
Abstract
We explored the relationship between abdominal vein thromboses, including portal vein thrombosis (PVT) and superior mesenteric vein thrombosis (SMVT), and thrombophilia. The frequency of thrombophilia, such as antithrombin (AT), protein C (PC), or protein S (PS) gene mutations, was examined in 21 patients with PVT, 6 patients with SMVT, and 6 patients with both PVT and SMVT. Low levels of AT, PC, or PS were frequently detected in patients with PVT or mesenteric vein thrombosis, and 4 mutations in the PS gene, 3 mutations in the PC gene, and 2 mutations in AT the gene were detected. Protein S Tokushima was detected in 3 of 4 patients with a PS gene mutation and was associated with 2 other PS gene mutations. The onset of PVT or SMVT was almost idiopathic in patients with congenital thrombophilia. Both PVT and SMVT were frequently caused by an AT, a PC, or a PS mutation, and the onset of these thromboses due to thrombophilia was frequently idiopathic.
Introduction
Abdominal vein thrombosis includes portal vein thrombosis (PVT) and mesenteric vein thrombosis (MVT). Portal vein thrombosis is venous thrombosis occurring in the trunk of the portal vein including portal branches such as the mesenteric and splenic veins. 1,2 Mesenteric vein thrombosis commonly involves the superior mesenteric vein, known as superior mesenteric vein thrombosis (SMVT), and rarely the inferior mesenteric vein. In SMVT, 3 local blood coagulation impairs the venous return of the bowel and causes ischemic changes and necrosis of the bowel wall. As SMVT is a relatively rare condition with nonspecific symptoms and insufficient clinician awareness, the mortality rate remains high due to a delayed diagnosis. The frequency of nonneoplastic PVT in patients with liver cirrhosis is about 7.2% to 17% 4,5 and is higher at the decompensated or advanced stage. 5,6 Although acute PVT can be severe and may lead to mesenteric ischemia and variceal bleeding, there are many cases of nonsymptomatic PVT. 7 The frequency of SMVT ranged from 1 of 5000 to 1 of 15 000 among inpatients and 1 of 1000 among emergency department admissions, accounting for 6% to 9% of all cases of acute mesenteric ischemia. 8 Portal vein thrombosis is also a frequent complication of splenectomy 7 and liver transplantation. 9 Primary SMVT develops spontaneously and is idiopathic, and secondary SMVT arises from underlying diseases or risk factors. A delayed diagnosis or treatment of SMVT allows intestinal infarction to develop, which can be life-threatening. Thrombophilia, 10 such as plasminogen activator inhibitor I 4G-4G, methylene tetrahydrofolate reductase (MTHFR) 677TT, factor V Leiden 506Q, prothrombin 20210A, and antithrombin (AT), protein C (PC), and protein S (PS) abnormalities, can frequently cause PVT or MVT. Few reports have explored the prevalence of MTHFR 677TT, factor V Leiden 506Q, and prothrombin 20210A in Japan.
In this study, the differences between PVT and SMVT, including abnormalities in AT, PC, and PS, were examined in 21 patients with PVT, 6 patients with SMVT, and 6 patients with both PVT and SMVT in order to confirm the relationship between thrombophilia and SMVT.
Materials and Methods
The study protocol was approved by the Human Ethics Review Committee of the Mie University School of Medicine, and a signed consent form was obtained from each patient. This study was faithfully carried out in accordance with the Declaration of Helsinki. Deep vein thrombosis (DVT) was diagnosed using echography or venography, and disseminated intravascular coagulation (DIC) was diagnosed according to the International Society of Thrombosis and Haemostasis overt DIC diagnostic criteria. 10 Cerebral vascular disease was diagnosed with computed tomography or magnetic resonance imaging (MRI), and cerebral venous sinus thrombosis (CVST) was diagnosed based on MRI, magnetic resonance venography, or cerebral angiography (CAG) findings. 11,12
Measurement of the AT, PC, PS, and Antiphospholipid Antibody Concentrations
Peripheral blood samples were collected in a 1/10 volume of 3.13% sodium citrate. The free PS antigen concentration was measured using a monoclonal antibody-based enzyme-linked immunosorbent assay (ELISA) with the Asserachrom free PS kit (Diagnostica Stago, Asnières, France). The plasma PS and PC activity levels were measured according to the clotting time method using STA-Staclot PS and STA-Staclot PC kit (Diagnostica Stago). The plasma PC antigen concentration was measured based on a latex agglutination test using a LPIA-ACE PC kit (Mitsubishi Chemical Medience Corporation, Tokyo, Japan). The plasma AT activity was measured according to a synthetic substrate assay using a Chromorate ATIII (C) kit (Mitsubishi Chemical Medience Corporation). The dilute Russell’s viper venom time was measured with the clotting time method using a Gradipore LA test (Gradipore, Sydney, Australia). The titers of anti-cardiolipin-β2-glycoprotein I antibodies were measured with an ELISA kit (Yamasa Co, Tokyo, Japan). 13
Gene Analyses of AT, PC, and PS
Genomic DNA was prepared from peripheral blood leukocytes using a QIAamp DNA blood mini kit (QIAGEN, Venlo, Netherlands) according to the manufacturer’s instructions. Each exon and exon/intron boundary of the gene was amplified from genomic DNA using polymerase chain reaction (PCR), as previously described. The PCR products were directly sequenced using a Big-Dye terminator cycle sequencing kit and Applied Biosystems 3130 genetic analyzer (Applied Biosystems, Foster City, California). 14 Gene analyses were carried out in cases with AT, PC, or PS levels less than 70% without warfarin treatment or liver failure.
Statistical Analyses
The data are expressed as the median (25th percentile to 75th percentile). Differences between the groups were examined for statistical significance using the Mann-Whitney U test. A P value <.05 denoted the presence of a statistically significant difference.
Results
In all, 12 patients with SMVT (median age, 49.5 years; 2th percentile to 75th percentile, 40.0-67.0 years; 3 females and 9 males) and 27 patients with PVT (median, 61.5 years; 25th percentile to 75th percentile, 55.0-77.0 years; 11 females and 16 males) were examined at Mie University Hospital between January 4, 1992, and December 28, 2016 (Tables 1 and 2). Both SMVT and PVT were diagnosed by echography or computed tomography. Ten patients with PVT and 1 patient with SMVT were diagnosed after surgery, and SMVT was unexpectedly diagnosed in most patients. Twelve patients with SMVT were associated with 6 PVT, 4VST, 1VT, and 1 cerebral thrombosis, and 4 patients had relapse. Of 27 patients with PVT, 6 were associated with SMVT, 4 DIC, 3 DVT, 3 CVST, 1 cerebral thrombosis, 1 major bleeding, and 1 pulmonary embolism (PE). Six patients were associated with both MVT and PVT. There were no significant differences in the age or sex between patients with SMVT and PVT (Tables 1 and 2). The cause of the onset of PVT was postoperative complication in 10 patients, idiopathic in 5 patients, pancreatic cancer in 4 patients, biliary duct cancer in 3 patients, living donor liver transplantation in 2 patients, liver failure in 2 patients, other cancers in 4 patients, and other causes in 4 patients. The cause of SMVT onset was idiopathic in 8 patients, biliary duct cancer in 2 patients, APS in 1 patient, and postoperative complication in 1 patient. The idiopathic onset in 5 patients with PVT and 8 patients with SMVT was suspect to be due to congenital thrombophilia. Some patients had more than 2 causes of thrombosis. None of the patient has in this study had an abnormal hematological phenotype.
Patients With Superior Mesenteric Venous Thrombosis.
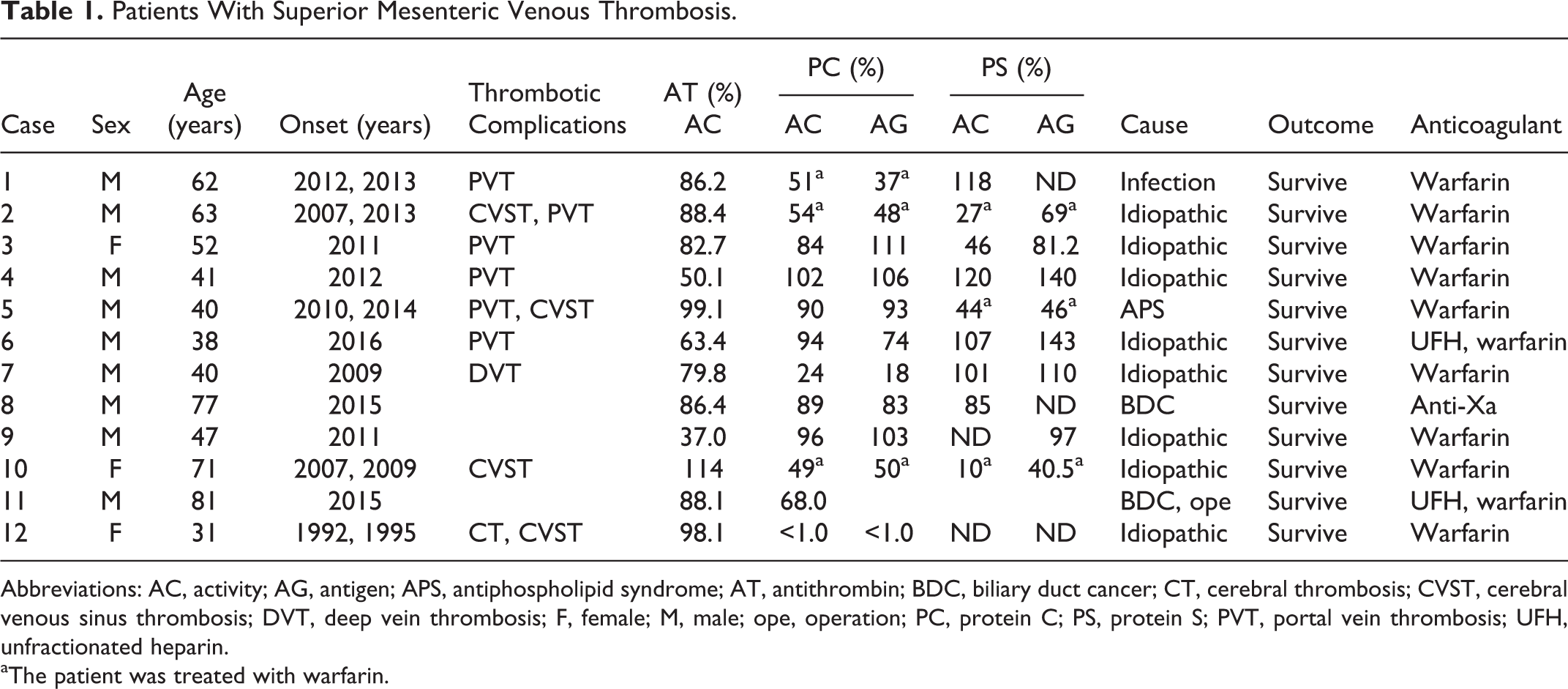
Abbreviations: AC, activity; AG, antigen; APS, antiphospholipid syndrome; AT, antithrombin; BDC, biliary duct cancer; CT, cerebral thrombosis; CVST, cerebral venous sinus thrombosis; DVT, deep vein thrombosis; F, female; M, male; ope, operation; PC, protein C; PS, protein S; PVT, portal vein thrombosis; UFH, unfractionated heparin.
aThe patient was treated with warfarin.
Patients With Portal Vein Thrombosis.a
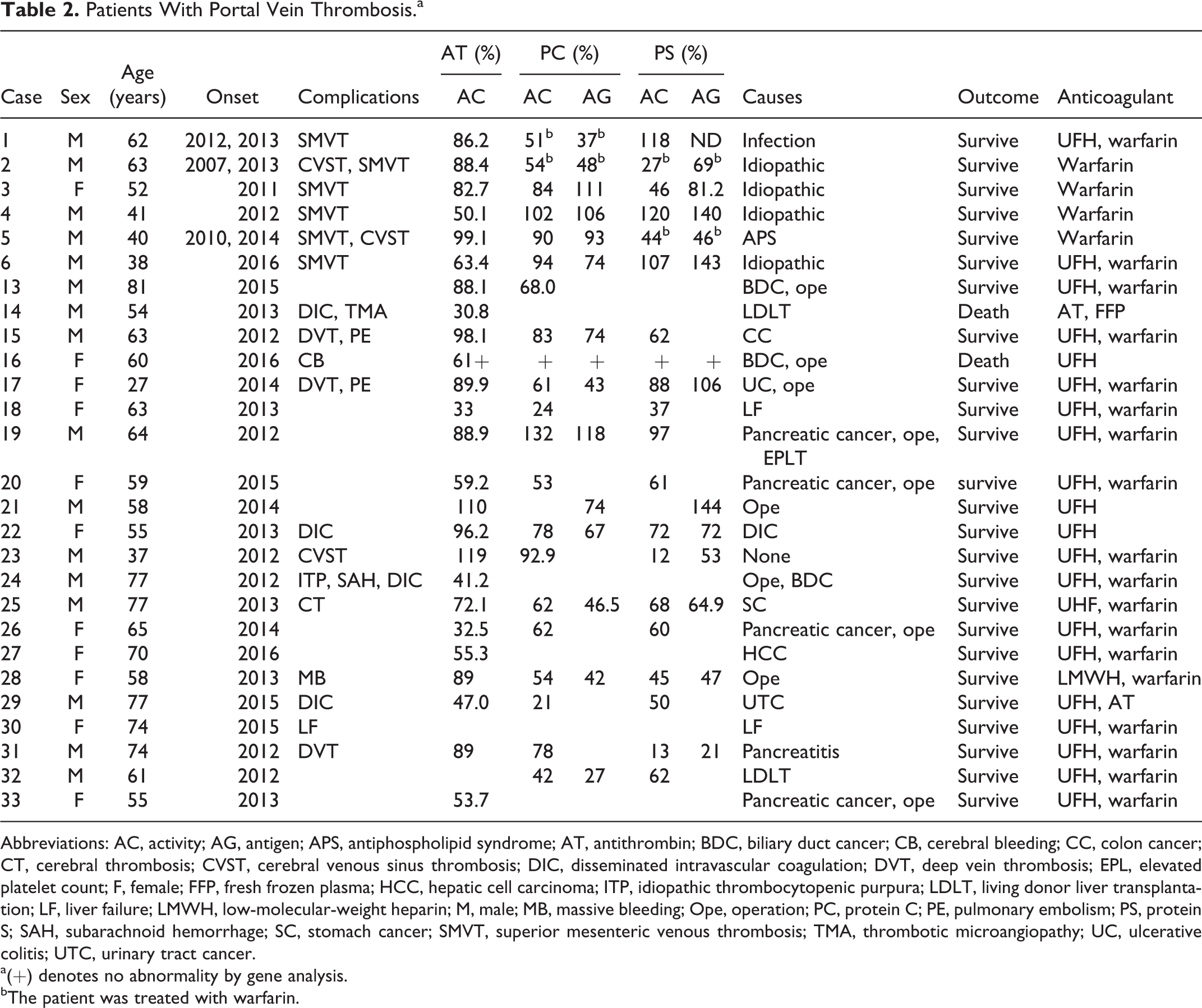
Abbreviations: AC, activity; AG, antigen; APS, antiphospholipid syndrome; AT, antithrombin; BDC, biliary duct cancer; CB, cerebral bleeding; CC, colon cancer; CT, cerebral thrombosis; CVST, cerebral venous sinus thrombosis; DIC, disseminated intravascular coagulation; DVT, deep vein thrombosis; EPL, elevated platelet count; F, female; FFP, fresh frozen plasma; HCC, hepatic cell carcinoma; ITP, idiopathic thrombocytopenic purpura; LDLT, living donor liver transplantation; LF, liver failure; LMWH, low-molecular-weight heparin; M, male; MB, massive bleeding; Ope, operation; PC, protein C; PE, pulmonary embolism; PS, protein S; SAH, subarachnoid hemorrhage; SC, stomach cancer; SMVT, superior mesenteric venous thrombosis; TMA, thrombotic microangiopathy; UC, ulcerative colitis; UTC, urinary tract cancer.
a(+) denotes no abnormality by gene analysis.
bThe patient was treated with warfarin.
The AT deficiency was observed in 3 of 12 patients with SMVT and 11 of 27 patients with PVT. The PC deficiency was observed in 6 of 12 patients with SMVT and 11 of 27 patients with PVT; PS deficiency was observed in 4 of 12 patients with SMVT and 13 of 27 patients with PVT. When AT, PC, and PS were measured, 5 patients with SMVT and 3 patients with PVT were already being treated with warfarin. Ultimately, all 12 patients with SMVT and the 27 patients with PVT survived and were treated with unfractionated heparin, warfarin, and anti-Xa agent. The AT, PC, or PS level was low in 1 patient with DIC and 1 patient with liver failure.
In the gene analysis (Table 3), mutations in AT, PC, or PS were detected in 9 of 32 patients; 7 patients had SMVT, 5 had PVT, and 3 had both PVT and SMVT. Eight patients with a gene mutation for AT, PC, or PS had multiple thromboses, including DVT, PE, CVST, PVT, or SMVT, but 1 patient had only MVT. Of 9, 8 patients with a gene mutation for AT, PC, or PS had an idiopathic onset for SMVT or PVT, and they had no malignancy. There were 4 mutations in the PS gene, 3 in the PC gene, and 2 in the AT gene. The PS Tokushima was detected in 3 of 4 patients with a PS gene mutation and was associated with 2 other PS gene mutations. Case 12 was combined heterozygous for PC and had multiple and recurrent thromboses. The age was significantly lower in patients with a gene mutation for AT, PC, or PS than in those without such mutations, and the rates of multiple thromboses (P < .001), idiopathic onset (P < .001), and nonmalignancy (P < .01) were significantly higher in those with mutations than in those without mutations (Table 4).
Gene Mutation for AT, PC, and PS.
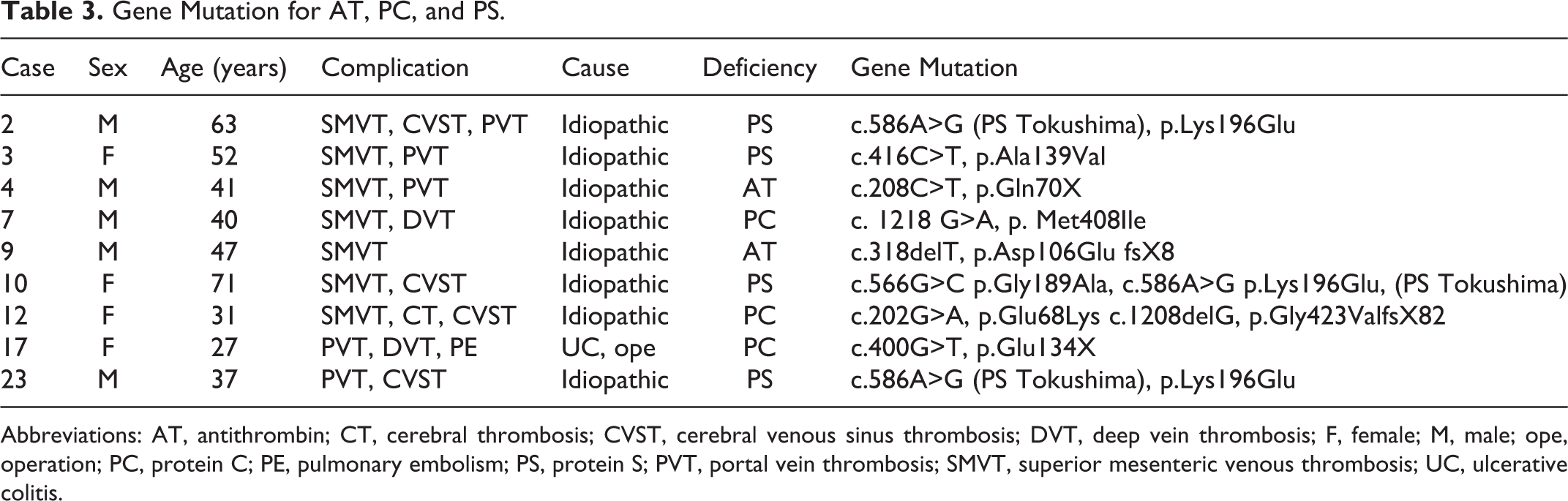
Abbreviations: AT, antithrombin; CT, cerebral thrombosis; CVST, cerebral venous sinus thrombosis; DVT, deep vein thrombosis; F, female; M, male; ope, operation; PC, protein C; PE, pulmonary embolism; PS, protein S; PVT, portal vein thrombosis; SMVT, superior mesenteric venous thrombosis; UC, ulcerative colitis.
Differences Between Patients With and Without Gene Mutations.a
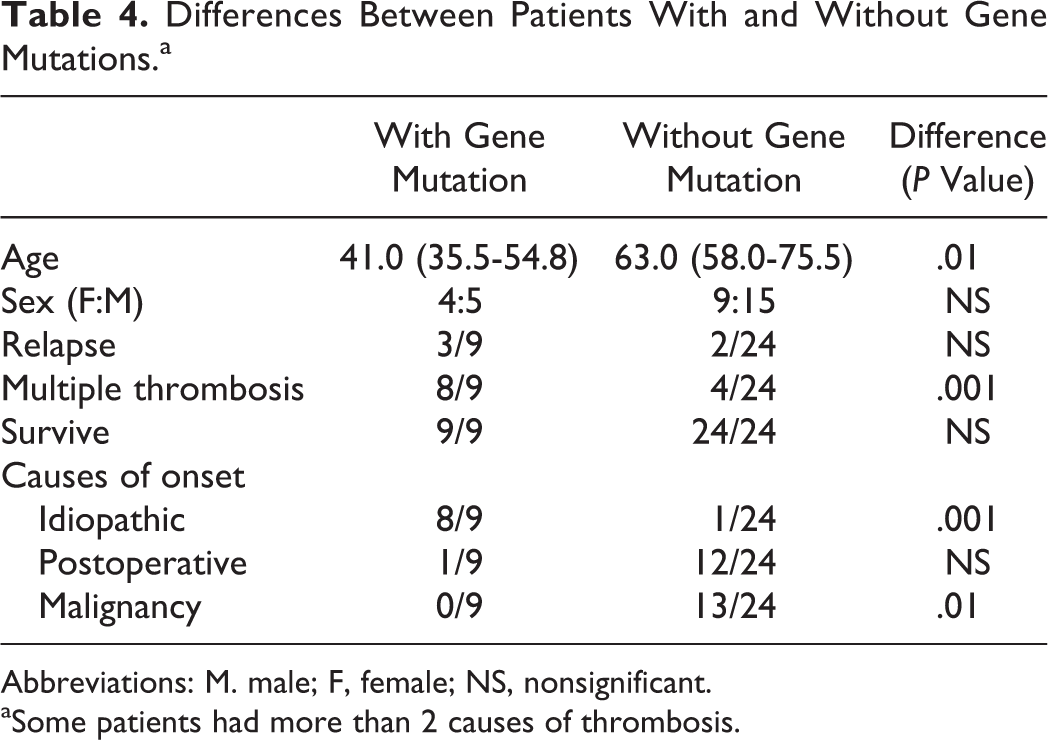
Abbreviations: M. male; F, female; NS, nonsignificant.
aSome patients had more than 2 causes of thrombosis.
Discussion
Our study showed that SMVT was frequently caused by an AT, a PC, or a PS mutation, and the onset of SMVT due to thrombophilia was frequently idiopathic. Both SMVT and PVT, especially SMVT, were frequently associated with other thromboses, such as CVST, PVT, SMVT, DVT, and PVT. Furthermore, the frequency of complication with relatively rare thromboses, aside from DVT/PE, was high. Given the small population in our study, there were no significant differences in the age and sex between patients with SMVT and PVT, although patients with SMVT tended to be younger than those with PVT or DVT after surgery. 15 All cases in this study survived, in agreement with previous report. 16
We previously reported the frequency of congenital thrombophilia to be 31.8% in patients with CVST 12 and 30.0% in patients with DVT or PE, including 11.5% with AT mutations, 12.3% with PC mutations, and 6.2% with PS mutations. 14 At the onset of thrombosis, decreased levels of AT, PC, or PS were observed in patients without congenital thrombophilia. 14,17 Few reports have described thrombophilia in PVT and SMVT. 18 –20
Patients with SMVT or PVT were frequently associated with a deficiency in PC or PS; however, these patients were often treated with warfarin, indicating that a gene analysis is useful for diagnosing congenital thrombophilia in such patients.
A gene analysis detected mutations in AT, PC, or PS in about 27% of patients with PVT or SMVT. Case 12 was previously reported as having a combined heterozygous PC deficiency 21 and cases 2, 10, and 23 were previously reported as having CVST. 22 In our study, the rate of PS mutation tended to be higher in PVT or MVT than in DVT/PE. 14 Although our sample size was small, this tendency is similar to that noted with CVST. 12 The PS Tokushima mutation was detected in 3 of 4 patients with a PS mutation, which is frequently observed in Japanese people. 23,24 Although the frequency of multiple thromboses was significant in cases of congenital thrombophilia with PVT or SMVT, there was no significant difference in the rate of relapse between PVT/SMVT with and without congenital thrombophilia, possibly due to our small sample size. The age was significantly younger, and the rate of idiopathic onset and nonmalignancy was significantly higher in patients with congenital thrombophilia than in those without. These findings were similar to those in previous reports on DVT/PE. 14 The Janus activating kinase 2 (JAK2) p.V617V mutation is a well-known risk factor for thrombosis in patients with myeloproliferative neoplasm. 25 However, since no abnormal hematological phenotypes were observed in this study, this mutation was not analyzed.
In conclusion, PVT and SMVT are frequently associated with congenital thrombophilia, such as AT, PC, or PS mutations. Young patients with an idiopathic onset of PVT or MVT with multiple thromboses should be considered at risk of having congenital thrombophilia.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by a Grant-in-Aid from the Ministry of Health, Labour and Welfare of Japan for Blood Coagulation Abnormalities, the Ministry of Education, Culture, Sports, Science and Technology of Japan, and the Rare/Intractable Disease Project of Japan from Japan Agency for Medical Research and Development (AMED).