
Abstract
Objective:
Data regarding cerebral venous thrombosis in North Africa are scarce. This study aims to identify the clinical features, risk factors, outcome, and prognosis of cerebral venous thrombosis in Tunisia.
Methods:
Data of 160 patients with radiologically confirmed cerebral venous thrombosis, hospitalized in Mongi Ben Hmida National Institute of Neurology (Tunis, Tunisia), were retrospectively collected and analyzed.
Results:
The mean age was 37.3 years with a female predominance (83.1%). The mode of onset was subacute in most cases (56.2%). Headache was the most common symptom (71.3%), and focal neurologic symptoms were the main clinical presentation (41.8%). The most common sites of thrombosis were the superior sagittal sinus (65%) and the lateral sinus (60.6%). More than 1 sinus was involved in 114 (71.2%) patients. Parenchymal lesions observed in 85 (53.1%) patients did not correlate with cerebral venous thrombosis extent. Major risk factors were obstetric causes (pregnancy and puerperium) found in 46 (38.6% of women aged <50 years) patients, followed by anemia (28.1%) and congenital or acquired thrombophilia (16.2%). Mortality rate was of 6.6%. Good outcome at 6 months (modified Rankin Scale ≤2) was observed in 105 (87.5%)of 120 patients available for follow-up. Predictors of poor outcome were altered consciousness and elevated plasma C-reactive protein levels.
Conclusion:
Clinical and radiologic presentation of cerebral venous thrombosis in Tunisia was quite similar to other parts of the world with, however, a particularly high frequency of obstetric causes. Plasma C-reactive protein level should be considered as a prognostic factor in CVT.
Introduction
Cerebral venous thrombosis (CVT) is a rare origin of stroke, accounting for 0.5% of all strokes in Western countries and usually affecting young individuals. 1 Patients with CVT exhibit nonspecific signs and a broad spectrum of presentation, making the diagnosis challenging. 1,2 Cerebral venous thrombosis was considered an infectious disease for a long period. However, more recently, its pathogenesis has been shown to be multifactorial with a key role for thrombophilia. 1
Most large series have been reported from Western or Asian countries. 3 –7 This is, to our knowledge, the largest study reported from North Africa. We aimed to characterize the clinical features, risk factors, outcome, and prognosis of 160 Tunisian patients with CVT.
Patients and Methods
We retrospectively studied 160 CVT cases colligated in the Department of Neurology of Mongi Ben Hmida National Institute of Neurology (Tunis, Tunisia). Patients were recruited from January 2000 to December 2013 among 6084 stroke admissions.
Demographic data and the clinical, radiological, and laboratory findings were reviewed for each patient. Diagnosis of CVT was based on conventional cerebral angiography, magnetic resonance imaging (MRI)/magnetic resonance (MR) venography, or contrast-enhanced computed tomography (CT) following established diagnostic criteria. 2 As proposed by Zubkov et al, 8 a CVT scoring system was used in cases explored by MRI/MR venography (100 cases), assigning 1 point for each sinus involved with thrombosis; the superior sagittal sinus was divided into thirds, and 1 point was assigned to each third. Occlusion of each internal cerebral vein and the vein of Galen was assigned 1 point per vein.
Depending on the period between the onset of the clinical symptoms and the time of diagnosis, the disease stages were designed as acute (<48 hours), subacute (between 48 hours and 30 days), and chronic (more than 30 days), as proposed by the International Study on Cerebral Venous and Dural Sinuses Thrombosis. 3
Outcomes at discharge and 6 months after onset were classified as nondependency (modified Rankin Scale [mRs] 0-2) and dependency or death (mRs, 3-6).
For the evaluation of thrombophilic conditions, blood samples were taken and checked for serum levels of anti-dsDNA antibody, anticardiolipin immunoglobulin (Ig) M and IgG, anti-beta 2 glycoprotein I IgM and IgG, lupus anticoagulant and antithrombin III, protein C and protein S antigen and activity, and resistance to activated protein C. Patients with abnormal laboratory values were tested twice at least 12 weeks apart.
For statistical data analysis, the Statistical Package for the Social Sciences V 15.00 was used. Bivariate analysis was performed using χ2 test or Fisher exact test for categorical variables and using Student t test for continuous variables. The statistical significant factors were further analyzed by multivariate logistic regression analysis to identify the independent predictors of outcome. Two-tailed P values <.05 were considered significant. Ethical approval for the study was obtained from the local ethics committees at Mongi Ben Hmida National Institute of Neurology.
Results
Demographic Characteristics
A total of 160 Tunisian patients with CVT were recruited for this study. There were 133 women and 27 men, with a male to female ratio of 1:4.92. The mean age of the patients was 37.3 years (standard deviation [SD], 18.84; range, 12-90 years). In the age groups by decades, the highest frequency was seen in the third decade (n = 58).
Clinical Signs and Presentations
The median delay from the onset of symptoms to diagnosis was 5 days (mean = 16.4, SD = 46.9). The mode of onset was acute in 59 (36.8%) patients, subacute in 90 (56.2%), and chronic in 11 (6.8%). Clinical signs and symptoms are summarized in Table 1.
Clinical Signs and Symptoms.a
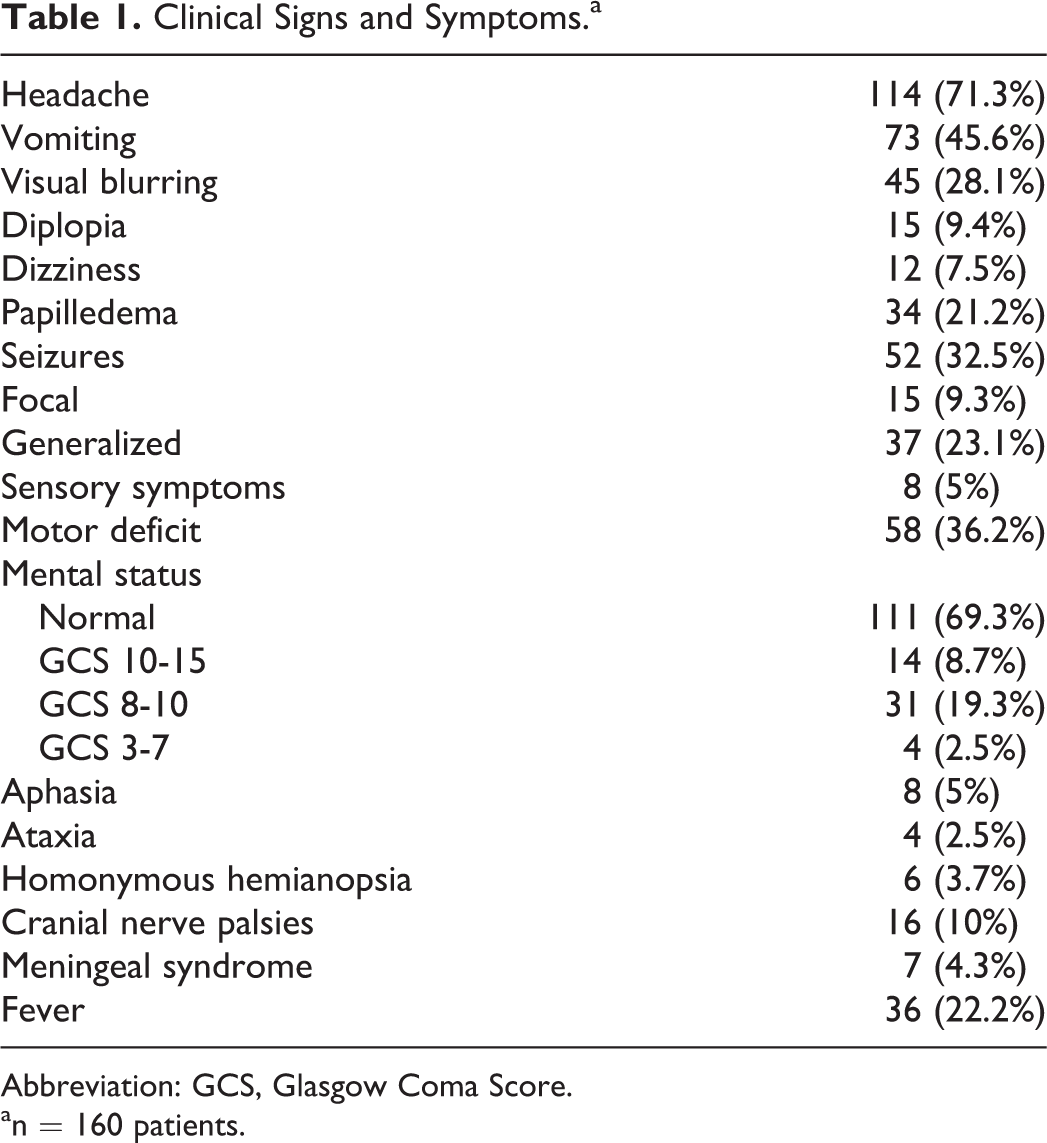
Abbreviation: GCS, Glasgow Coma Score.
an = 160 patients.
Headache (71.3%) was the most common symptom followed by focal motor deficits (36.2%) and seizures (32.5%). The most common clinical presentation was focal neurologic symptoms (either focal motor/sensory deficits or focal seizures) found in 67 (41.8%) patients followed by isolated intracranial hypertension in 44 (27.5%) patients.
A diffuse encephalopathy presentation, with reduced consciousness or generalized seizures and no focal symptoms, was observed in 5 (3.1%) patients. A cavernous sinus syndrome with painful ophthalmoplegia and chemosis was found in 3 (1.8%) patients. Five (3.2%) patients experienced headaches with a normal neurologic examination.
Neuroradiological Findings
The diagnosis of CVT was established in most patients (86%) by multiple imaging methods. The CT scan was normal in 52 (36.8%) of 141 cases. The MRI/MR venography was performed in 100 patients and cerebral angiogram in 7 patients. A summary of neuroradiological findings is given in Table 2.
Neuroradiological Findings.a
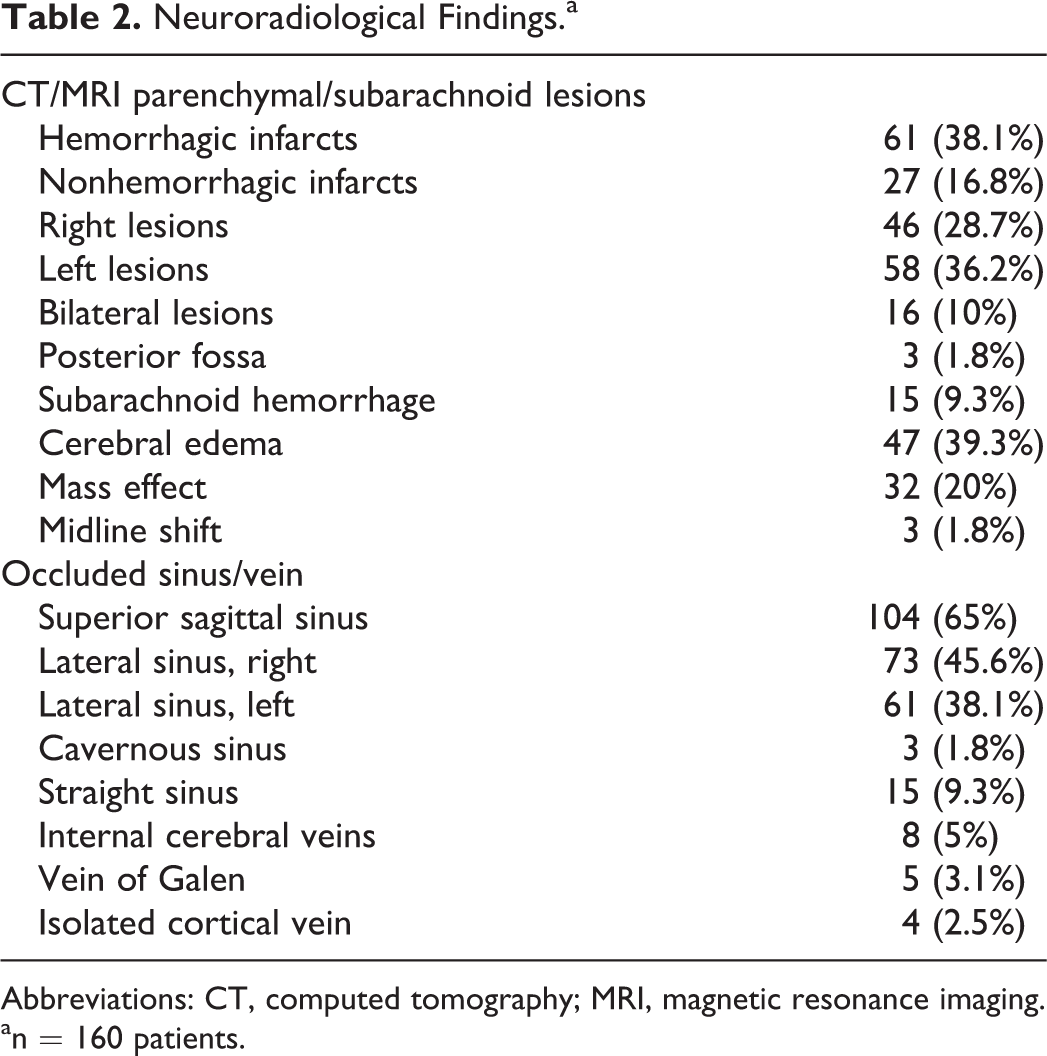
Abbreviations: CT, computed tomography; MRI, magnetic resonance imaging.
an = 160 patients.
The superior sagittal sinus was the most common site of occlusion (104 patients, 65%), followed by the lateral sinus (97 patients, 60.6%) and the straight sinus (15 patients, 9.3%). Abnormalities were found in 2 or more sinuses in 114 (71.25%) patients, and the mean CVT extension score was 3.2 ± 1.6.
Parenchymal lesions were observed in 85 (53.1%) patients and mainly presented as hemorrhagic infarcts. They were bilateral in 16 (10%) patients.
In most cases, the occlusion of the superior sagittal sinus resulted in unilateral frontoparietal lesions and lateral sinus thrombosis caused unilateral posterior temporal lesions. In 3 (13.6%) of 22 cases of deep venous system thrombosis, the thalamus showed edematous lesions. The CVT extension scores did not correlate with the presence of parenchymal lesions.
Biological Findings
Lumbar puncture was performed in 37 patients: 7 (18.9%) patients had >5 cells and 18 (48.6%) patients had >45 mg/dL protein. Hyperleukocytosis (white blood cells >11 × 109/L) was found in 32 (20%) cases and thrombocytosis (platelet count >450 × 109/L) in 24 (15%) cases. Forty-five (28.1%) patients were anemic (hemoglobin level <10 g/dL) and 11 of them were in the postpartum period. Eighteen (11.2%) patients had both anemia and thrombocytosis. Erythrocyte sedimentation rate was elevated in 78 (48.7%) cases, and plasma C-reactive protein (CRP) level was above 6 mg/L in 48 (30%) cases. Laboratory findings of cases with a prothrombotic condition are presented in Table 3.
Risk Factors for Cerebral Venous Thrombosis.a
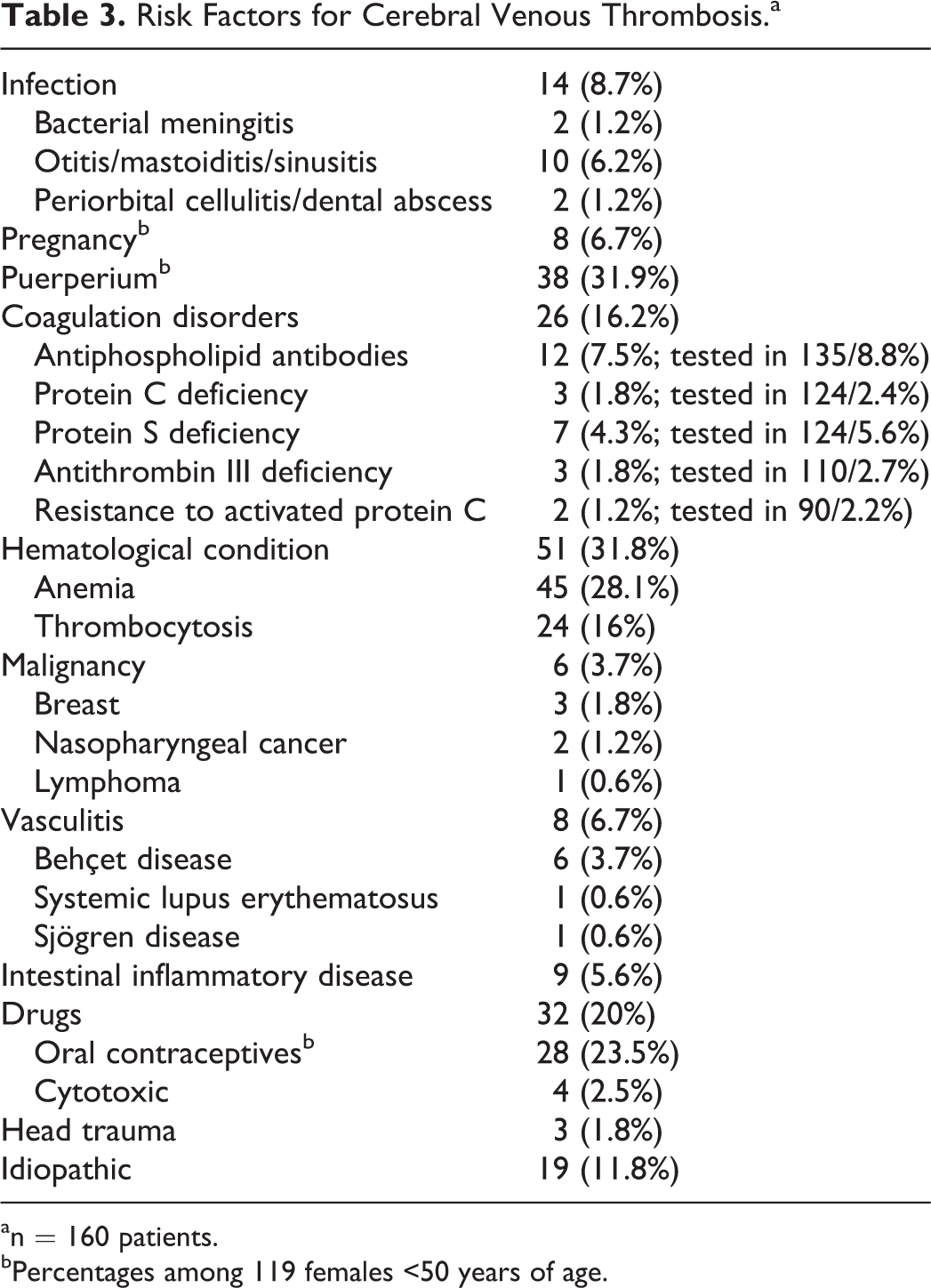
an = 160 patients.
bPercentages among 119 females <50 years of age.
Risk Factors and Comorbidities
Cerebral venous thrombosis was associated with 2 or more underlying causes in 63 (39.3%) patients. The most common risk factors were obstetric causes (pregnancy and puerperium) found in 46 (38.6% of women aged <50 years) patients, followed by anemia in 45 (28.1%) patients and congenital or acquired thrombophilia in 26 (16.2%) patients. Coagulation disorders were mainly due to antiphospholipid syndrome and protein S deficiency. Two patients had a resistance to activated protein C, associated in 1 case with lupus anticoagulant. Reactive thrombocytosis was found in 24 patients with no myeloproliferative disorder identified. Celiac disease was observed in 2 cases and hypothyroidism in 1 case. Risk factors are summarized in Table 3.
Treatment
Regarding treatment methods, most patients (157 cases, 98.1%) were treated, even in cases of hemorrhagic infarcts, with unfractionated heparin followed by warfarin, with the international normalized ratio maintained between 2 and 3. Additional treatments included antiepileptic drugs (52 patients, 32.5%), osmotherapy (5 patients, 3.12%), steroids (9 patients, 5.62%), and acetazolamide (11 patients, 6.87%). Twenty (12.5%) patients required intensive care unit admission and 2 (1.25%) patients had decompressive craniotomy.
Patient Prognosis
Mean hospital stay was 16.2 ± 8.6 days. Six (3.7%) deaths occurred in the acute phase. Six-month follow-up was available for 120 patients (75%). Of these, 91 (75.8%) patients had complete recovery (mRs, 0-1), 14 (8.7%) had partial recovery (mRs, score 2), 7 (5.8%) were dependent (mRs, score 3-5), and 2 (1.6%) were dead. Sequelae included focal motor deficits in 9 (5.6%) cases, epilepsy in 4 (2.5%) cases, and optic atrophy in 3 (1.8%) cases.
Median length of follow-up was 18 months (mean = 29.5, SD = 30.6). Two (1.2%) patients had recurrent CVT in relation to Behçet disease in 1 case and without identified cause in the other. On multivariate analysis, predictors of poor outcome (mRS, 3-6) were Glasgow Coma Scale 14 or less on admission (odds ratio: 9; 95% confidence interval [CI]: 2.2-35.6) and elevated plasma CRP levels (odds ratio: 1.18; 95% CI: 1.03-1.36). Other parameters such as age, time to diagnosis, or CVT extent did not seem to have any influence on outcome.
Discussion
Cerebral venous thrombosis is an uncommon cause of stroke accounting for 2.6% of all our hospitalized patients with stroke. It presents with a highly variable mode of onset and a wide spectrum of signs. 1,2
In our study, we found a young female predominance with a male to female ratio of 1:4.92 and the highest frequency of occurrence in the third decade. Western reports 3,4 showed comparable age distribution but less gender discrepancy, with a male to female ratio ranging from 1:1.49 to 1:2.92.
The onset was subacute in most of our cases (56.2%). Headache was the most common symptom (71.3%) and focal neurologic symptoms were the main clinical presentation (41.87%) followed by isolated intracranial hypertension (27.5%). These findings were comparable to previous studies. 3 –7 However, we found a lower frequency of isolated headache (3.21%) compared with the study of Crassard and Bousser 9 (25%). This discordance is probably due to the underdiagnosis of paucisymptomatic cases in our population.
The most common sites of CVT in the present study were the superior sagittal sinus (65%) and the lateral sinus (60.6%), which is consistent with previous reports. 3 –7 In contrast to Zubkov et al, 8 and despite using a same clot extension scoring system, the CVT extent did not correlate in our patients with the presence of parenchymal lesions.
This lack of correlation was in agreement with the study by Bergui et al. 10 It could be explained by the fact that the cerebral collateral venous circulation is highly variable. Moreover, relevant disturbances can arise from thrombosis of cortical, bridging, or medullary veins, hardly shown on neuroradiological investigations.
The pathogenesis of CVT is often multifactorial as illustrated in our study where up to 39.3% of the patients had more than 1 risk factor.
Cerebral venous thrombosis is often an obstetric complication related to a transient prothrombotic state. In fact, pregnancy induces several changes in coagulation, which persist at least during early puerperium. In addition, hypercoagulation is aggravated after delivery as a result of volume depletion and trauma. 11 Puerperium was the major risk factor identified in our patients (31.9%), which is consistent with previous North African case series 12,13 and with reports from developing Asian countries. 5,6 However, this factor was far more prevalent as compared to the West (<15% of cases), 3,4 despite a similar fertility rate (2 births per women in Tunisia). 14 This difference could be explained by a higher prevalence of anemia in our population during the puerperium and certain rituals such as the consumption of high-fat food and prolonged bed rest during the peripartum period. 11,15
In contrast to previous Western reports 3,16 and similarly to some Asian studies, 5,6 oral contraceptives were not a major risk factor for CVT in our patients. They were used in 23.5% of cases, compared with 19% in the general population of married Tunisian women aged 15 to 49 years. 17
Septic factors were found in 8.7% of our cases, which is comparable to Western studies. 3,4 Despite the high prevalence of Behçet disease in Arab countries, it was diagnosed in only 3.7% of our patients, which was <9% to 25% as reported from Middle East studies. 18,19 The frequency of Behçet disease was probably underestimated in our study, as vasculitis cases are usually hospitalized in internal medicine departments.
Thrombophilia was noted in 16.2% of our cases with congenital thrombophilia accounting for 9.3%. Antiphospholipid antibodies, which are reportedly a relevant cause of acquired thrombophilia, 20 were identified in 7.5% of our patients. Protein S deficiency was found in 4.3% of cases and represented the most frequent cause of congenital thrombophilia in our study. Conversely, the most frequent genetic mutation in European patients with CVT occurred in the factor V Leiden gene (13.7%). 21 However, this discrepancy should be considered in the light that our screening for factor V abnormalities was only based on the resistance to activated protein C testing.
Most of our patients (98.1%) were treated with unfractionated heparin. We noted a mortality rate of 6.6%, which is within the range reported in the literature (6%-15%). 3 –7,22,23 Follow-up was available for 120 patients, and in accordance with previous reports, 3 –7 outcome was overall good, with 87.5% of the patients being functionally independent.
In our patients, independent predictors of unfavorable outcome were altered consciousness and elevated plasma CRP levels. Risk factors for poor long-term prognosis reported in previous studies 3,23 were mainly coma, cerebral hemorrhage, and malignancy. We lack data on the potential predictive value of CRP in CVT, but it is a well-known independent prognostic factor in arterial stroke. 24
The limitations of our study were its retrospective nature as well as potential selection bias with the recruitment of all patients from a single department and the relatively high rate of follow-up loss. In addition, some prothrombotic conditions such as hyperhomocysteinemia and prothrombin G20210A mutation have not been investigated in our patients.
In conclusion, and despite these limitations, our study that included a large number of patients allowed a better characterization of CVT in North Africa. Preventive measures should be taken to reduce peripartum CVT risk factors, which are predominant in our population. Moreover, plasma CRP level should be considered as a prognostic factor in CVT.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.