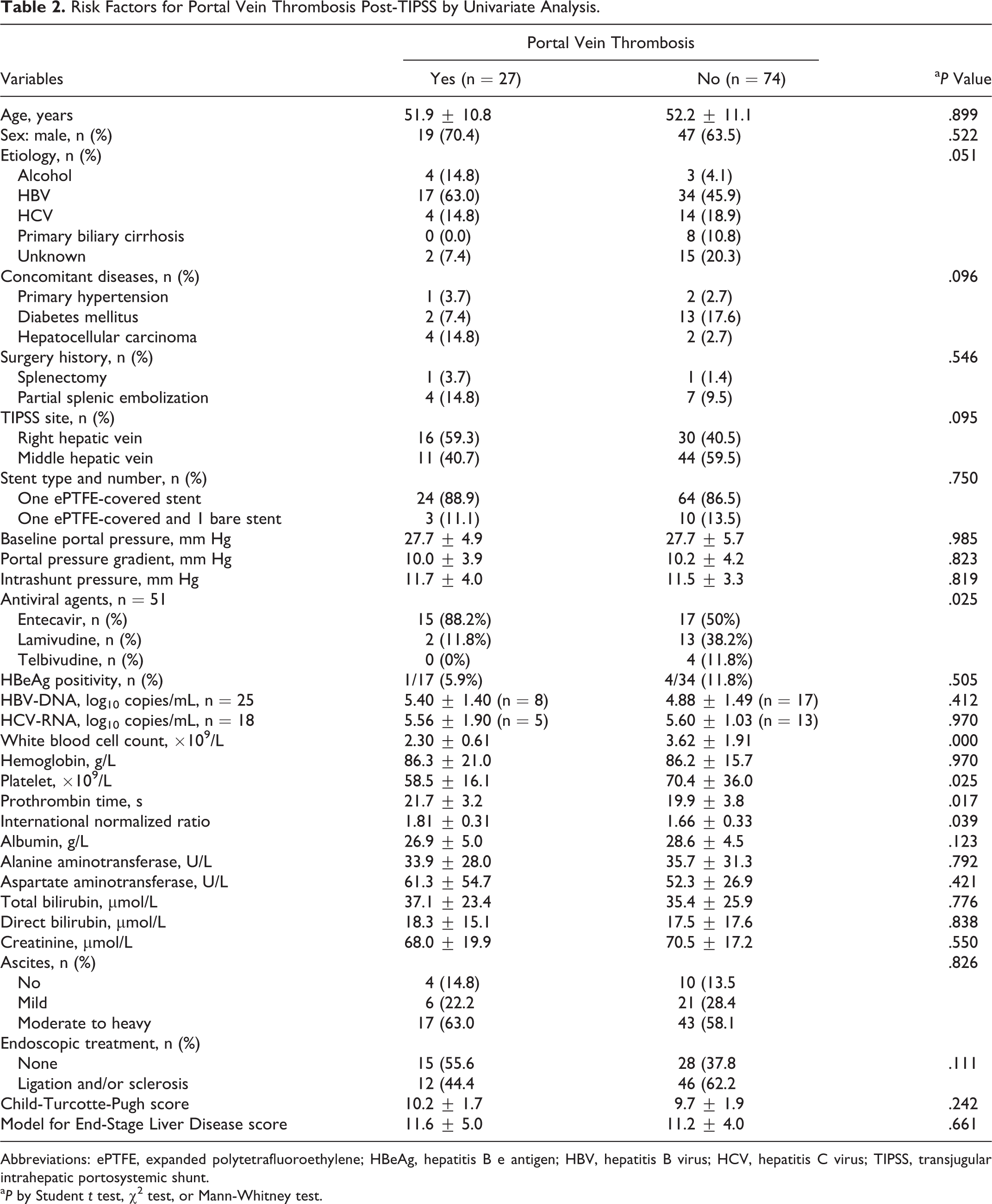
Abbreviations: ePTFE, expanded polytetrafluoroethylene; HBeAg, hepatitis B e antigen; HBV, hepatitis B virus; HCV, hepatitis C virus; TIPSS, transjugular intrahepatic portosystemic shunt.
a P by Student t test, χ2 test, or Mann-Whitney test.
Significant Risk Factors for Portal Vein Thrombosis Post-TIPSS by Multivariate Analysis.
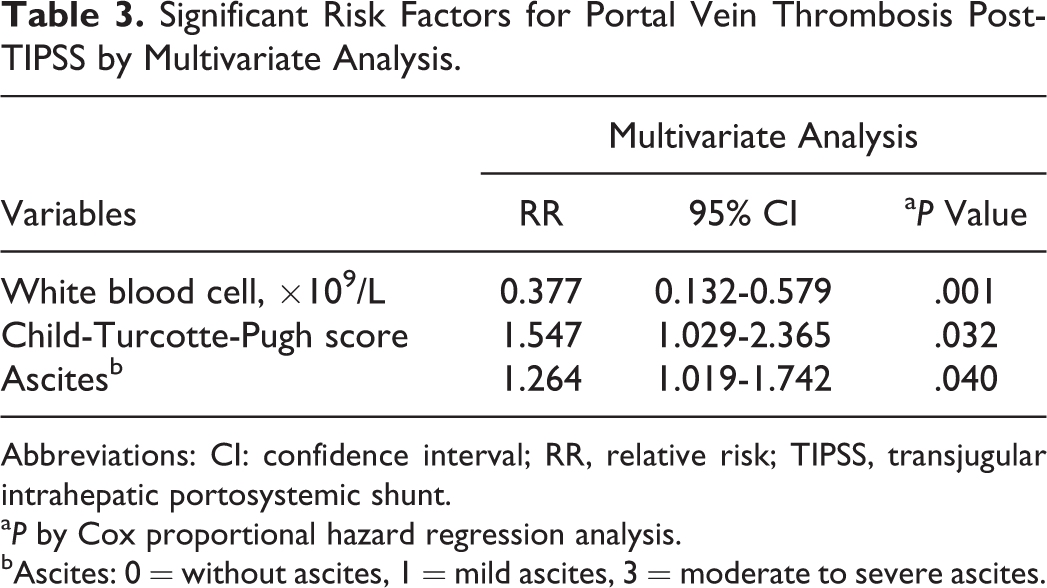
Abbreviations: CI: confidence interval; RR, relative risk; TIPSS, transjugular intrahepatic portosystemic shunt.
a P by Cox proportional hazard regression analysis.
bAscites: 0 = without ascites, 1 = mild ascites, 3 = moderate to severe ascites.
Efficacy and Side Effects of Anticoagulant and Antiplatelet Therapy
Among the 27 patients who developed PVT after a median of 6 (range: 1-23) months, 11 (40.7%) patients switched to warfarin, and the remaining 16 (59.3%) patients continued their previous therapy. Baseline features were comparable between these 2 groups except for total and direct bilirubin (Supplementary Table 1). Of the 11 patients switching to warfarin for a median of 10 (range: 1-12) months, complete recanalization was detected in 6 (partial recanalization in 3 and no change in 2) patients, as compared to complete recanalization in 5 (partial recanalization in 0 and no change in 11) of the 16 patients who continued aspirin or clopidogrel therapy for a median of 7.5 (range: 5-10) months (54.5% vs 31.3%; P = .013). Figure 2A and B illustrates sequential CT contrast-enhanced portal venography in a patient who had a partially occlusive PVT at the portal vein trunk, which was recanalized after 1 month of warfarin (1.5 mg/d) treatment.
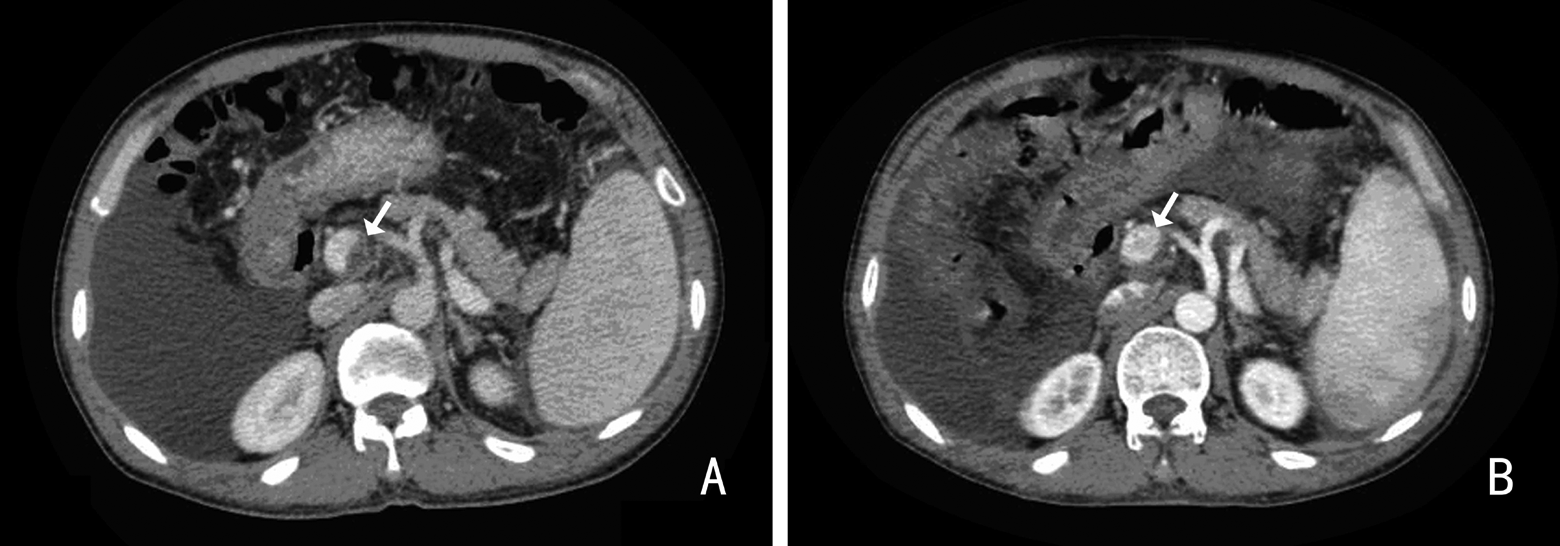
CT contrast-enhanced portal venography showing a partially occlusive thrombus at the trunk of portal vein (A, white arrow) and complete recanalization of the thrombus 1 month following warfarin treatment (B, white arrow) in a patient with hepatitis B virus–related cirrhosis. CT indicates computed tomography.
Of the 11 patients who received warfarin, 4 had epigastric discomfort, as compared to 42 of the 90 patients who received aspirin or clopidogrel (36.4% vs 46.7%; P = .517), which was relieved by pantoprazole. Two of the 11 patients receiving warfarin and 21 of 90 patients receiving aspirin or clopidogrel reported nasal or gingival hemorrhage (18.2% vs 23.3%; P = .701), which resolved after temporary discontinuation of treatment. Peptic ulcer disease or hemorrhagic gastritis was found in 0 of 11 patients treated by warfarin, as compared to 5 of 90 patients treated by aspirin or clopidogrel (0% vs 5.6%; P = .423). Other severe adverse events were not recorded.
Clinical Outcomes Post-TIPSS
Variceal rebleeding
Overall, 15 patients had at least 1 episode of variceal rebleeding proved by gastroscopy after TIPSS, of whom 12 were due to shunt dysfunction (stenosis in 11 and occlusion in 1). The 1-year and 2-year cumulative variceal rebleeding rates were significantly lower in patients without PVT than those with PVT after TIPSS (1 year: 0% vs 9.3%; 2 years: 15.9% vs 36.6%; P = .023, by log-rank test; Figure 3A).
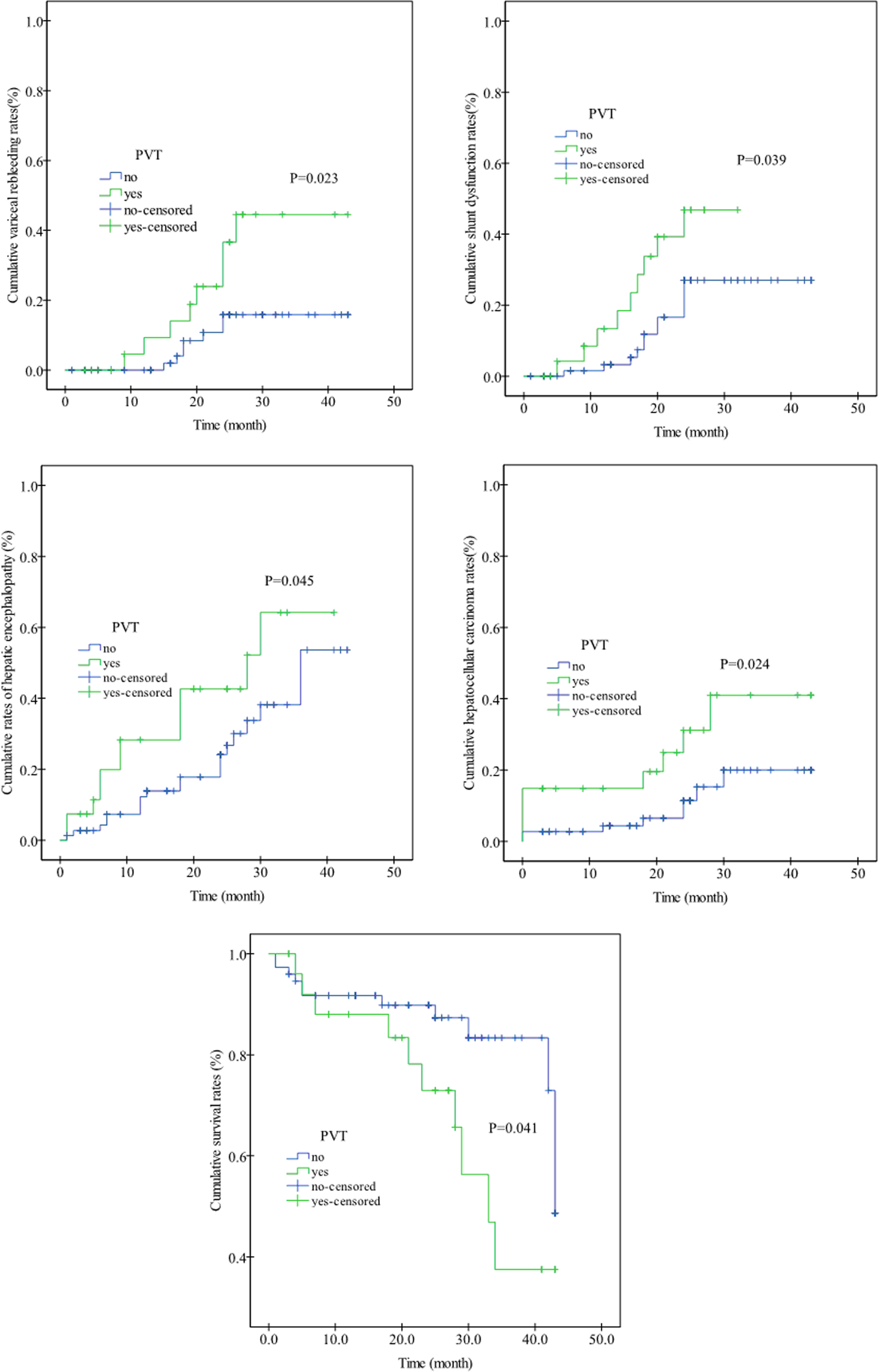
A, Cumulative variceal rebleeding rates in patients with and without PVT after transjugular intrahepatic portosystemic shunt (P = .023, by log-rank test). B, Cumulative shunt dysfunction rates in patients with and without PVT after transjugular intrahepatic portosystemic shunt (P = .039, by log-rank test). C, Cumulative rates of a first episode of hepatic encephalopathy in patients with and without PVT after transjugular intrahepatic portosystemic shunt (P = .045, by log-rank test). D, Cumulative hepatocellular carcinoma rates (including baseline and de novo hepatocellular carcinoma) in patients with and without PVT after transjugular intrahepatic portosystemic shunt (P = .024). E, Cumulative survival rates in patients with and without PVT after transjugular intrahepatic portosystemic shunt (P = .041). PVT indicates portal vein thrombosis.
Shunt dysfunction and repair
During the study, 16 patients with variceal rebleeding after TIPSS were subjected to direct portal venography using digital subtraction angiography imaging technique, which revealed shunt stenosis in 12 cases and occlusion in 4. Markedly slowed (n = 4) or no blood flow (n = 1) within the shunt was detected by Doppler ultrasonography in 5 patients without rebleeding. Direct portal venography again demonstrated shunt stenosis in 4 patients and occlusion in 1. Therefore, 21 patients with shunt dysfunction were repaired by balloon dilation (n = 14) and stent placement (n = 6). Notably, there were 2 patients who received TIPSS repair twice, with balloon dilation for the first time and then followed by stent placement. One patient with occlusive PVT within the stent was treated by guide wire puncture and subsequent injection of 100 000 unit of urokinase, which though failed to recanalize the thrombus.
The 1-year and 2-year cumulative shunt dysfunction rates were markedly lower in patients without PVT than those with PVT after TIPSS (1 year: 3.3% vs 13.3%; 2 years: 27.0% vs 46.8%; P = .039, by log-rank test; Figure 3B).
Hepatic encephalopathy
During follow-up, 32 patients developed at least 1 episode of hepatic encephalopathy, which was due to 1 or more of the following causes: constipation (n = 11), hematemesis (n = 5), infection (n = 7), consumption of meat (n = 7), and unknown precipitators (n = 2). The cumulative 1- and 2-year rates of a first episode of hepatic encephalopathy were prominently lower in patients without PVT than those with PVT (1 year: 12.2% vs 28.3%; 2 years: 24.1% vs 42.6%; P = .045, by log-rank test; Figure 3C).
Hepatocellular carcinoma
During the study, de novo hepatocellular carcinoma occurred in 4 of 23 patients with de novo PVT after TIPSS, compared to 6 of 72 patients without PVT. The cumulative hepatocellular carcinoma rates were similar between these 2 groups (P = .099, by log-rank test). However, there were 4 (14.8%) patients with de novo PVT and 2 (2.7%) patients without PVT who also had hepatocellular carcinoma at baseline. If these 6 patients with baseline hepatocellular carcinoma were counted, the cumulative 1-year and 2-year hepatocellular carcinoma rates were significantly lower in patients without PVT than those with PVT (1 year: 4.4% vs 14.8%; 2 years: 11.4% vs 31.2%; P = .024, by log-rank test; Figure 3D).
Overall survival
In total, there were 22 death cases, among which 10 occurred in 27 patients with PVT after TIPSS and 12 in 74 patients without PVT. The 1-year and 2-year cumulative survival rates were significantly higher in patients without PVT than those with PVT (1 year: 91.7% vs 88.0%; 2 years: 89.8% vs 72.9%; P = .041, by log-rank test; Figure 3E).
Discussion
In this study, PVT formation was detected in 26.7% of patients with cirrhosis undergoing TIPSS, which was similar to those without TIPSS. 2,3 Despite previous studies reporting that TIPSS was safe and effective in recanalizing PVT, 12,13 our study further showed that TIPSS could not stop development of PVT. Cirrhosis is associated with increased intrahepatic vascular resistance and reduced hepatopetal blood flow. 14 The latter seems to be the most important risk factor for PVT in cirrhosis and has been found to be predictive of future PVT. 15 However, we found that portal pressure before TIPSS and intrashunt pressure post-TIPS (reflecting vascular resistance) were not significant predictors for PVT in univariate analysis (Table 2) and multivariate analysis (data not shown).
In our study, multivariate analysis showed that WBC, CTP score, and ascites were independent predictors for PVT in TIPSS-treated patients with cirrhosis. The WBC was inversely correlated to risk of thrombosis, and patients with lower WBC count had significantly higher risk of thrombosis. As we know, WBC count reflects the severity of hypersplenism, a consequence of portal hypertension in cirrhosis. We could speculate that lower WBC probably indicates more severity of cirrhosis. Moreover, WBC plays a vital role in phagocytosis and immunity and in defense against infection, the risk of which, commonly gram-negative sepsis in this setting, increases when the absolute granulocyte count falls below 1000/µL. 16 For patients with marked liver disturbance, the WBC function is also greatly compromised. 17 We could argue that defect of WBC in quantity and quality may result in decreased removal of endotoxin in the blood stream. Indeed, endotoxemia is common with worsening liver disease 18,19 and has been reported to favor PVT. 20 Our results illustrated that patients with higher CTP scores and more severe ascites had higher thrombosis risks, indicating that PVT was more likely to form in patients with more severe cirrhosis, which was in line with previous studies. 1,2
Up-to-date, optimal management of PVT in cirrhosis is not addressed in any consensus publication. 21 Anticoagulation with heparin derivatives, and vitamin K antagonists, has been repeatedly adopted for the treatment of PVT in cirrhosis. In these studies, anticoagulation resulted in 39% to 82% of partial or complete recanalization of PVT, as compared to 0% to 4.8% among controls. 7,22,23 Notably, Werner et al 23 reported that warfarin led to complete or partial recanalization of PVT in 23 (82.1%) of 28 patients and no change in 5 (18%) of 28 patients with advanced cirrhosis. In our study, warfarin resulted in 9 (81.8%) of 11 complete or partial recanalization in PVT that occurred post-TIPSS, markedly superior to aspirin or clopidogrel, which was consistent with these studies. Recently, direct-acting oral anticoagulants (DOACs) are used to treat patients with cirrhosis and splanchnic vein thrombosis, but data on its safety and efficacy are limited, and randomized clinical trials are required to confirm its applicability in this setting. 24
Variceal hemorrhage, intestinal ischemia, and portal biliopathy were common complications of PVT. 25 Previous studies reported that patients with cirrhosis and PVT were at an increased risk of variceal hemorrhage compared to those without. 3 In our study, the cumulative 1-year and 2-year variceal rebleeding rates in patients with PVT were 9.3% and 36.6%, respectively, significantly higher than those without PVT, which was in line with previous studies. We could argue that variceal hemorrhage might be a consequence of thrombosis. However, Francoz et al 22 pointed out that episodes of variceal hemorrhage, reflecting the severity of portal hypertension, were more likely to be predisposing factors for, instead of a consequence of, thrombosis itself.
The TIPSS is established to be associated with increased risk for hepatic encephalopathy. 6,13,26 The PVT was also reported to relate to occurrence of hepatic encephalopathy. 27 Villa et al 28 reported that rates of hepatic decompensation (including hepatic encephalopathy) were significantly lower in the treatment arm (without PVT) compared with controls (27% rate of PVT). Our study showed that occurrences of hepatic encephalopathy in TIPSS-treated patients with PVT at 1 year and 2 years were markedly higher than those without PVT, which was compatible with these studies.
The presence of hepatocellular carcinoma without vascular invasion seems to be a risk factor for nonmalignant PVT. 29 Connolly et al 30 reported that advanced stage, higher CTP class, major vessel involvement, low serum albumin, and high α-fetoprotein levels were predictors for PVT in patients with hepatocellular carcinoma. However, the exact association of PVT with hepatocellular carcinoma is not well established in literature. In our study, we observed that post-TIPSS development of hepatocellular carcinoma was similar between patients with and without PVT, although those with PVT did have higher rate of hepatocellular carcinoma before TIPSS (14.8% vs 2.7%).
With regard to survival, results of previous studies were conflicting. Englesbe et al 31 reported that cirrhotic patients with PVT had an increased death risk, whereas Berry et al 32 showed that patients with advanced cirrhosis and PVT had lower mortality than those without PVT. Moreover, previous studies also reported that the presence of PVT might be associated with the long-term mortality (3 years) in nonliver transplant patients with cirrhosis, but not with the short-term mortality (5 days, 6 weeks, and 1 year); the presence of PVT was not significantly associated with overall mortality for the cirrhotic patients undergoing surgical or interventional shunts. 33 Notably, Perarnau et al 34 showed that cumulative survival rates were not significantly different between TIPSS-treated cirrhotic patients with and without PVT (1 year: 80% vs 84%; 2 years: 72% vs 70%; and 4 years: 55% vs 52%; P = .58, by log-rank test). In our study, the 1-year and 2-year cumulative survival rates were significantly lower in patients with PVT than those without PVT. This discrepancy might be associated with different patient compositions in etiology, gender ratio, degree of PVT, race, concomitant diseases, etc.
Our study has the following limitations: first, it is not a controlled study; second, allocation of anticoagulant or antiplatelet drugs was not randomized; and third, the follow-up duration was relatively short, ranging from 1 to 43 months. However, we prospectively investigated several clinically pertinent but unclear issues by enrolling a relatively large cohort of patients, which may provide some useful information for clinicians, weighing over these limitations.
In conclusion, our study showed that WBC count, CTP score, and ascites were independent baseline predictors for PVT post-TIPSS; before the safety and efficacy of DOACs were confirmed, oral warfarin could be a better choice than aspirin or clopidogrel; patients developing PVT post-TIPSS had poorer clinical outcomes than those not.
Supplemental Material
Supplementary_Table_1 - Portal Vein Thrombosis in Patients With Cirrhosis Undergoing Elective Transjugular Intrahepatic Portosystemic Shunt: Risk Factors, Warfarin Efficacy, and Clinical Outcomes
Supplementary_Table_1 for Portal Vein Thrombosis in Patients With Cirrhosis Undergoing Elective Transjugular Intrahepatic Portosystemic Shunt: Risk Factors, Warfarin Efficacy, and Clinical Outcomes by Wan Yue-Meng, Yu-Hua Li, Hua-Mei Wu, Jing Yang, Li-Hong Yang, and Ying Xu in Clinical and Applied Thrombosis/Hemostasis
Footnotes
Authors’ Note
Wan Yue-Meng contributed to study concept and design, acquisition of data, analysis and interpretation of data, statistical analysis, and drafting of the manuscript. Ying Xu contributed to the critical revision of the manuscript for important intellectual content; administrative, technical, or material support; and study supervision. Yu-Hua Li, Hua-Mei Wu, Jing Yang, and Li-Hong Yang contributed to the acquisition of data, analysis and interpretation of data, and statistical analysis. All procedures followed were in accordance with the ethical standards of the ethics committee of the Second Affiliated Hospital of Kunming Medical University on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.