
Abstract
Chronic immune thrombocytopenia (ITP) carries a poor prognosis in the elderly patients. Increasing evidence proposes that a subgroup of patients with chronic ITP may be more susceptible to ischemic stroke. An 84-year-old Caucasian man with multiple ischemic stroke risk factors presented with acute onset of slurred speech, confusion, and unsteady gait. Physical examination and neurologic imaging were consistent with a new left thalamic infarct. Platelet counts ranged between 40 000 × 109/L and 65 000 × 109 /L. Antiplatelet therapy for his newly acquired stroke was not initiated considering his low platelet counts and for mildly symptomatic thrombocytopenia, and the patient was discharged home. Both hematologic and neurologic guidelines for the management of chronic ITP and stroke have contradictory goals. Although anticoagulation is mandated in acute stroke, ITP causes low platelet counts that increase bleeding complications.
Introduction
According to a recent collaboration of an international experts in the field of immune thrombocytopenia, chronic immune thrombocytopenia (ITP) is defined as an autoimmune condition that results in a platelet count of <100 × 109/L for more than 12 months of duration. 1 The pathophysiology of ITP is described as autoantibody-mediated platelet destruction with impaired platelet production. 2 Unlike its acute form which is more frequent in children and more likely to regress, chronic ITP is seen primarily in adults and remission is uncommon. 3 Immune thrombocytopenia is further categorized as primary or secondary ITP—primary ITP is a diagnosis of exclusion, while the later is the result of underlying causes. 2
Management of chronic ITP is guided by recommendations set by the American Society of Hematology 3,4 in 1996. A platelet count of 30 000 × 109/L is the treatment threshold of ITP and 50 × 109/L in less sedentary patients—a patient’s symptomatology supersedes these values depending on the severity of bleeding manifestations. First-line management currently includes high-dose steroids, intravenous immunoglobulin therapy, anti-Rh antibodies, splenectomy, rituximab, and thrombopoeitin mimetics. Clinical manifestations are mucocutaneous bleeding, petechiae, and purpura. 2,5 The most serious morbidity is intracranial hemorrhage. 6 Ischemic stroke in association with chronic ITP is far less common and is rarely reported in the literature. 7 In this report, we describe a case of ischemic stroke in the setting of chronic ITP in an elderly patient.
Case Presentation
An 84-year-old Caucasian man with stage 1E extranodal marginal zone lymphoma of the conjunctiva diagnosed in 2006 in remission, coronary artery disease, hypertension, hyperlipidemia, ischemic stroke without residual defect in 1997, and documented chronic thrombocytopenia since 1999, was transferred from an outside hospital to our institution for acute onset of slurred speech, confusion, and unsteady gait. Physical examination was notable for mild-to-moderate aphasia and dysarthria, mild cognitive deficits, and decreased vibration and position sense in the left lower extremity to the ankle with no other focal findings. His vital signs were within normal limits, and the patient’s history of hypertension was treated with furosemide 40 mg daily, lisinopril 40 mg daily, and nifedipine (extended release tablet) 30 mg daily, while his home regimen of atorvastatin 40 mg was continued for his history of hyperlipidemia. One day prior at the outside institution, the patient received platelet transfusions for an initial platelet count of 11 000 × 109/L (normal 150 000-400 000 × 109/L) with an appropriate response. The patient was given 1 dose of oral prednisolone 50 mg in our emergency room, given his previously low platelet count. Manual platelet counts ranged between 40 000 × 109/L and 65 000 × 109/L. Magnetic resonance imaging and computerized tomography showed a new left thalamic infarct, changes consistent with small vessel ischemic disease, and an 8-mm left-sided supraclinoid aneurysm (Figure 1 ). No evidence of hemorrhagic bleeding was appreciated. A cardiac echocardiogram showed left ventricular dysfunction and telegraphic monitoring was unremarkable. A carotid ultrasound showed 1% to 39% stenosis bilaterally. Outside hospital records revealed Helicobacter pylori on recently biopsied gastric samples, and the patient was started on amoxicillin 1000 mg twice daily, clarithromycin 500 mg twice daily, and pantoprazole 40 mg twice daily for H pylori eradication. Antithrombotic therapy was not initiated considering his low platelet counts and for a history of mildly symptomatic thrombocytopenia, and the patient was discharged home.
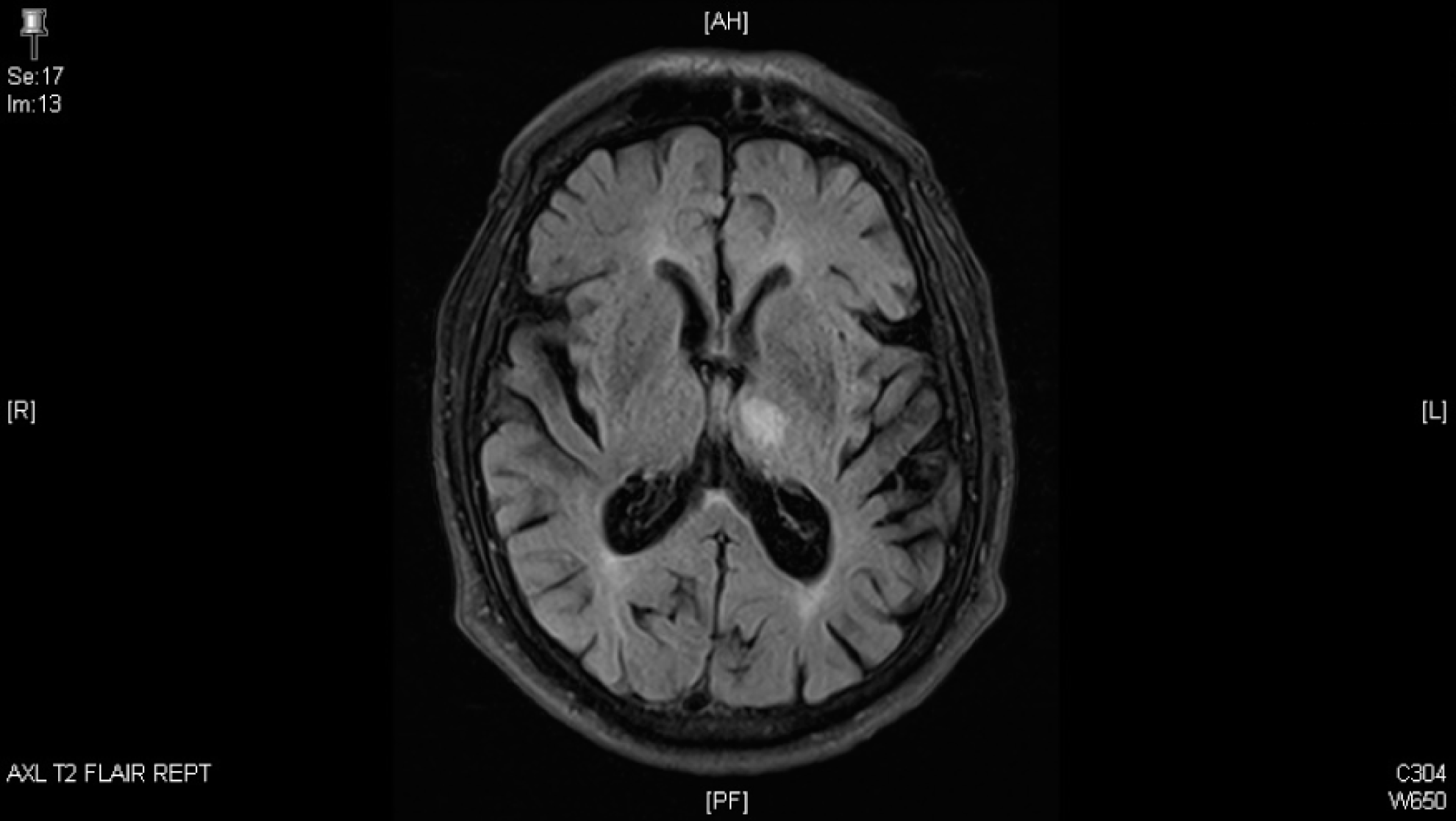
Magnetic resonance image with a focal area of hyperintensity involving the left thalamus consistent with an acute ischemic event.
A thorough review of the patient’s chronic thrombocytopenia reveals a platelet count in the range of 150 × 109 /L to 250 × 109 /L in 1999, with a steady decline over the next 10 years to his most recent platelet count spanning between 30 × 109 /L and 60 × 109 /L. Our patient established care at an outside hematologist years before his presentation to our institution, where a bone marrow biopsy performed was normal. A medication review shows that the patient had never been on heparin or other drug known to cause thrombocytopenia. The patient’s thrombocytopenia did not respond to a trial of rituximab years prior but did respond temporarily after anti-Rh antibody treatment in 2005. A previous coagulopathy workup was negative. Peripheral blood smears were unremarkable other than the decreased quantitative platelets. Hepatitis and human immunodeficiency virus (HIV) serologies have also been negative, and immunofixation and serum protein electrophoresis studies were unremarkable. In regard to our patient’s symptomatology, our patient bruises and bleeds with minor trauma and had 1 prior instance of diffuse purpura after aspirin therapy for his first ischemic stroke in 1997. He otherwise has no history of serious bleeding.
Discussion
The differential diagnosis of our patient’s thrombocytopenia includes primary ITP versus secondary ITP. Possible secondary causes in our patient include H pylori-induced ITP, myelodysplastic syndrome, or other lymphoproliferative disease. A normal bone marrow biopsy and no other significant abnormal hematologic laboratory findings excluded many of the possible causes for diagnoses. Our patient’s thrombocytopenia was deemed multifactorial and likely acquired as our patient had newly diagnosed ITP prior to 10 years. He otherwise had consecutive normal range platelet counts throughout most of his adulthood. Given his recent diagnosis of H pylori, we could not exclude H. pylori-induced ITP as a possible etiology for his thrombocytopenia. 8,9
Relating to our patient’s neurologic clinical presentation, the unique manifestation in our patient was the finding of ischemic stroke in the setting of chronic ITP, when hemorrhagic stroke would otherwise be expected. Chronic ITP is known to carry a poor prognosis in the elderly patients because of the risk of hemorrhagic stroke. 6 In the most recent recommendations published by the American Society of Hematology, a tabulated review of the available literature showed the rate of fatal hemorrhage in older patients to be 5%, with the majority of these incidents secondary to intracranial hemorrhage. 3 The predicted risk of fatal hemorrhages due to any cause in a patient 60 years and older with persistently low platelet counts is estimated to be 13% per year, though newer therapies for ITP likely lower these estimates. 3,10
Nevertheless, newer literature suggests that thrombotic complications in patients with ITP may be more substantial than previously thought. A review by Doeuvre et al shed light on the notion of procoagulant platelet-derived microparticles associated with ischemic cerebrovascular events and transient ischemic attacks. 11 The authors highlighted a study involving a study cohort with ITP, cerebral small vessel ischemic disease, and elevated procoagulant platelet-derived microparticles. Ahn et al and related in vitro studies suggest that raising platelet counts in patients with a history of ischemic changes on cerebral imaging may increase the risk of thrombotic complications and to consider this possibility in patients who have relatively asymptomatic thrombocytopenia. 12–14 More recently in 2010, a retrospective study assessing thromboembolic events among 1070 adult patients with primary ITP found the incidence of venous thromboembolic events to be greater in the study group than the disease-free group, with an incidence rate ratio of 1.57 (95% confidence interval [CI] 1.04-2.37) and a hazard ratio of 1.58 (95% CI 1.01-2.48) that was statistically significant. 15
Extrapolating this information to our patient, we face a conundrum in his therapeutic management. Our patient has a number of risk factors for a subsequent ischemic stroke, including advanced age, hypertension, heart disease, and hypercholesterolemia. His risk factors and history of ischemic stroke favor the use of antiplatelet therapy, but his history of purpura after aspirin use and initial platelet count of 11 000 × 109/L deter the initiation of secondary stroke prevention. In terms of prognosis, the mortality rate of hemorrhagic stroke far exceeds ischemic stroke by up to 4-fold within the first 3 months, and the hemorrhagic strokes overall tend to be more severe. 16 In patients with ITP and small vessel ischemic cerebral changes, glucocorticoids and danazol have been used to stabilize platelet counts initially, with the addition of antiplatelet therapies once the platelet counts have relatively normalized without major bleeding events. 12 Additional studies that evaluate the optimal management in elderly patients with chronic ITP and association with ischemic stroke, as well as prospective trials that better define any association between chronic ITP and procoagulant activity are recommended.
Conclusion
In summary, chronic ITP carries a poor prognosis in elderly patients with respect to their risk of hemorrhagic stroke. Future studies are needed to better elucidate a relationship between chronic ITP and thrombosis-related complications as well as to establish safety profiles of antiplatelet therapy in these patients.
Footnotes
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors received no financial support for the research, authorship, and/or publication of this article.