
Abstract
Deep vein thrombosis (DVT) and pulmonary embolisms (PEs) are common complications after surgical procedures. The influence of prescribed blood products on the occurrence of DVT and PE was evaluated in postsurgical patients in this retrospective case–control study. The records of 286 surgical patients were analyzed: DVT (n = 52), PE (n = 92), and a control group (n = 142). The amounts of prescribed blood, blood products, and vitamin K were reviewed, together with appropriate prescribing of low-molecular-weight heparins. The influence of prescribed blood products on the occurrence of DVT or PE was analyzed using multinomial logistic regression. We demonstrated a significant difference between the test and control groups (P < .05) in relation to receiving packed red blood cells. Treatment with red blood cells was associated with an increased risk of PE but not DVT. Patients who developed PE after surgery were hospitalized for longer (median 10 days) than patients with DVT (median 6 days). There was no difference between the test and control groups concerning treatment with fresh frozen plasma. Inadequate thromboprophylaxis significantly increased the likelihood of DVT. There is a connection between receiving packed red blood cells and occurrence of postoperative PE in surgical patients. Thus, patients receiving red blood cells should be monitored more closely after surgery, as they are more likely to develop PE postoperatively.
Introduction
Hemostasis is the process of blood clot formation at the site of vessel injury. 1 Although the clotting process is a dynamic, highly interwoven array of multiple processes, it can be viewed as occurring in phases: endothelial injury and formation of the platelet plug, propagation of the clotting process by the coagulation cascade, termination of clotting by antithrombotic control mechanisms, and removal of the clot by fibrinolysis. 2 Platelets are activated at the site of vascular injury to form a platelet plug, the initial hemostatic response to stop bleeding. 3 Vascular injury is 1 of 3 causes of venous thromboembolism (VTE) included in Virchow’s triad, a major theory delineating the pathogenesis of VTE. 4,5 Thus, VTE occurs as a result of alterations in blood flow (stasis), vascular endothelial injury, and alterations in blood constituents (inherited or acquired hypercoagulable state). The VTE is a formation of the clot in a deep vein, causing complete or partial obstruction of the vein; deep vein thrombosis (DVT) is the development of a clot mostly in the veins of the lower extremities. The most common complication of untreated acute proximal DVT is pulmonary embolism (PE). 3,6
The DVT and PE are rather common complications after surgical procedures 7,8 and present major health-care problems resulting in significant mortality, morbidity, and expenditure of resources. 8,9 Approximately two-thirds of symptomatic VTE cases are manifested by DVT, one-third by PE, which is the leading cause of death in hospitals. 10 –12 The main risk factors for VTE are recent surgery, lower extremity trauma, history of immobilization or prolonged hospitalization/bed rest, obesity, prior episode(s) of VTE, malignancy, use of oral contraceptives or hormone replacement therapy, pregnancy or postpartum status, and stroke. 13,14 A risk factor for thrombosis can now be identified in over 80% of patients with venous thrombosis. The 6 most prevalent preexisting medical characteristics of such patients 15 are more than 48 hours of immobility in the preceding month (45%), hospital admission in the past 3 months (39%), surgery in the past 3 months (34%), malignancy in the past 3 months (34%), infection in the past 3 months (34%), and current hospitalization (26%). Only 11% of the 587 episodes of VTE analyzed had none of these 6 characteristics; 36% had 1 to 2 risk factors and 53% had ≥3. 15
The VTE is a common complication during and after hospitalization for acute illness or surgery and can be avoided with proper prevention in hospitals. 16 To prevent VTE in surgery, we use low-molecular-weight heparins, which act as Xa and thrombin (IIa) antagonists (so-called anti-Xa activity). 17 Increased levels of blood clotting factors VIII, IX, XI, thrombin-activated fibrinolysis inhibitor, and interleukin 8 are associated with an increased risk of thrombosis. 18
Fresh frozen plasma (FFP) is used in patients who are bleeding because of low levels of coagulation factors and anticoagulant therapy. In a population study, elevated levels of plasma components, including clotting factors and inflammatory cytokines, caused 2 to 3 times increased risk for the first episode of VTE. 19 Physicians differed greatly in prescribing FFP to patients in the intensive care unit: FFP was prescribed to 31% of patients with normal prothrombin times and also to 41% of patients despite the fact that they were not bleeding. 19
Vitamin K is used in addition to FFP for patients who are bleeding because their levels of clotting factors are too low. Vitamin K is also used in preoperative preparation of patients who are on permanent anticoagulant therapy with warfarin. 20,21 The international normalized ratio is effectively reduced, thus surgical procedures can be done without major bleeding. 22,23
Atrial fibrillation, the most common cardiac arrhythmia, can have adverse consequences related to a reduction in cardiac output and to atrial appendage thrombus formation. 23 –25 Affected patients may be at increased risk of death. In a study in patients with self-reported major medical illnesses (liver or kidney disease, rheumatoid arthritis, multiple sclerosis, heart failure, hemorrhagic stroke, and arterial thrombosis), the risk of venous thrombosis was increased, with odds ratios in the range 1.5 to 4.9. The combination of a major medical illness, as defined above, plus immobilization increased the odds ratio for development of venous thrombosis to 10.9 (95% confidence interval: 4.2-28). 26 The aim of the study was to evaluate the influence of prescribed blood products on the occurrence of DVT or PE after surgical treatment.
Materials and Methods
Study Design
The study was designed as a retrospective case–control study and was granted ethical approval by the Republic of Slovenia National Medical Ethics Committee (0120-139/2015-2, KME 119/06/15). We reviewed blood transfusion, blood products, vitamin K, and appropriate prescribing of low-molecular-weight heparins in surgical patients who were diagnosed with DVT or PE between January 1, 2007, and December 31, 2011, at the Murska Sobota General Hospital (SBMS) as a complication of surgical treatment. The DVT and PE groups were compared with a control group in whom there was no DVT or PE after surgical treatment.
Patients
Using the hospital computer program BIRPIS21 and on the basis of the inclusion criteria, we identified 257 patients with DVT or PE treated in the surgical department at the SBMS during the 5-year period studied. We excluded patients after polytrauma and patients who were already diagnosed with PE or DVT and were hospitalized because of this diagnosis and did not have surgery or major changes in drug therapy in the 3 months before the onset of DVT or PE. We also excluded patients with recurrence of DVT or PE and patients with inherited thrombophilia or proven malignancy. Overall, 113 patients were excluded.
Finally, 144 patients with either DVT or PE were identified. The DVT or PE was diagnosed the first time; patients in the test group developed the complications within 180 days after surgical treatment. The control group comprised 142 patients treated in the surgical department at SBMS and who did not have VTE as the principal or accompanying diagnosis.
We reviewed the entire medical records of patients, including therapeutic sheets and other documentation that was available in the hospital computer program. We reviewed received blood, blood products, and vitamin K during hospitalization in the surgical department. We recorded patients’ age, weight, height, number of hospitalized days, time of intervention, onset of DVT or PE, and the accompanying medical diagnosis. We also reviewed proper dosage and the dosing interval of low-molecular-weight heparins, together with the accompanying diagnosis as atrial fibrillation, heart failure, diabetes mellitus, or other cardiovascular disease (myocardial infarction or transient ischemic attack in the past, angina pectoris, mitral stenosis, or atherosclerotic vascular disease). Patients were assigned to test groups according to the type of operation, and the risk of a VTE event was estimated using the Caprini point system. For the control group, 142 patients with operations similar to the test group were randomly chosen and classified according to the same criteria, based on type of operation. The adequacy of thromboprophylaxis was assessed in the control patients as for the test groups.
Statistical Analysis
SPSS Statistics version 22 (Chicago, Illinois) was used for the analysis. The influence of prescribed blood products on the occurrence of DVT or PE in comparison with the control group was analyzed using multinomial logistic regression. Adjusted odds ratios were calculated by including other covariates in the regression model. The significance level was set at .05.
Results
Among the 144 patients in the test group, 92 (63.9%) had PE, 51 (35.4%) had DVT, and 1 patient had Budd-Chiari syndrome and was included in the analysis. Forty-one (28.5%) of these patients died. On the basis of autopsy findings for the effects of proven PE, 25 patients died (27.2% of those who had PE; 61.0% of all deaths in the test group). Autopsies were not performed for all deceased patients, and in some cases, the exact cause of death was not known; however, the suspected diagnosis responsible for death was PE. Patients in the control group did not have any health complications in terms of PE or DVT within 180 days, or longer, after the surgery. Characteristics of the patients and risk factors for DVT and PE are shown in Tables 1 and 2.
Baseline Characteristics of the Patients.
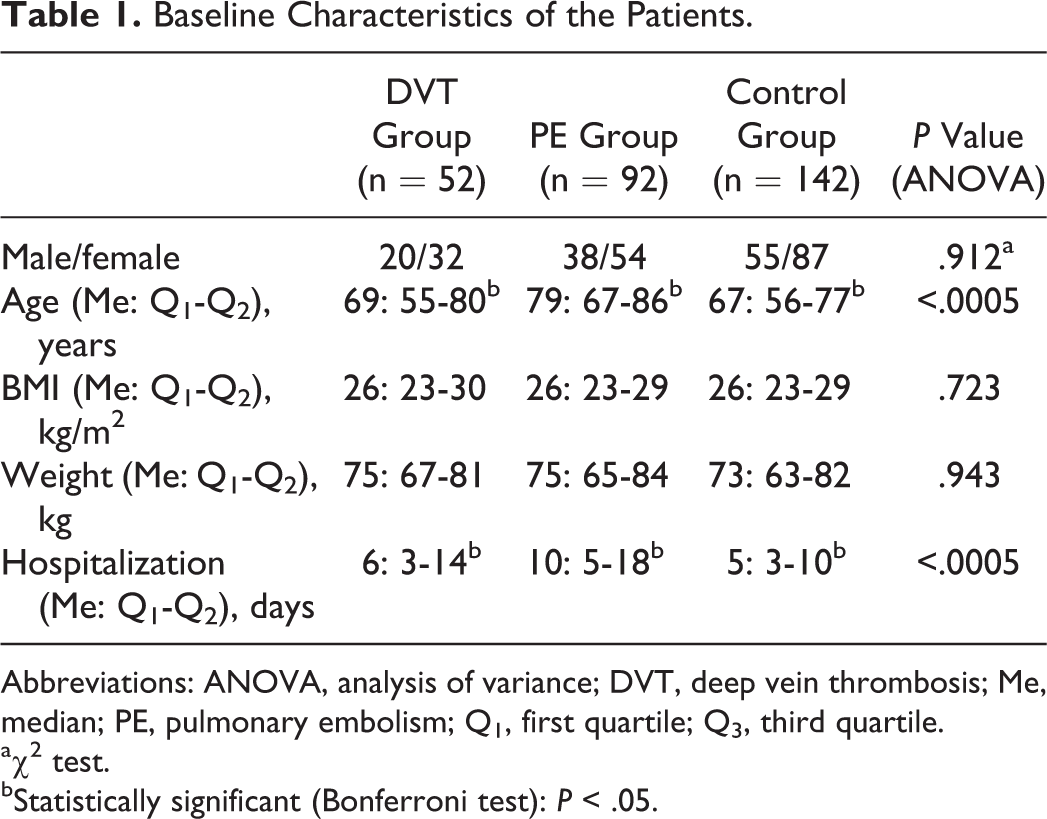
Abbreviations: ANOVA, analysis of variance; DVT, deep vein thrombosis; Me, median; PE, pulmonary embolism; Q1, first quartile; Q3, third quartile.
aχ2 test.
bStatistically significant (Bonferroni test): P < .05.
Risk Factors for DVT and PE.
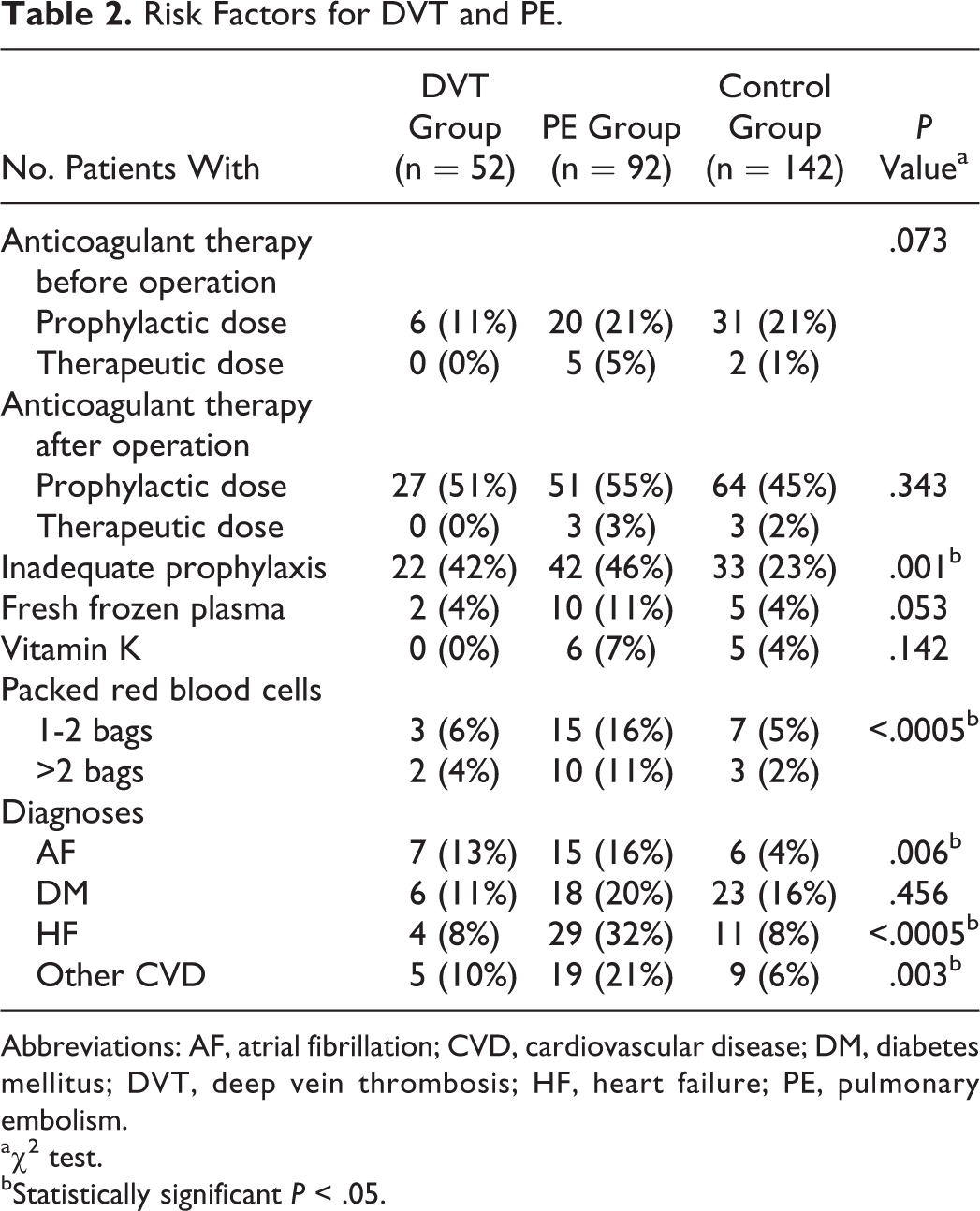
Abbreviations: AF, atrial fibrillation; CVD, cardiovascular disease; DM, diabetes mellitus; DVT, deep vein thrombosis; HF, heart failure; PE, pulmonary embolism.
aχ2 test.
bStatistically significant P < .05.
One or two bags (270-350 mL) of packed red blood cells (stored as blood product units available for transfusion) were given to 5 patients who developed DVT, 25 patients with PE, and 10 patients in the control group.
A unit of FFP is the fluid portion of 1 unit of human blood that is centrifuged, separated, and frozen solid at −18°C (0°F) or colder within 8 hours of collection. The FFP volume given to our patients was usually 240-270 mL per bag. Two (4%) patients who developed DVT received FFP: 1 of them received just 1 bag, the other patient ≥3. In patients with PE, 10 (12%) received FFP: 2 patients just 1 bag, 5 received 2 bags, and 3 patients received ≥3. In the control group, 5 (4%) patients received FFP: 3 patients received 1 bag and 2 patients received 2 bags.
Vitamin K1 (phytomenadione) was given intravenously in doses from 10 to 80 mg. In the PE group, 6 (7%) patients received the vitamin: 3 received 10 to 20 mg and the other 3 ≥30 mg. In the control group, 5 (4%) patients received the vitamin: 3 received 10 to 20 mg and 2 received ≥30 mg. No patient with DVT received vitamin K1.
The appropriateness of VTE prophylaxis was evaluated using the Caprini score. 14,27,28 We evaluated the adequacy of dose, the dosing interval, and the appropriate duration of therapy based on the risk assessment score provided by the guidelines. 14 We also reviewed the proper dosage and dosing interval of low-molecular-weight heparins and the accompanying diagnosis. Among the patients without cardiovascular disease, 24 had DVT, 21 had PE, and 67 were in the control group.
The results of multinomial logistic regression analysis are shown in Table 3. The test and control groups differed significantly in relation to treatment with packed red blood cells (P < .05). Patients with heart failure and atrial fibrillation or with other cardiovascular disease were significantly more at risk for developing PE.
Prediction of the Impact of Factors on the Incidence of DVT and PE.a
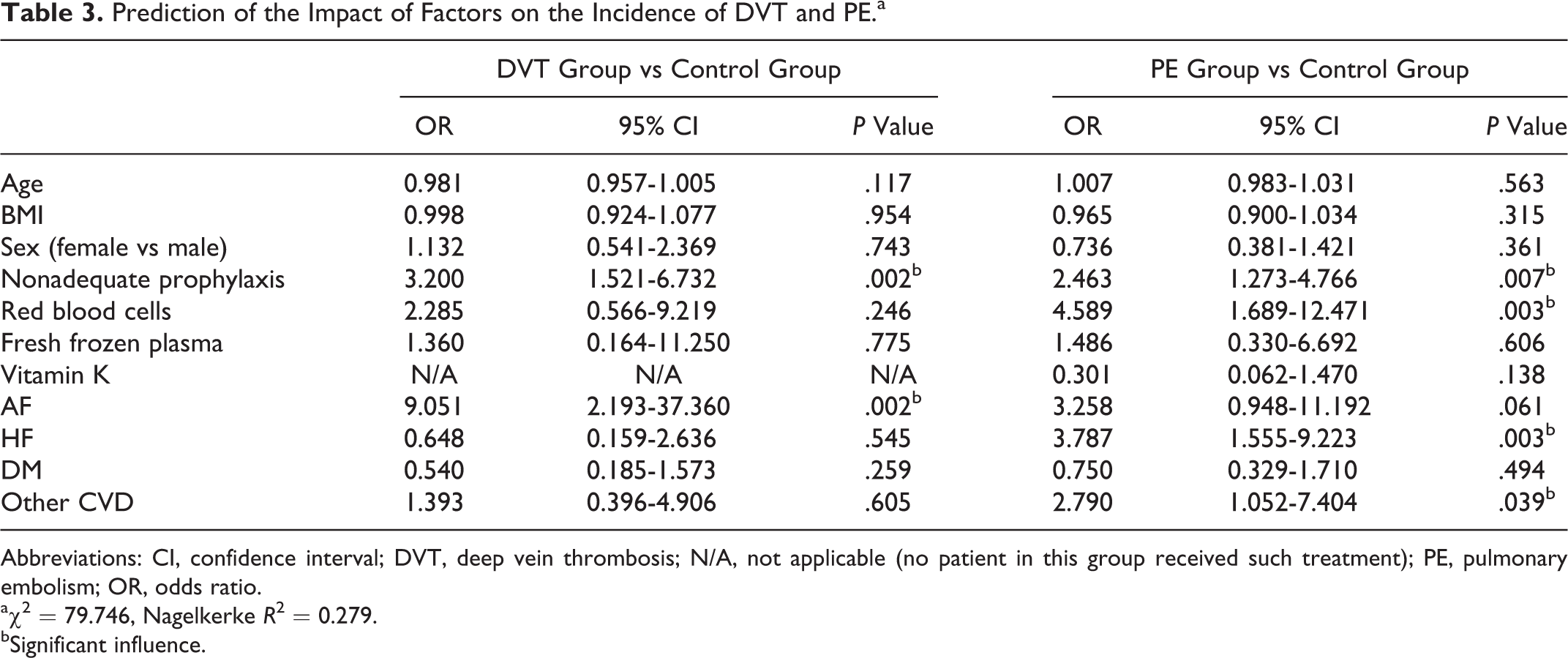
Abbreviations: CI, confidence interval; DVT, deep vein thrombosis; N/A, not applicable (no patient in this group received such treatment); PE, pulmonary embolism; OR, odds ratio.
aχ2 = 79.746, Nagelkerke R2 = 0.279.
bSignificant influence.
Discussion
The effect of prescribed concentrated red blood cells on development of postoperative PE in surgical patients was demonstrated in this study. Concentrated red blood cells are the most common blood product used to restore the oxygen-carrying capacity of the blood in patients with anemia. We speculate that by increasing blood viscosity and marginating platelets toward the endothelium, red blood cells may contribute to thrombotic complications, that is, PE. We did not demonstrate a similar connection in patients with DVT. However, in our analysis, red blood cells were given to only 5 (9.6%) of 52 patients who developed DVT, whereas red blood cells were given to 25 (27.2%) of 92 patients with PE.
The test groups also differed in hospitalization time: those who developed PE after surgery had longer hospitalization (median 10 days) than patients with DVT (median 6 days). Patients who are hospitalized for a shorter time are mobile earlier. In 26 patients who developed PE in the first 6 days after surgery, hospitalization was prolonged because of thrombotic complications. Thus, in patients who develop PE, it appears that longer hospitalization and receiving red blood cells are important risk factors that should be monitored closely.
Red blood cells affect blood viscosity and consequently blood flow. Moreover, red blood cells most probably affect the constituents of blood. Overall, it is clear that 2 of 3 important points in Virchow’s triad are affected.
Although components of plasma can increase the risk for the first episode of VTE, 19 we found no increased risk of thrombotic complications. There was no difference between the test and control groups in receiving FFP. The reason may be that the sample size was small, since FFP was given to only 12 (8.3%) patients in the test group and 5 (3.5%) in the control group.
Moreover, we did not find any association between treatment with vitamin K1 and increased risk of either DVT or PE in surgical patients. Vitamin K1 is necessary for the synthesis of the blood coagulation factors II (prothrombin), VII, IX, and X and the synthesis of inhibitors of coagulation proteins C and S in the posttranslational stage, thus affecting blood coagulation. The vitamin has an average half-life of 14 hours and therefore most probably does not have a long-term impact on the increased risk of postoperative thrombotic complications (either DVT or PE) if patients are protected with adequate prophylactic anticoagulant therapy.
The decision for or against a bridging therapy with appropriate doses of anticoagulants depends on assessment of the risk of thrombosis against the risk of bleeding. 28 In our study, 31 patients in the test group (6 patients with DVT, 25 patients with PE) and 33 patients in the control group received bridging therapy. Inadequate prophylaxis significantly increased the likelihood of both DVT (P = .002) and PE (P = .007). Appropriateness of prophylaxis has been reviewed at our hospital 27 using guidelines for the prevention of VTE. The appropriate selection of drugs, adequacy of dose and dosing interval, and appropriate duration of therapy were determined, based on the risk assessment score provided by the guidelines. In that analysis, 77% of patients in the control group received thromboprophylaxis according to the guidelines; in the test group, the proportion was only 56% (P < .05). 27 This finding of frequent inadequate thromboprophylaxis should increase awareness among hospital staff (predominantly doctors) of the need for appropriate thromboprophylaxis with low-molecular-weight heparins or other anticoagulants in surgical patients. Patients undergoing surgery should be stratified for risk of VTE according to patient risk factors, disease-related risk factors, and procedure-related risk factors. The type of prophylaxis should be commensurate with the risk of VTE based on the composite risk profile. The Caprini risk assessment model places patients in an ACCP risk, but packed red blood cells are not included among the risk factors. 14 According to our study, treatment with red blood cells is a significant factor that should be listed among risk factors for at least 1 point in the model.
Conclusions
An association between treatment with packed red blood cells and development of postoperative PE was identified in surgical patients. We believe that the key for appropriate thromboprophylaxis is good risk assessment of the patient followed by the appropriate treatment. From our findings, we suggest that surgical patients receiving red blood cells should be monitored more closely after surgery, because of their increased risk of postoperative PE.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.