
Abstract
Warfarin is a recommended therapy to reduce the risk of stroke in patients with nonvalvular atrial fibrillation (NVAF). The objectives of this study were to identify potential factors associated with warfarin persistence and evaluate the impact of warfarin persistence on health-care resource utilization and costs among patients with NVAF in the United States. Patients (≥18 years) with ≥1 inpatient or ≥2 outpatient diagnoses of AF without valvular disease were identified from an electronic medical record database (January 1, 2004, to January 31, 2015). The patients with NVAF were grouped into 2 cohorts—persistent with warfarin therapy and not persistent (warfarin discontinuation in <365 days). A multivariable regression was used to identify potential predictors of warfarin persistence. Health-care costs were evaluated during a 12-month follow-up period for study cohorts. Among the study population, 52%, (n = 4086) were persistent with warfarin therapy and 48% (n = 3722) were not. Patients with NVAF with higher Charlson comorbidity index and CHADS2 scores versus those with scores of 0 were more likely to demonstrate persistence with warfarin therapy. After adjusting for patient characteristics, patients with NVAF persistent with warfarin therapy versus those who were not were 30% less likely to be hospitalized during the follow-up period (P < .001). Additionally, total all-cause health-care costs (US $2183, P < .001) and stroke-related costs (US $788, P < .001) were significantly lower among patients persistent with warfarin therapy versus those who were not. Patients with NVAF who have greater comorbidity and stroke risk are more likely to be persistent with warfarin therapy. Patients with NVAF who are persistent with warfarin therapy versus those who are not have lower all-cause and stroke-related health-care costs.
Introduction
Atrial fibrillation (AF) is a common cardiac rhythm disorder estimated to affect 5.2 million individuals in the United States in 2010, which is projected to increase to 12.1 million by 2030. 1 It is predominately not caused by a heart valve problem and is known as nonvalvular atrial fibrillation (NVAF). 2 It becomes increasingly more prevalent as people age and is associated with up to a 5-fold higher stroke risk. 2,3 Taking into consideration the growing elderly population in the United States, the number of persons with NVAF is estimated to double or possibly triple by 2050. 2,3 Consequently, the economic burden of NVAF, to which hospitalizations significantly contribute, is also predicted to increase from an estimated US$13.9 billion annually in 2010 to nearly US$30 billion annually by 2050. 4
Warfarin has been shown to be efficacious for reducing the risk of stroke among patients with NVAF, with a meta-analysis of several clinical trials reporting a 64% decrease in the risk of stroke among patients with AF treated with adjusted-dose warfarin versus control or antiplatelet agents. 5 However, a substantial percentage of patients with NVAF, ranging from 25% to 65%, exhibit poor persistence with warfarin therapy, which has been attributed to several factors, including patient age, bleeding risk, suboptimal anticoagulation control, recent hospitalization, and lower risk of stroke. 6 –12
The American College of Chest Physicians guidelines recommend that “health care providers who manage oral anticoagulation therapy should do so in a systematic and coordinated fashion, incorporating patient education, systematic International Normalized Ratio (INR) testing, tracking, follow-up, and good patient communication of results and dosing decisions.” 13(p.e153S) Studies of pharmacist-managed anticoagulation services have demonstrated that patients who receive care at these types of programs have less anticoagulation-related adverse events and less hospitalizations and emergency department (ED) visits as compared to patients who receive usual care. 14 –17 As a result, health-care costs are lower for these patients. 14 –17 In this study, we evaluated in a large anticoagulation program managed by anticoagulation clinics in an integrated delivery network (IDN) setting the potential factors associated with warfarin persistence and the impact of warfarin persistence status on health-care resource utilization and costs among patients with NVAF.
Methods
Adult patients (aged ≥18 years) with a primary or secondary diagnosis of AF (International Classification of Diseases, 9th Revision, Clinical Modification [ICD-9-CM] code 427.31) on ≥1 inpatient encounter or on ≥2 outpatient encounters on 2 separate dates or ≥6 encounters with an anticoagulation clinic on separate dates were identified from an electronic medical record (EMR) database between January 1, 2004, and January 31, 2015. The data source is de-identified and compliant with the Health Insurance Portability and Accountability Act. The first prescription record for warfarin after the initial AF diagnosis was defined as the index event, with the corresponding date as the index date. The baseline and follow-up periods were the 12 months before and after (and including) the index date, respectively. Patients were excluded if they had any primary or secondary diagnosis code or procedure code for valvular disease and if they had any primary or secondary diagnosis code or procedure code for pregnancy, labor, or delivery during the study periods. Patients were also excluded if they received any of the direct-acting oral anticoagulants (DOACs), including dabigatran, rivaroxaban, apixaban, and edoxaban.
Warfarin time to discontinuation (TTD) was defined similar to Go et al 17 as the number of days from the index date to the end of continuous warfarin therapy. Continuous warfarin therapy was defined as having 2 warfarin prescriptions with a gap of <60 days. If the gap between warfarin prescriptions was >60 days, but an INR laboratory test occurred at least every 60 days, then the patient was still considered as having continuous warfarin therapy. In the event that INR measurements were greater than 60 days apart, the patient was considered to be not taking warfarin from day 31 after the end date of the first prescription until the start date of the next prescription. This grace period of 30 days at the end of each warfarin usage period was used since changes in dosages are common. The end of continuous warfarin treatment period was defined as the end of the above described continuous treatment period. Patients with continuous warfarin treatment up to the end of their follow-up periods were considered to have their treatment period censored by the end of the follow-up period. Descriptive statistics were used to measure warfarin TTD of all patients with NVAF. The median TTD was determined to be 383 days, and close to 365 days, which was defined as the TTD threshold. Patients with NVAF were grouped into 2 study cohorts—(1) persistent with warfarin therapy cohort comprised of patients with a warfarin TTD longer than 365 days and (2) nonpersistent with warfarin therapy cohort comprised of patients with a warfarin TTD less than 365 days.
Demographics and Clinical Characteristics
Patient profiles were evaluated for the study cohorts and consisted of demographics and clinical characteristics, including age, gender, race, Charlson comorbidity index (CCI), CHADS2 and CHADS2-VASc scores, and major comorbid conditions.
Predictors of Warfarin Persistence Status
A multivariable logistic regression was carried out to identify potential patient factors associated with warfarin persistence status. Covariates in the regression included age, gender, race, CCI score group, and CHADS2 score group.
Health-Care Resource Utilization and Costs
Health-care resource utilization and costs during the 12-month follow-up period were evaluated for the study cohorts. Health-care resources included all health-care encounters—inpatient admissions, including length of hospital stay and intensive care unit (ICU) stay; office visits; and ED visits. Health-care resource utilization was further stratified by encounters for all causes and by cardiovascular (CV)-, stroke-, and bleeding-related encounters. The CV-, stroke-, and bleeding-related health-care utilization was identified by the corresponding ICD-9-CM codes on either inpatient or outpatient health-care encounters for a primary or secondary diagnosis of the particular condition. Total health-care costs were measured for all evaluated health-care resource utilizations. All costs were inflation adjusted to 2015 cost levels using the Consumer Price Index: Medical Care. 18
Statistical Analyses
Descriptive statistics were used to evaluate differences between the study cohorts in demographics, clinical characteristics, and unadjusted health-care resource utilization and costs. T tests and χ2 tests were used to detect statistically significant differences in continuous and categorical variables, respectively. A multivariable logistic regression was carried out to evaluate the impact of warfarin persistence status on the odds of hospitalization during the follow-up period. Covariates included age, gender, race, CCI score group, and CHADS2 score group. Multivariable generalized linear models (GLMs) were used to control for differences in patient characteristics and to examine the impact of warfarin persistence status on health-care costs for all causes and for stroke- and bleeding-related costs. Covariates included in the GLMs were age, gender, race, CCI score group, CHADS2 score group, and baseline total health-care cost. The GLMs used a γ distribution and log transformation for the cost variable. A critical value of .05 was used to determine statistical significance. All statistical analyses were performed using SAS version 9.3.
Results
Demographics and Clinical Characteristics
Demographics and clinical characteristics of the study cohorts are presented in Table 1. Among the study population, 52%, (n = 4086) were persistent with warfarin therapy and 48% (n = 3722) were not. Mean ages of the persistent and nonpersistent cohorts were 71.8 and 71.0 years, respectively. The majority (99%) of both study cohorts were white. Overall comorbidity, as measured by mean CCI score (2.1 vs 1.8, P < .001), and stroke risk, as measured by mean CHADS2 score (1.9 vs 1.6, P < .001) and CHADS2-VASc score (3.4 vs 3.0, P < .001), were greater for patients with NVAF persistent with warfarin therapy versus those who were not. Hypertension, diabetes, and congestive heart failure were significantly more common among patients with NVAF persistent with warfarin therapy versus those who were not.
Demographics and Clinical Characteristics of Study Cohorts.
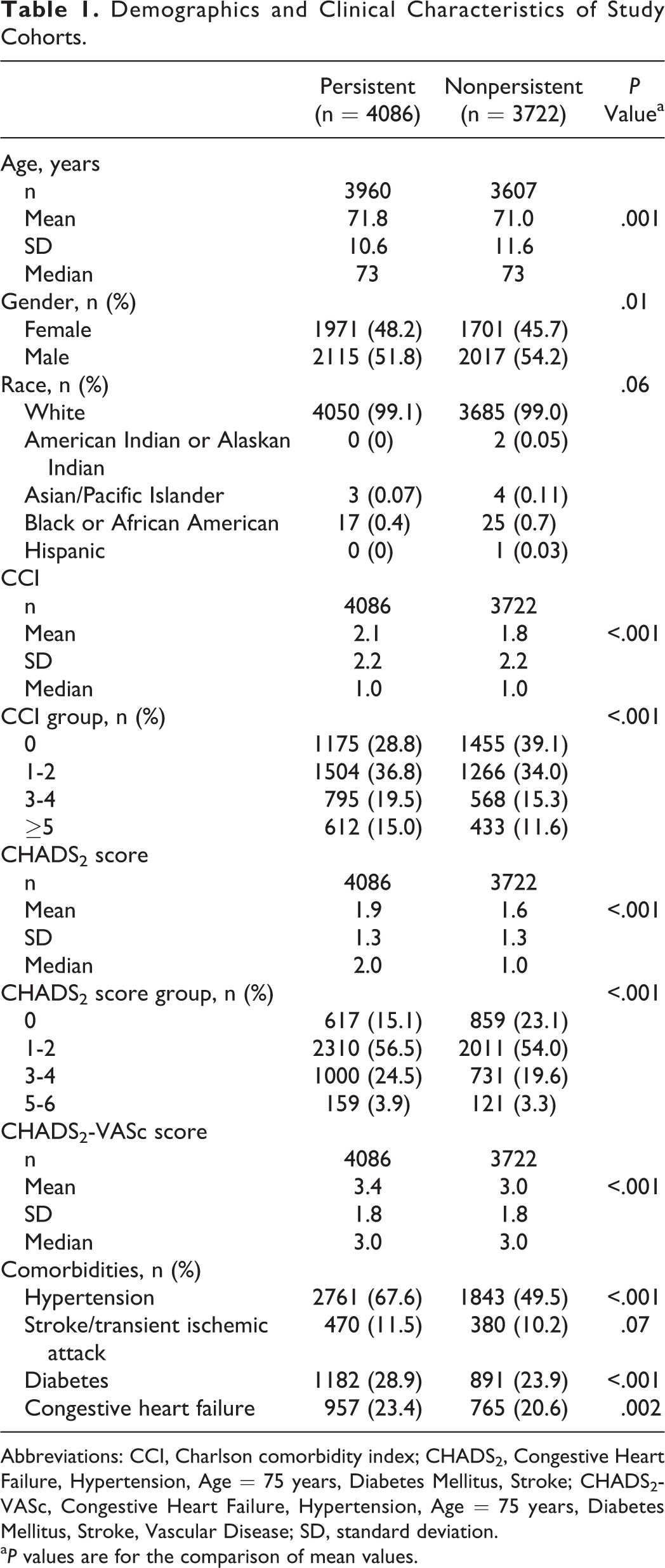
Abbreviations: CCI, Charlson comorbidity index; CHADS2, Congestive Heart Failure, Hypertension, Age = 75 years, Diabetes Mellitus, Stroke; CHADS2-VASc, Congestive Heart Failure, Hypertension, Age = 75 years, Diabetes Mellitus, Stroke, Vascular Disease; SD, standard deviation.
a P values are for the comparison of mean values.
Predictors of Warfarin Persistence Status
Patients with NVAF with higher CCI scores (odds ratio [OR] for CCI = 1-2 vs CCI = 0: 1.34, P < .001; CCI = 3-4 vs CCI = 0: 1.51, P < .001; CCI ≥5 vs CCI = 0: 1.55, P < .001) and CHADS2 scores of 1 to 4 (OR for CHADS2 = 1-2 vs CHADS2 = 0: 1.38, P < .001; CHADS2 = 3-4 vs CHADS2 = 0: 1.39, P < .001) versus those with scores of 0 were more likely to be persistent with warfarin therapy (Table 2).
Multivariable Regression: Predictors of Persistent Versus Not Persistent With Warfarin Therapy Among Patients With NVAF.
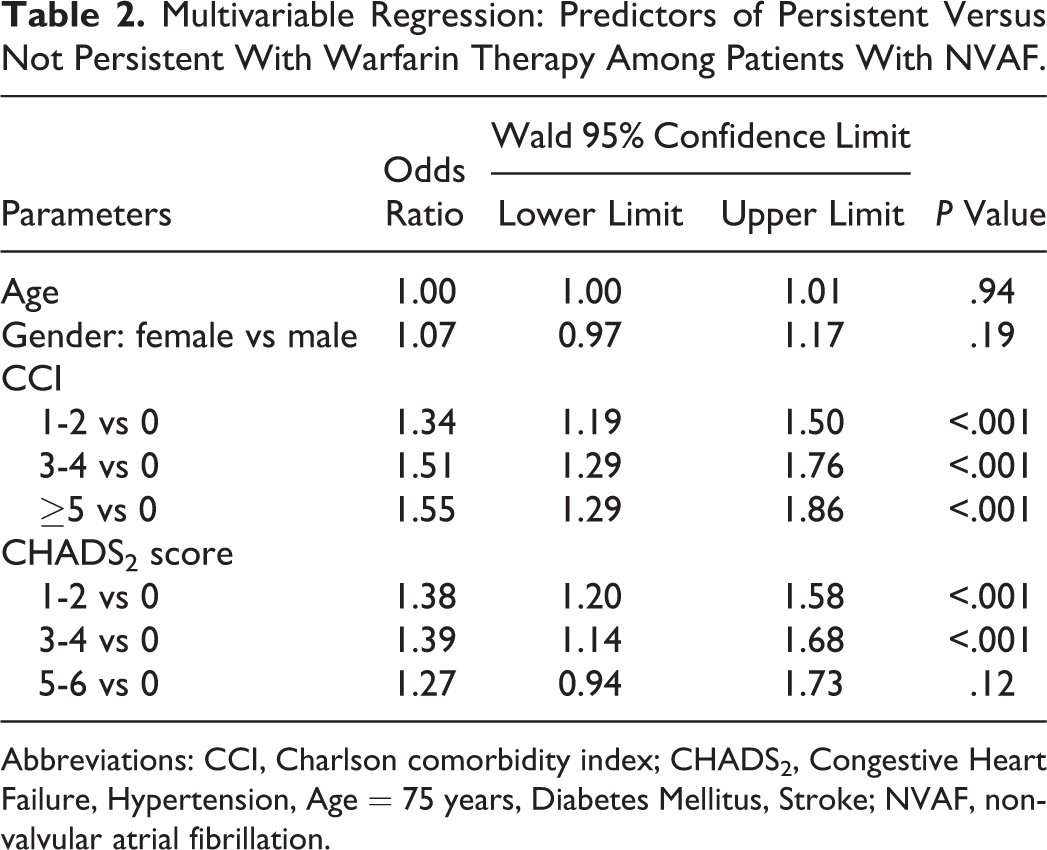
Abbreviations: CCI, Charlson comorbidity index; CHADS2, Congestive Heart Failure, Hypertension, Age = 75 years, Diabetes Mellitus, Stroke; NVAF, nonvalvular atrial fibrillation.
Health-Care Resource Utilization and Costs
Unadjusted health-care resource utilization and associated costs for the 2 study cohorts during the 12-month follow-up period are shown in Table 3. Total health-care resource utilization for all causes was greater among patients with NVAF persistent with warfarin therapy versus those who were not (mean: 58.9 vs 28.3 health-care encounters, P < .001), as well as were CV-related (42.6 vs 16.8 encounters, P < .001) and stroke-related (0.89 vs. 0.51 encounters, P < .001) health-care resource utilization. However, in comparison to patients with NVAF not persistent with warfarin therapy, the mean number of inpatient admissions for all causes (0.48 vs 0.64, P < .001), mean hospital length of stay (2.49 vs 3.84 days, P < .001), and mean ICU length of stay (0.12 vs 0.28 days, P < .001) were significantly less for patients persistent with warfarin therapy during the follow-up period. For both study cohorts, the majority of inpatient admissions during the follow-up period were CV related, which were similarly lower in number (0.48 vs 0.62 encounters, P < .001) and associated with significantly less lengths of stay in the hospital (2.44 vs 3.71 days, P < .001) and in the ICU (0.12 vs 0.27 days, P < .001) for patients with NVAF persistent with warfarin therapy versus those who were not. The mean number of stroke-related inpatient admissions (0.08 vs 0.10, P = .01), hospital length of stay (0.50 vs 0.73 days, P = .003), and ICU length of stay (0.02 vs 0.09 days, P < .001) as well as bleeding-related inpatient admissions (0.09 vs 0.11, P = .005), hospital length of stay (0.56 vs 0.79 days, P = .004), and ICU length of stay (0.04 vs. 0.11 days, P = .002) were significantly less for patients with NVAF persistent with warfarin therapy versus those who were not during the follow-up period.
Unadjusted Health-Care Resource Utilization and Associated Costs Per Patient During the 12-Month Follow-Up Period.
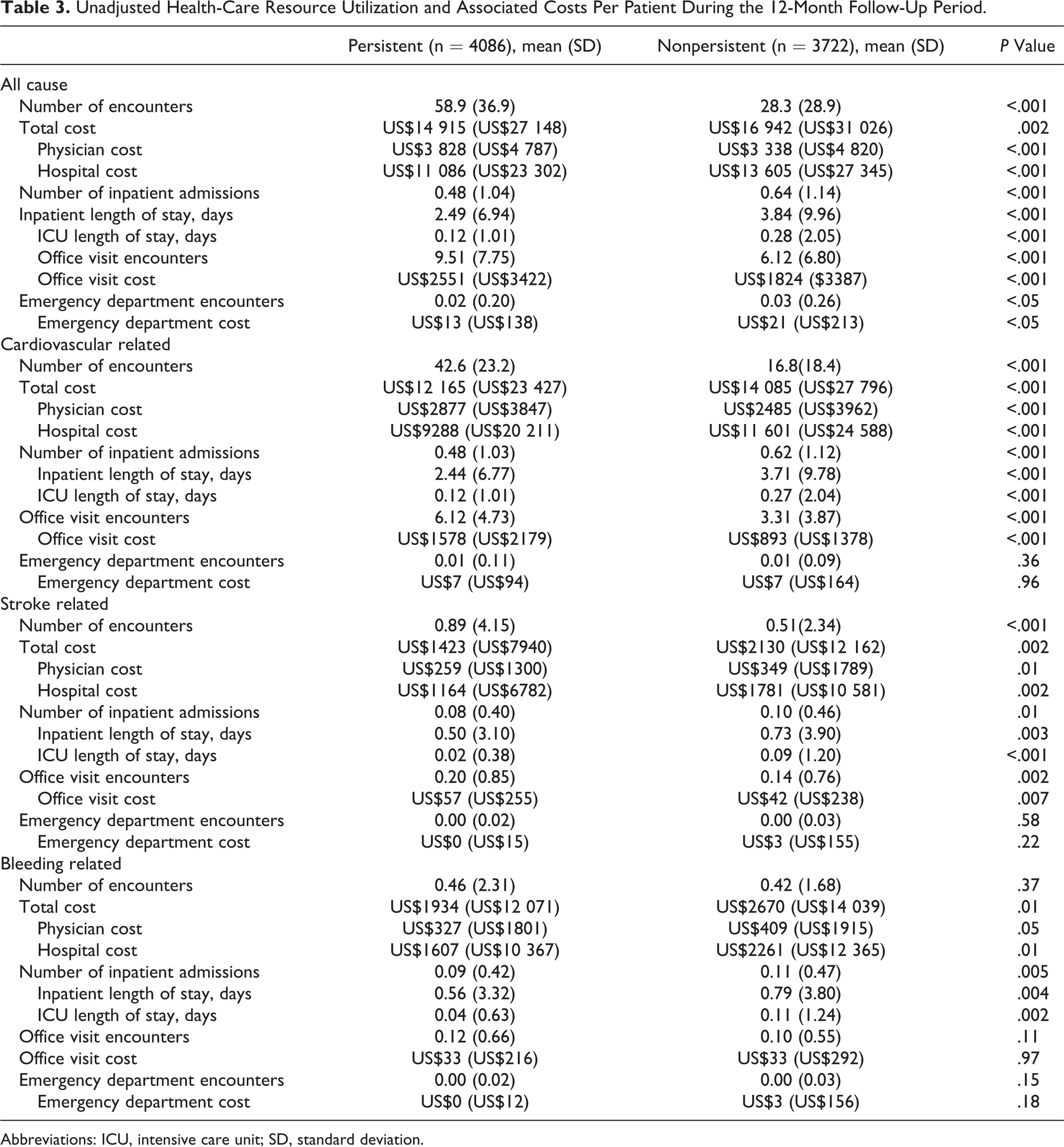
Abbreviations: ICU, intensive care unit; SD, standard deviation.
The lesser use of inpatient health-care resources among patients with NVAF persistent with warfarin therapy versus those who were not was reflected in lower mean total health-care costs and hospital costs per patient for all causes (US$14 915 vs US$16 942, P = .002; US$11 086 vs US$13 605, P < .001, respectively), CV related (US$12 165 vs US$14 085, P < .001; US$9 288 vs US$11 601, P < .001, respectively), stroke related (US$1423 vs US$2130, P = .002; US$1164 vs US$1781, respectively), and bleeding related (US$1934 vs US$2670, P = .01; US$1607 vs US$2261, P = .01, respectively). Mean physician (US$3828 vs US$3338, P < .001) and office visit costs (US$2551 vs US$1824, P < .001) for all causes and those which were CV related (physician: US$2877 vs US$2485, P < .001; office: US$1578 vs US$893, P < .001) were greater for patients with NVAF persistent with warfarin therapy in comparison to those who were not. Stroke-related physician costs were also lower. Office visit costs were higher for patients persistent with warfarin therapy in comparison to those who were not. Bleeding-related physician costs also tended to be lower among patients persistent with warfarin, whereas bleeding-related office visit costs were similar for both cohorts.
Hospitalization During the Follow-Up Period
After adjusting for age, gender, race, CCI score group, and CHADS2 score group, patients with NVAF persistent with warfarin therapy, relative to those who were not, had lesser odds of hospitalization during the 12-month follow-up period (OR: 0.69, P < .001; Figure 1).
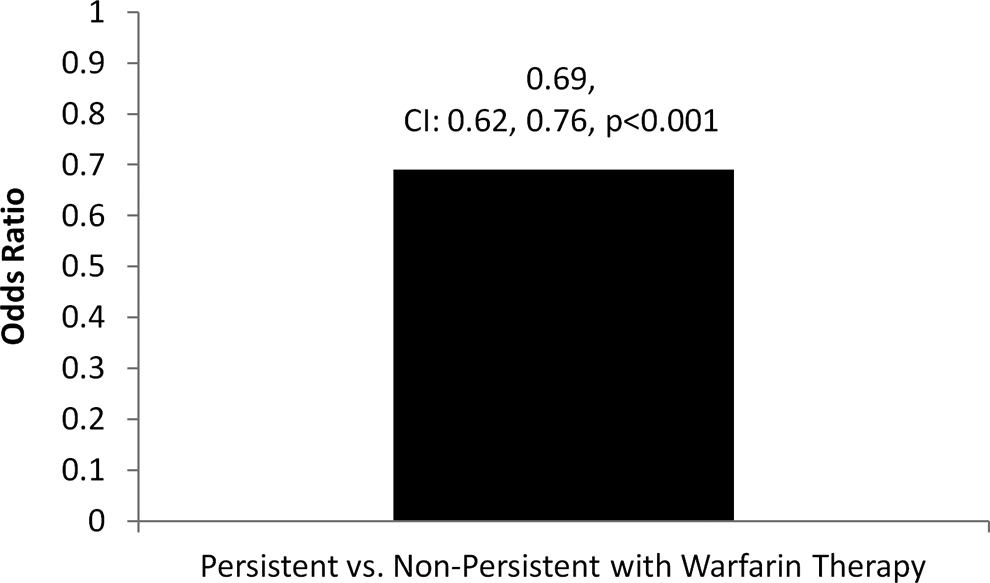
Likelihood of hospitalization during the follow-up period.
Adjusted Health-Care Costs
A summary of the multivariable regression analyses examining the impact of warfarin persistence status on health-care costs is presented in Table 3 (Figure 2). After adjusting for patient characteristics, total health-care costs for all causes and stroke-related health-care costs were US$2183 (P < .001) and US$788 (P < .001) lower per patient, respectively, among patients persistent with warfarin therapy versus those who were not. After adjusting for patient characteristics, bleeding-related health-care costs tended to be lower for patients persistent with warfarin therapy versus those who were not (US $544, P = .07).
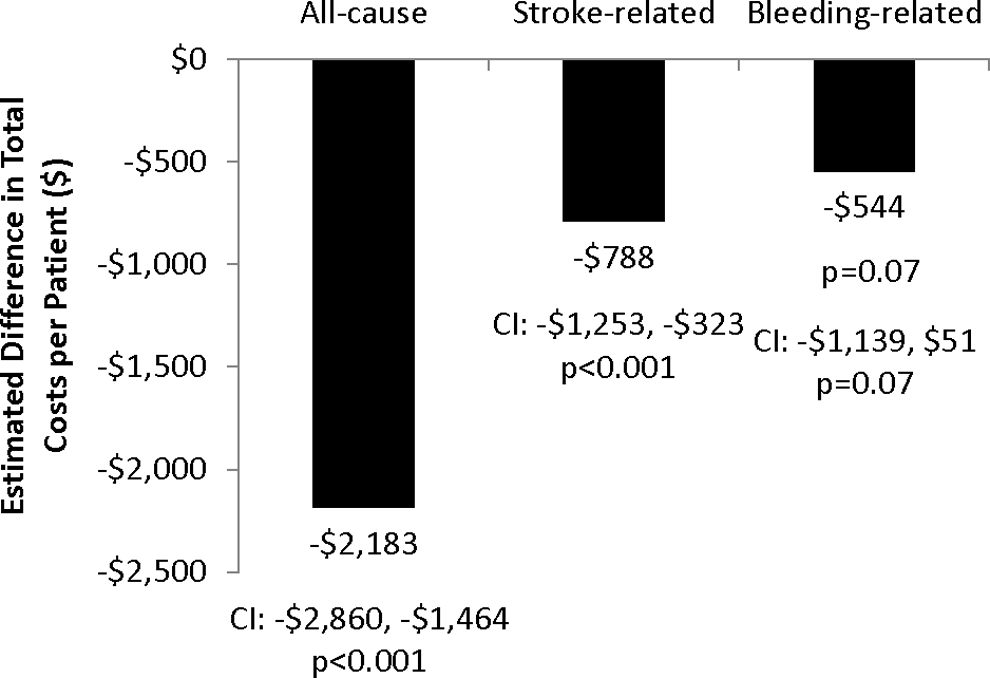
Summary of multivariable regression results: estimated differences in total costs per patient among patients with nonvalvular atrial fibrillation (NVAF) persistent with warfarin therapy versus not persistent.
Discussion
In this study of 7808 patients with NVAF with warfarin therapy managed by an anticoagulation program, 52% were persistent with warfarin therapy and 48% discontinued treatment within 1 year. These results are similar to that of an earlier database study of patients with NVAF between January 1, 2005, and June 30, 2009, which reported that 51.4% of 16 253 of patients with NVAF discontinued warfarin therapy (with a gap over 60 days between warfarin prescriptions) at least once during the follow-up period. 19 The proportion of patients with NVAF who discontinued warfarin therapy in our study is below that observed by Spivey et al, in which 55.2% of patients with NVAF insured commercially or through Medicare discontinued warfarin within the first year of therapy. 6 Despite some variation in results and methodology across these more recent studies evaluating persistence with warfarin therapy, the frequency of discontinuation in patients with NVAF approximates 50%. 6,20 Thus, even when patients with NVAF receive high-quality care from pharmacist-managed anticoagulation clinics, as in our study, there remains a substantial portion of patients with NVAF who discontinue warfarin therapy. It is likely that the patient population in this study included those chronically treated for AF with anticoagulation therapy, as patient data were extracted from EMRs obtained from anticoagulation clinics within the IDN, and these clinics primarily manage patients with AF receiving chronic therapy.
Multiple studies have found that interruption of warfarin therapy is associated with an increased risk of adverse events among patients with NVAF. 19 –21 Deitelzweig et al, in the study in which 51.4% of patients with NVAF discontinued warfarin therapy, reported that stroke risk increased 1.6-fold during periods of warfarin discontinuation. 19 Spivey et al reported a 2-fold increased risk of ischemic stroke for patients who discontinued warfarin therapy in comparison to those who were persistent with therapy. 20 Raunso et al conducted a nationwide study in Denmark of 48 989 patients with AF and reported the incidence rate of the combined end point of thromboembolism or death increased up to 2.5-fold in the first 90 days of warfarin treatment interruption. 21 Based on these studies, it is of great concern that so many patients with NVAF potentially remain at higher risk for adverse events, including death, and it is important to identify predictors of warfarin discontinuation to improve the management of these patients.
In this study, greater comorbidity and higher stroke risk, as measured by CHADS2 scores, of patients with NVAF were associated with a greater likelihood for persistence with warfarin therapy. These findings are similar to that of Deitelzweig et al and Spivey et al who also found that higher stroke risk, as measured by CHADS2 scores, was associated with a lesser likelihood for discontinuing warfarin (ie, persistent). 6 The calculation of the CHADS2 score includes history of stroke or transient ischemic attack (TIA) as a component. Therefore, those patients with NVAF with higher CHADS2 scores may have a history of stroke or TIA, which may influence treatment decisions by care providers and patients, such that patients continue with warfarin therapy. Although Spivey et al did not find that CCI score of patients with NVAF influenced discontinuation of warfarin therapy, the presence of comorbid conditions, including diabetes, hypertension, history of stroke or TIA, and congestive heart failure, was associated with a lower risk of discontinuing warfarin therapy. 6 Although our findings show that greater comorbidity is associated with persistence with warfarin therapy, in another recent study conducted among patients with NVAF in the same IDN setting, we found that greater CCI score and the presence of diabetes, congestive heart failure, peripheral vascular disease, coronary artery disease, and pulmonary diseases were associated with a lower likelihood of having a high warfarin time in therapeutic range (TTR). 22 Therefore, while greater comorbidity of patients with NVAF may indicate a greater likelihood for persistence with warfarin therapy, providers should be alerted of these patients potentially having suboptimal warfarin therapy, based on lower TTR. 22 Further study is needed to better understand the clinical characteristics of patients with NVAF who discontinue or have suboptimal warfarin therapy, as patients with NVAF with certain comorbid conditions may benefit from alternative medications for anticoagulation therapy, such as DOACs.
In this real-world study of patients with NVAF managed by anticoagulation clinics in an IDN setting, total health-care resource utilization for all causes was greater among those who were persistent with warfarin therapy versus those who were not, as well as were CV-related and stroke-related health-care resource utilization. However, in comparison to patients with NVAF not persistent with warfarin therapy, inpatient admissions for all causes, hospital length of stay, and ICU length of stay were significantly less for patients persistent with warfarin therapy during the follow-up period. For both study cohorts, the majority of inpatient admissions were CV related, which were similarly lower in number and associated with significantly less lengths of stay in the hospital and in the ICU for patients with NVAF persistent with warfarin therapy versus those who were not. Furthermore, total health-care costs for all causes remained lower for patients with NVAF who were persistent with warfarin therapy versus those who discontinued warfarin therapy after adjusting for comorbidity and stroke risk. Additionally, total stroke-related health-care costs were lower for patients who were persistent with warfarin therapy versus those who were not. The greater utilization of outpatient care services of patients with NVAF persistent with warfarin therapy may have potentially contributed to the avoidance of the more costly use of inpatient services, relative to patients who were not persistent. Although Casciano et al did not directly compare health-care costs of persistent warfarin users to those who were nonpersistent, health-care costs were found to be lower for patients with AF with high adherence to warfarin in comparison to patients with AF who did not take warfarin as a result of decreased inpatient utilization. 23 Also, in the study by Casciano et al, health-care costs were similar for patients with AF with low adherence to warfarin therapy and patients with AF who did not receive warfarin. 23
Study Limitations
In this retrospective study, we were only able to evaluate the association and not the causality between health-care resource utilization and costs with warfarin persistence status. Other patient variables, such as socioeconomic factors, were not taken into account in this analysis and may influence the results. Warfarin TTR was not evaluated in this study, and thus, actual clinical efficacy of anticoagulation therapy was not assessed for patients within the study cohorts. In regard to bleeding-related health-care resource utilization, patients may not be seeking health-care services for very minor bleeding, such as a regular nose bleed. Thus, the bleeding services identified in this study may be more likely to represent either major bleeding or clinically relevant bleeding. Also, nonpersistency with warfarin therapy may be the result of an occurrence of a bleeding event or concern for bleeding and therefore may not necessarily have led to a bleeding event.
Although warfarin prescription information was obtained from EMRs within the IDN, prescriptions may not be filled or may be filled and not taken by the patients, and therefore, there are limitations for using documented prescriptions as a proxy for medication compliance. Some patients with NVAF may have a primary care physician outside the EMR system represented in the data source for this study, and their warfarin usage and monitoring may have not been entirely captured in the EMR system. This may have led to an underestimation of warfarin persistence among our study population. On the other hand, this IDN is the dominant medical service provider system in the geographic region, and it is therefore likely that the IDN records contain the majority of patient health-care encounters. Patient data came from a single health system that cares for a primarily Caucasian population in a mostly rural region of Pennsylvania and therefore may not be generalizable to other study populations. The EMR databases are subject to coding errors (coding for the purpose of rule out rather than actual disease and undercoding) either by the health-care provider or because of limitations imposed by the database. However, these issues were at least partially ameliorated with the use of this IDN database, that is, a high-quality EMRs database.
Conclusion
Patients with NVAF who have greater comorbidity and stroke risk are more likely to be persistent with warfarin therapy, which was associated with a lesser likelihood for hospitalization during the follow-up period. Furthermore, patients with NVAF who are persistent with warfarin therapy, in comparison to those who are not, have lower all-cause and stroke-related health-care costs.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: S. Deitelzweig is a consultant for Bristol-Myers Squibb and Pfizer. M. Evans is a consultant to MedMining, which received funding from Bristol-Myers Squibb and Pfizer in connection with conducting this study. K. Gupta is an employee of Bristol-Myers Squibb and owns stock in the company. J. Trocio is an employee of Pfizer and owns stock in the company. M. Lingohr-Smith, B. Menges, and J. Lin are employees of Novosys Health, which has received research funds from Bristol-Myers Squibb and Pfizer in connection with conducting this study.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study and development of this manuscript was funded by Bristol-Myers Squibb and Pfizer.