
Abstract
Keywords
Introduction
Venous thromboembolism (VTE) is a common disorder associated with significant mortality and morbidity. Currently, after heart attack and stroke, VTE is the third most common vascular disorder.1,2 Two thirds of all VTE events are hospital acquired. 3 Much evidence exists about the efficacy, safety, and also cost-effectiveness of pharmacological and nonpharmacological measures to prevent VTE; nevertheless, appropriate thromboprophylaxis is still missing for a large number of hospitalized patients. Real-world reports suggest that less than 50% of the inpatients with diagnosed deep vein thrombosis (DVT) received adequate prophylaxis before DVT diagnosis. 4
Even though several studies have assessed pharmacological prophylaxis prescription among hospitalized patients, much less attention has been given to nonpharmacological prophylactic measures. In addition to the well-described complications of chemoprophylaxis such as bleeding and heparin-induced thrombocytopenia, there is limited reporting of other complications such as injection site pain and discomfort caused by bruises.5,6 Moreover, there is a paucity of evidence regarding thromboprophylaxis state in hospitalized patients in the Middle East, 7 including Iran. 8
Therefore, in this study we prospectively gathered data from inpatients of Masih-Daneshvari Medical Center, a teaching affiliate of Shahid Beheshti University MC, in Tehran, Iran; not only to determine the thromboprophylaxis rate but also to elucidate the thromboprophylaxis appropriateness and the adequacy of thromboprophylaxis based on the most recent recommendations of the American College of Chest Physicians (ACCP) on the prevention of VTE. 9
Methods
In this observational cross-sectional study, we prospectively evaluated the thromboprophylaxis state and all the associated parameters for hospitalized patients from Masih-Daneshvari hospital during the period from October 1, 2009 to December 30, 2009. Selected patients were from the internal medicine, cardiovascular, tuberculosis, and surgery departments. Exclusion criteria were admission less than 3 days, admission to the pediatrics department, primary hospitalization in the intensive care unit (ICU), and receiving therapeutic anticoagulation for primary cardiovascular or thromboembolic disease. All patients were visited in person by a nurse well trained about VTE and VTE prophylaxis (a VTE nurse). Data from the interviews and background data from the patients' charts were recorded in preformed data sheets. Two of the investigators (M.S. and A.S.) were in charge of checking the completed data sheets and data entry into the electronic databases. A separate investigator (B.B.) evaluated all the entered data to ensure the correctness and validity of the data before data analysis. Demographic information, primary admission diagnosis, as well as extensive data on VTE risk factors and comorbidities, baseline use of antithrombotics or antiplatelets, contraindications to thromboprophylaxis, and the use of nonpharmacological or pharmacological prophylaxis were recorded. Patients were asked whether they were advised to move out of bed after symptomatic recovery. Data regarding the local and systemic complications attributable to thromboprophylaxis were also obtained. A possible diagnosis of heparin-induced thrombocytopenia was defined as a platelet count of less than 150.000/fl after thromboprophylaxis reception, or a 50% reduction in the platelet count from baseline following thromboprophylaxis without any other apparent identifiable cause. A numeric scale ranging from 0 to 10 points was used to evaluate injection-site pain. In all patients, the presence of injection-site bruising before discharge or thromboprophylaxis discontinuation, whichever came first, was investigated. We used the eighth edition of the ACCP guidelines on VTE prophylaxis to check for the thromboprophylaxis appropriateness (including appropriate prophylaxis, underprophylaxis, and overprophylaxis).
9
We have previously described the methodology to assess thromboprophylaxis reception and prophylaxis appropriateness.
10
In summary, patients receiving VTE prophylaxis while having a low risk of VTE according to the ACCP guidelines were designated to be “overprophylaxed” whereas at-risk patients who did not receive any VTE prophylaxis were designated to be “underprophylaxed.” Conversely, the state of thromboprophylaxis was considered as “appropriate” in 2 series of patients: Cases who did not receive thromboprophylaxis and were not eligible for thromboprophylaxis according to the ACCP guidelines Cases who received thromboprophylaxis and had indications for thromboprophylaxis according to the ACCP guidelines
For the latter group, the type and dosing of the prescribed thromboprophylaxis were separately evaluated, as well (Figure 1
).
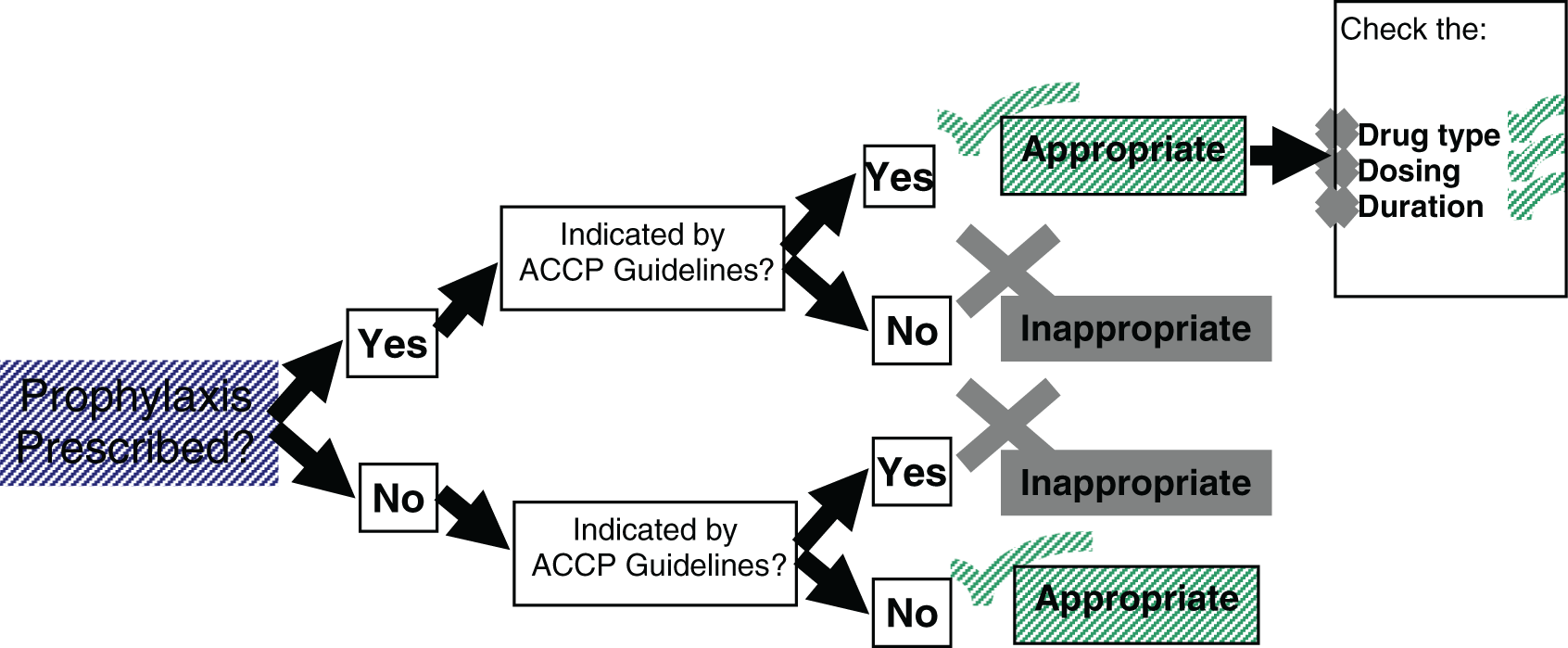
Model used for checking the thromboprophylaxis reception appropriateness.
Moreover, for those who needed to be prophylaxed, a ratio was defined to indicate ideal prophylaxis, dividing the prophylaxis reception length by the days the patients should have been prophylaxed according to the ACCP guidelines (see Table 1 ).
Background Findings and Comorbidities
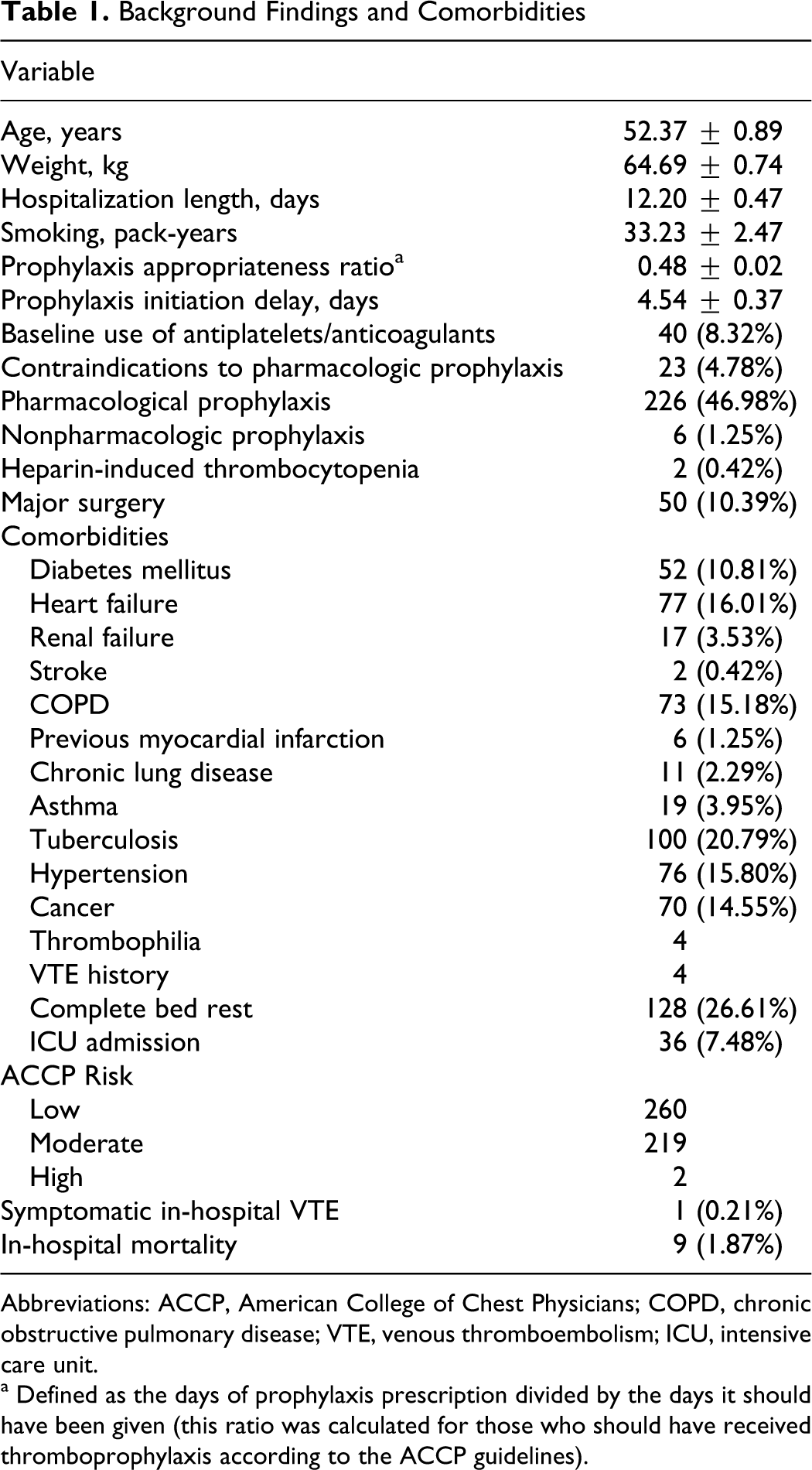
Abbreviations: ACCP, American College of Chest Physicians; COPD, chronic obstructive pulmonary disease; VTE, venous thromboembolism; ICU, intensive care unit.
a Defined as the days of prophylaxis prescription divided by the days it should have been given (this ratio was calculated for those who should have received thromboprophylaxis according to the ACCP guidelines).
All the patients' data remained confidential and were not shared with any third parties. The study protocol was approved by the National Research Institute of Tuberculosis and Lung Disease (NRITLD) ethics committee and NRITLD research council.
For statistical analysis, we used a statistical software package (STATA 8.0, StataCorp LP, College Station, Texas). Parametric data were reported as mean ± standard error of the mean. We used the chi-square test, with exact correction when necessary for categorical variables, and student’s t test for comparison of the means of quantitative parameters between 2 groups, whereas 1-way analysis of variances was used for a similar analysis between more than 2 groups. Similarly, for nonparametric data the Kruskal-Wallis test and the Mann-Whitney U test were used. Correlations between variables were checked by the Pearson’s and Spearman’s correlation coefficients. Multivariate logistic regression analysis was performed to find the independent predictors of prophylaxis prescription and thromboprophylaxis appropriateness. A P value of less than .05 was considered as significant. An attempted was made to prepare the manuscript according to the STROBE statement. 11
Results
A total of 904 cases were considered for this study, of whom 423 were excluded (126 received therapeutic anticoagulation from admission, 109 were primarily hospitalized in the ICU, 97 were pediatric patients, and 91 were hospitalized for less than 3 days) and finally 481 patients entered the study (mean age: 52.37 ± 0.89 years, 296 males and 185 females). Table 2 summarizes the initial diagnoses of the patients. Taken as a whole, 260 patients were at low VTE risk according to the ACCP guidelines, 219 patients had intermediate risk, and 2 patients were at high VTE risk. Twenty-three patients had contraindications to pharmacological prophylaxis (14 patients had severe renal or hepatic dysfunction, 4 had active gastrointestinal bleeding, 3 had severe anemia with hematocrit less than 30%, and 2 had massive hemoptysis). No patient had apparent contraindications to nonpharmacological prophylaxis. Background findings and comorbid conditions could be found in Table 1.
Initial Diagnosis of Hospitalized Patients
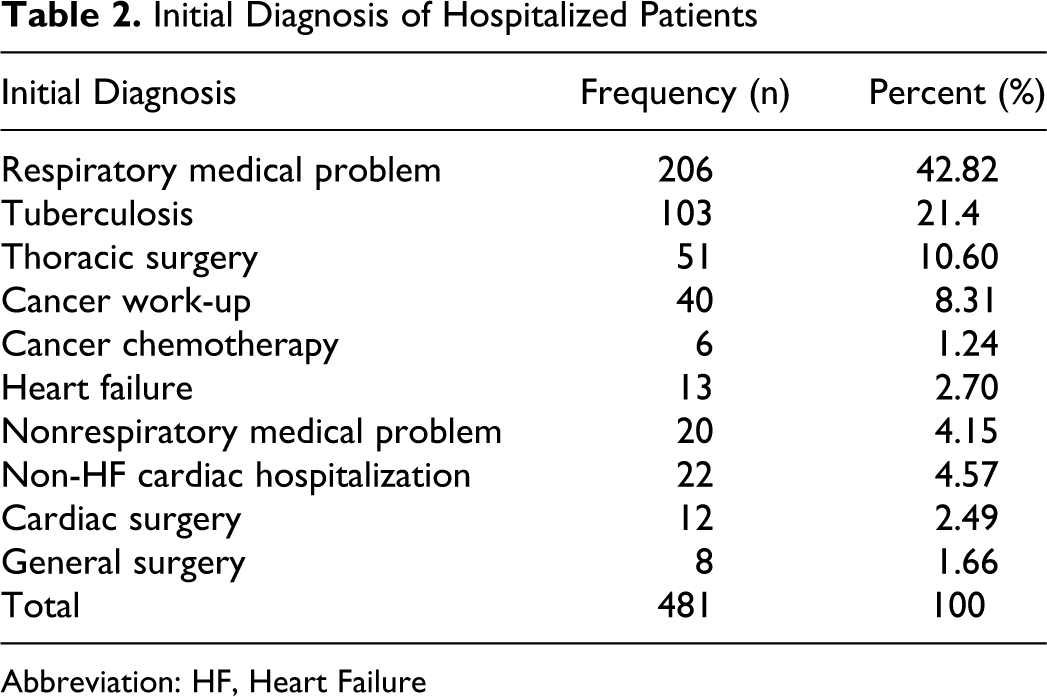
Abbreviation: HF, Heart Failure
Overall, prophylaxis was prescribed for 232 patients (48.23%); 157 (67.56%) received unfractionated heparin (UFH), 69 (29.74%) received enoxaparin sodium, and for 6 (2.58%) nonpharmacological prophylaxis was used. Of those, 94 patients were overprophylaxed, while 139 of those who received VTE prophylaxis were designated as “at risk” based on the ACCP guidelines. In the latter group, 57 patients received their thromboprophylaxis with delay, 2 patients received the improper prophylaxis type, and 17 patients received incorrect dosing of thromboprophylaxis. Therefore, only 63 (28.50%) patients from the total of 221 (219 + 2) patients who should have received thromboprophylaxis had received their thromboprophylaxis regimen properly. Of the 249 patients who did not receive any prophylaxis, 82 were underprophylaxed (Figure 2 ).
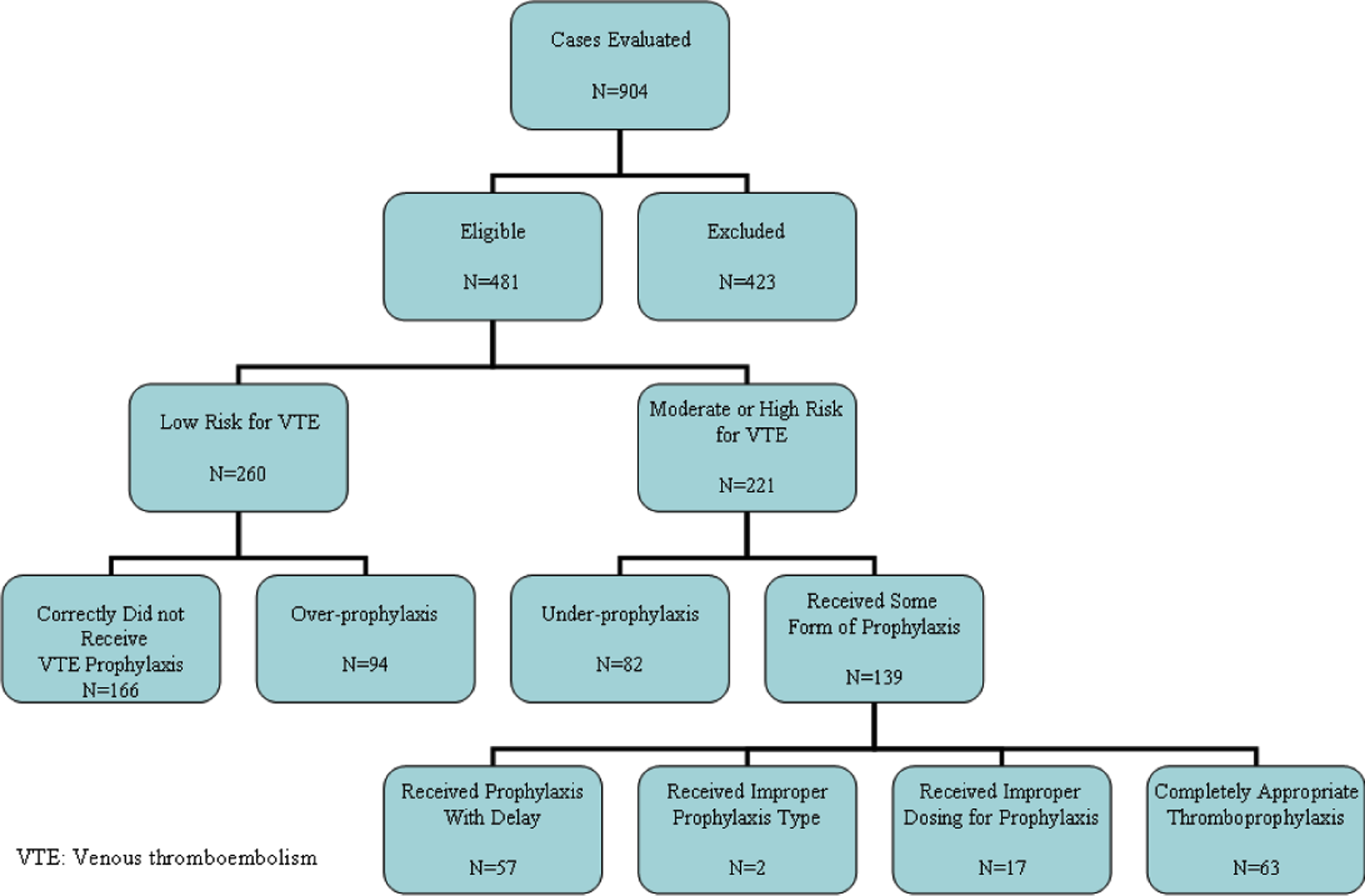
Use the thromboprophylaxis in patients' subgroup.
Therefore, from the total of 481 included patients, for 305 (63.40%) correct decision was made on whether to prophylaxe or not. However, complete thromboprophylaxis appropriateness (also entailing the correct regimen type, dosing, and duration) was only evident for 229 cases (47.60%). Symptomatic VTE happened for only 1 patient who had received prophylactic heparin, albeit with delay. There were no major bleeding events due to pharmacological prophylaxis.
Patients with history of diabetes mellitus, bed rest, heart failure, chronic obstructive pulmonary disease (COPD), and ICU admission in the course of hospitalization more frequently received thromboprophylaxis (P < .001 for each). However, no significant difference was found in the relative frequency of renal failure, major surgery, or cancer in those who received thromboprophylaxis compared to those who did not (P = .69, P = .96, and P = .27, respectively). Interestingly, presence of contraindications to pharmacological prophylaxis was not associated with lower rate of prophylaxis prescription (P = .37). Moreover, patients with moderate-to-high ACCP risk due to surgery, less commonly received any type of prophylaxis, compared to those with moderate-to-high ACCP risk due to nonsurgical reasons (P = .03).
Forty-seven patients with complete bed rest order had not received thromboprophylaxis. Of those, 2 were young patients with hemoptysis who were at low risk for VTE and 4 patients had contraindications to pharmacoprophylaxis and did not receive nonpharmacological prophylaxis. The remainder of cases was likewise underprophylaxed.
There was no significant difference in the frequency of injection site bruising in those receiving UFH compared to those receiving low-molecular-weight heparin (LMWH; 87.16% vs 78.46%; P = .106). Injection-site pain was not significantly different between the 2 groups, either (3.59 ± 0.17 vs 4.09 ± 0.27; P = .12). Duration of prophylaxis was associated with injection-site pain (Pearson rho: .193, P = .005) and injection-site bruising (Spearman rho: .232, P < .001). Two patients had a possible diagnosis of heparin-induced thrombocytopenia, both of whom had received prophylactic UFH.
By multivariate logistic regression, ACCP risk for VTE was the strongest predictor of prophylaxis prescription (odds ratio [OR]: 2.62, 95% confidence interval [CI]: 1.35-5.05, P = .004). Interestingly, however, presence of COPD was also an independent predictor of prophylaxis prescription, even after adjustment for the ACCP risk (OR: 2.47, 95% CI: 1.23-4.98; P = .011). Admission in the surgical department was an inverse independent predictor of prophylaxis prescription (OR: 0.34, 95% CI: 0.11-1.01; P = .05).
Multivariate logistic regression analysis also demonstrated that presence of heart failure was an independent predictor of better prophylaxis appropriateness (OR: 2.60, 95% CI: 1.30-5.20; P = .007). The ACCP risk for VTE was an inverse predictor of prophylaxis appropriateness (OR: 0.46, 95% CI: 0.25-0.85; P = .013), that is patients at low risk for VTE had better appropriateness ratios. In other words, underprophylaxis was more prominent than overprophylaxis, overall.
Discussion
Studies evaluating the thromboprophylaxis state and prophylaxis appropriateness in Middle Eastern countries are not plentiful. The few existing reports suggest that the situation in such countries is suboptimal,7,8,12 and in some aspects worse than that of Europe and North America.8,12 In our study, correct decision on whether to prophylaxe or not for VTE was made in 305 (63.40%) patients. Complete thromboprophylaxis appropriateness was seen only in 229 cases (47.60%). These figures should be comparable, and at some instances superior to thromboprophylaxis data from hospitals in Western countries.13,14 The Masih-Daneshvari hospital is located at the NRITLD, a World-Health-Organization-collaborating university-based tertiary care center for tuberculosis, lung disease, and associated cardiac conditions, which has acted as a pioneer in several programs pertaining to management and prophylaxis of VTE in the region. No active intervention was performed to enhance VTE prophylaxis state or thromboprophylaxis appropriateness during the study period, however, several programs, including the use of sticker reminders to improve prophylaxis appropriateness 10 (which had resulted in an overall appropriateness rate of above 78%) had been conducted at NRITLD before the current study was started. Accordingly, relatively desirable knowledge and awareness of NRITLD health care staff regarding VTE prophylaxis is in general dissimilar to that expected at other medical centers of a developing country like Iran where at some other hospitals thromboprophylaxis appropriateness rates of less than 1% have been reported.8,15 Heart failure patients in our study had a better overall prophylaxis appropriateness. We believe this finding to be caused by significant contribution of the team responsible for management of heart failure patients in many separate VTE prophylaxis studies and clinical initiatives.
Interestingly, barriers to proper thromboprophylaxis in different departments in our study were not identical. While some studies suggest that surgical at-risk patient receive prophylaxis more frequently and more appropriately,16,17 in our study patients hospitalized in the surgical department were more frequently underprophylaxed compared to patients in the medical departments (24 of 90 vs 58 of 391; P = .028). In contrast, overprophylaxis was more commonly seen in those hospitalized at medical departments (90 of 391 vs 4 of 90; P = .001). This was mainly owing to overprophylaxis in many medical patients with a history of COPD. Chronic obstructive pulmonary disease is known to be associated with increased risk of VTE and disease severity in those with VTE, and therefore, appropriate thromboprophylaxis is warranted for at-risk COPD patients.9,18,19 However, many COPD patients in our study were hospitalized in order to fully learn how to adjust themselves to the medications, under close observation. These patients (in contrast to COPD, or asthma patients for whom prophylaxis was necessary) did not present with severe respiratory distress, were ambulatory, and their hospitalization length was likewise short.
Our study did not show a significant difference in local complications between UFH and LMWH. Both UFH and LMWH have comparable efficacy for thromboprophylaxis and the choice between them should be based on clinical condition of the patient, renal function, economical factors, and physicians' preferences. 9
Nonpharmacological means of thromboprophylaxis (ie, graded compression stockings or intermittent pneumatic compression) were only used in 6 (1.24%) patients. Given the proven usefulness of nonpharmacological thromboprophylaxis for those with contraindications to pharmacological options, 9 educational and monitoring strategies should be developed for more widespread applications of nonpharmacological prophylaxis. Moreover, even though evidence exists about the usefulness of early ambulation for hospitalized patients,9,20,21 only 2 patients (0.4%) in our study had received such recommendations. In a similar study by Rahim et al, only 4% of patients had received early ambulation orders. 22 Therefore, we believe that physicians should be urged to discuss the benefits of early ambulation with hospitalized patients more responsively.
We must also acknowledge the limitations of our study: The number of VTE events in our study is possibly underestimated, since routine screening is not performed for DVT or pulmonary embolism (PE) at our center. Therefore, it is possible that some cases of asymptomatic DVT, and some cases of PE in whom competing comorbidities were masking the clinical manifestations, were missed. Our data represent the thromboprophylaxis state in an academic teaching hospital. In order to better represent such data from Iran, multicentric studies which also incorporate patients from community hospitals, particularly from less developed districts would be necessary.
Our findings suggest similar thromboprophylaxis state and prophylaxis appropriateness compared to the Western countries. Nevertheless, our reported thromboprophylaxis appropriateness is far from optimal. Barriers to appropriate thromboprophylaxis are diverse and include underestimation of VTE risk and overestimation of bleeding risk, guidelines discrepancy, and lack of institutional internal prophylaxis protocols. 23 Ways to improve barriers to appropriate thromboprophylaxis include updating knowledge of responsible physicians by continuous medical education programs and auditing systems, as well as applying reminder systems similar to the sticker reminder system we had used for a short time at NRITLD 10 or ideally, electronic alert systems that notify the responsible physicians about the VTE risks and available prophylaxis options for each of the hospitalized patients, as well as development of local VTE prophylaxis protocols at hospitals. 24 What is more, implementation of a comprehensive approach that also encompasses public awareness programs and policy-making support, in addition to targeting the practicing physicians could ultimately translate into reduction in VTE events and better patient care. 25
Conclusion
Our study demonstrated similar thromboprophylaxis and prophylaxis appropriateness ratios compared to the Western studies. Since the thromboprophylaxis pitfalls occur differently based on physicians' specialty, distinct educational or reminder programs could be more useful rather than “one-size-fits-all” solutions. Using a multistep program encompassing public awareness raising, medical education at medical schools, continuous education for practicing physicians, providing targeted educational material and reminder programs about VTE prophylaxis, as well as proper policy making could ideally remove many of the barriers to appropriate thromboprophylaxis and lead into marked reduction in VTE events.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This Work was supported by a research grant from the National Research Institute of Tuberculosis and Lung Disease.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.