
Abstract
Myeloma has a well-described association with venous thromboembolism (VTE). There are few dedicated studies investigating the incidence and risk factors. Many assessment scores have been suggested to estimate the risk of VTE in patients with cancer but these have been validated in solid organ tumors. The records of patients with myeloma attending a university hospital between January 2007 and December 2012 were reviewed to investigate the incidence of VTE and the associated risk factors. In all, 217 patients with a mean (standard deviation) age at diagnosis of 65 (12) years were included. Of 217 patients, 12% had an episode of VTE, 69% received at least 1 immunomodulatory agent, and 95% had low or intermediate risk of VTE according to the Khorana score. Venous thromboembolism was a frequent occurrence in this cohort. Patients had many risk factors for VTE but no one was predictive. As myeloma outcomes continue to improve, a dedicated prospective study is warranted to investigate the most appropriate thromboprophylaxis strategy.
Introduction
Multiple myeloma is a malignant disorder characterized by uncontrolled clonal proliferation of plasma cells. 1 It accounts for about 1% of malignant tumors and slightly more than 10% of hematologic malignancies in the United States. 2 The incidence is 7.7 per 100 000 with 37% of patients surviving their disease by 5 years or more. 3
Thromboembolic events are reported in up to 20% of patients with cancer 4 and are one of the leading causes of death. 5 Cancer-related thrombosis is a heterogeneous entity with many contributory factors including hospitalization, surgery, thrombogenic chemotherapy, and direct tumor effects. 6 The consequences of cancer thrombosis for patients are further disease and treatment burden, delays in treatments and procedures, prolonged hospitalization, worsened short- and long-term survival, and decreased quality of life. It also results in increased use of resources. 7 Patients with hematological malignancies have the highest risk of venous thrombosis, adjusted for age and sex. 8
Plasma cell disorders have long been associated with an increased risk of venous thromboembolism (VTE)—Catovsky et al 9 reported 14 cases of VTE in the British Medical Journal in 1970 and Srkalovic et al reported increased rates of VTE in both the monoclonal gammopathy of uncertain significance (MGUS) 10 and the amyloidosis 11 populations.
The background rate of VTE in myeloma is likely due to enhanced expression of tissue factor and vascular endothelial growth factor, 12 acquired cytokine-mediated activated protein C resistance, 13 downregulation of thrombospondin, 14 higher production of factor VIII, von Willebrand factor (VWF), and inflammatory cytokines (interleukin 6, tumor necrosis factor, and C-reactive protein). 15,16 The production of procoagulant autoantibodies with prothrombotic properties (antiprotein S40 and C41; lupus anticoagulant) has also been reported in these patients. 17 Age also plays a role as plasma cell disorders are predominantly diseases of the elderly patients with the median age at diagnosis of 69. 18
ABO blood group status has previously been identified as a risk factor for the development of thrombosis 19 in patients with malignancy 20 and pregnancy. 21 This is likely due to the influence of the ABO group on plasma VWF levels. 22 –24 Nonblood group O individuals have higher rates of both arterial and venous thrombosis. 25
Thalidomide, an immunomodulatory drug (IMiD), revolutionized the outcomes of patients with myeloma due to its antiinflammatory and antiangiogenic effects. It has been shown to be associated with a high risk of VTE, especially if used in combination with steroids or cytotoxic agents. The risk is further increased if these agents are administered without thromboprophylaxis. 26,27 Lenalidomide is also associated with an increased risk of VTE. Larocca et al found that in newly diagnosed multiple myeloma treated with lenalidomide and high-dose dexamethasone, the VTE rate was 12% if prophylaxis was not used versus 2.27% in an aspirin prophylaxis group and 1.2% in an LMWH group. 28 Conversely, Bortezomib, a proteosome inhibitor, is not assocatied with an increased rate of VTE and may in fact be protective against VTE when used in combination with IMiDs. 29
At present, much of the knowledge base for VTE in myeloma has been obtained from the setting of clinical trials for IMiDs and bortezomib. Given that the cohort of patients with myeloma is mainly elderly patients and inherent in this is both a heavy burden of comorbidities and polypharmacy, the published data may not be generalizable to all.
Many assessment scores have been suggested to try and predict a patients risk of cancer-associated thrombosis. One of the most commonly used is the Khorana score, 30 which has been extensively validated in a number of trials. 31 This has the advantage of being easy to calculate, depending on readily available data such as site of cancer, hemoglobin <10 g/dL, or use of erythropoietin stimulating agent, platelet count >350 × 109/L, leukocyte count > 11 × 109/L, and body mass index (BMI) >35 kg/m2. Although patients with myeloma were not considered in the first risk assessment model proposed by Khorana et al in Blood in 2008, they were included in the validation study published in 2010. 32 There are also myeloma-specific VTE predictive scores including one published by the International Myeloma Working Group (IMWG) 33 but these are based on expert opinion only and have not been prospectively validated.
The aim of this study was to perform a retrospective review of all the myeloma patients attending a tertiary referral center to investigate the rate of VTE and look at the risk factors associated with it.
Patients and Methods
Patients with multiple myeloma attending the hematology service in a university hospital between January 2007 and December 2012 were identified by searching the Lantis Oncology Information System (used to record outpatient activity) and the Hospital In-Patient Enquiry (HIPE) Scheme (used to record in-patient activity) for the terms myeloma, multiple myeloma, smouldering myeloma, plasma cell leukemia, plasmacytoma, plasma cell disorder, and monoclonal gammopathy of uncertain significance (MGUS). The medical records, including the pathology reports of the patients, identified were then reviewed to ensure that they met the inclusion criteria of having symptomatic multiple myeloma. The remaining patient records were then examined to ascertain patient demographics such as age at diagnosis, sex, myeloma subtype, international staging system (ISS), number of lines of therapy, exposure to IMiDs, and the presence of a secondary malignancy. The pretreatment Khorana score was then calculated for all patients. The hospital picture archiving and communication system (PACS)—Agfa IMPAX 6.4.0.4551was consulted to identify who had a history of VTE. A VTE was deemed to have occurred if there was evidence of a pulmonary embolism (PE) on a computed tomography (CT) pulmonary angiogram or CT thorax or evidence of a deep vein thrombosis (DVT) on compression Doppler ultrasound or contrast venography. Among the cases, further details were obtained such as age, duration of myeloma, M-protein level, hemoglobin, platelet count, white cell count, creatinine, immunomodulatory use, chemotherapy/high-dose steroid use, erythropoietin use, presence of central venous access device, and coexisting illnesses at the time of VTE. The study protocol was approved by the clinical research ethics committee of the institution.
Data were described using mean and standard deviation (SD) or for nonparametric distributions using median and intraquartile range (IQR). Comparison between the groups was performed using Fisher exact test for categorical variables and Mann-Whitney U test or Kruskal-Wallis test for nonnormally distributed continuous variables with 2 or more than 2 groups, respectively. Analyses were performed using Predictive Analytical Software Statistics, Version 18.0, using a 2-sided type 1 error rate of .05.
Results
Two hundred and seventeen patients were identified—see Table 1 for patient characteristics. The mean (SD) age at diagnosis was 65.2 (12.3) years. The male to female ratio was 5:3. All patients were caucasian. Overall, there were 9675 months of follow-up with a mean (SD) of 44.6 (37) months per patient.
Patient Characteristics.
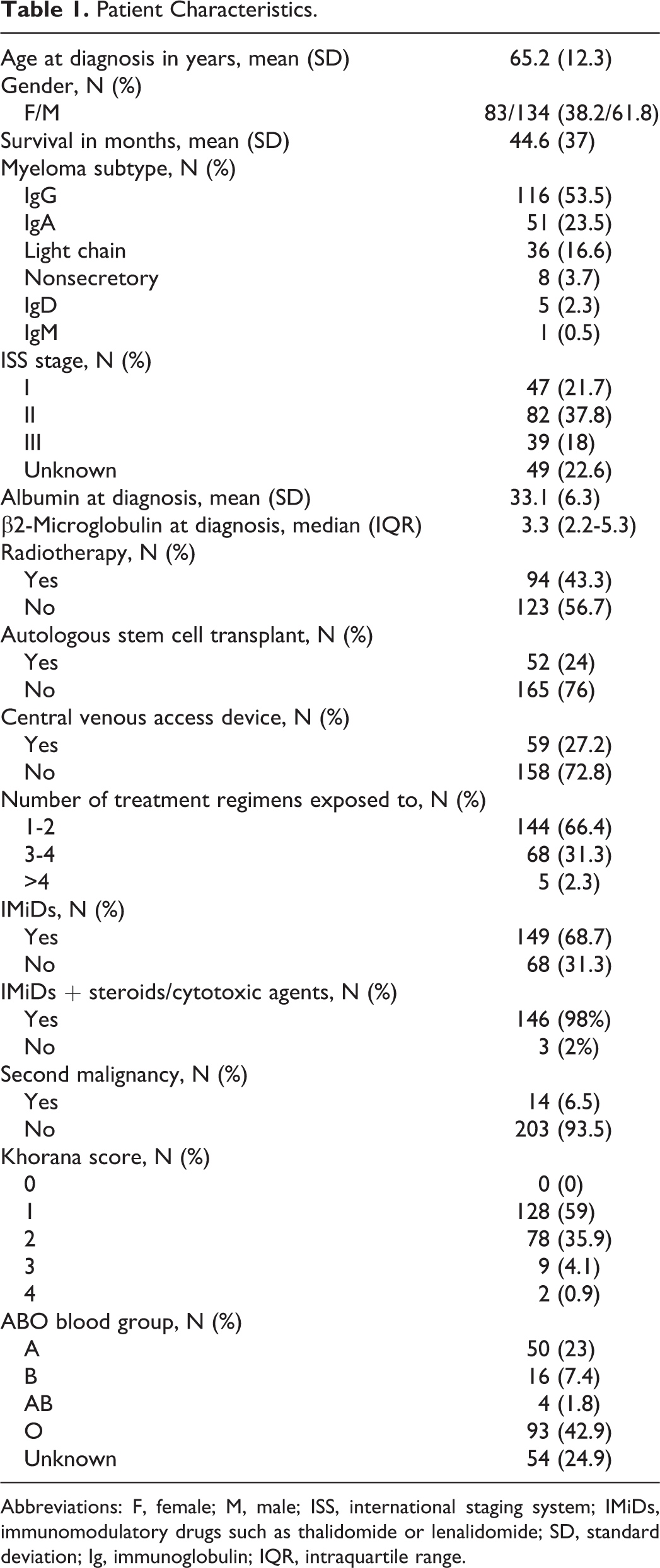
Abbreviations: F, female; M, male; ISS, international staging system; IMiDs, immunomodulatory drugs such as thalidomide or lenalidomide; SD, standard deviation; Ig, immunoglobulin; IQR, intraquartile range.
The most common myeloma subtypes were immunoglobulin (Ig) G, IgA, and light Chain. The mean (SD) albumin was 33.1 (6.3) g/dL and the median (IQR) β2 microglobulin was 3.3 (2.2-5.3) mg/L at diagnosis, resulting in 82 (37.8%) patients having ISS stage II disease. In all, 144 (66.4%) patients were exposed to 1 or 2 different types of myeloma regimens; 149 (68.7%) patients received at least 1 IMiD. These were administered in combination with high-dose steroids or chemotherapy in 98% of the cases. In all, 94 (43.3%) patients underwent radiotherapy and 52 (24%) patients underwent an autologous stem cell transplant. Fifty-nine (27.2%) patients had a central venous access device inserted at some point in their treatment.
Of the patients, 6% had a second malignancy (3 breast cancers, 1 bladder carcinoma, 1 chronic myeloid leukemia, 1 lung carcinoma, and 1 basal cell carcinoma of the skin). In all, 70 (32.3%) patients were non-ABO group O; 206 (94.9%) patients had a Khorana score of either 1 or 2, making them low or intermediate risk of VTE.
In all, 27 (12%) patients had an episode of VTE (15 PEs and 12 DVTs). The cases were then reviewed separately—see Table 2. Seventeen (63%) were male. The median (IQR) age of patients at the time of VTE was 64 (57-73) years. The median (IQR) interval since myeloma diagnosis was made was 7 (2-18) months with 11 (41%) episodes of VTE occurring in the first 6 months after diagnosis and 1 patient’s myeloma presenting as a PE—see Figure 1. The distribution of myeloma subtypes in the VTE cohort was similar to the distribution of subtypes in the cohort as a whole. In patients with IgG and IgA disease, 2 had faint bands evident only and only 4 patients had M-protein levels greater than 20 g/L.
Characteristics of Patients With VTE.a
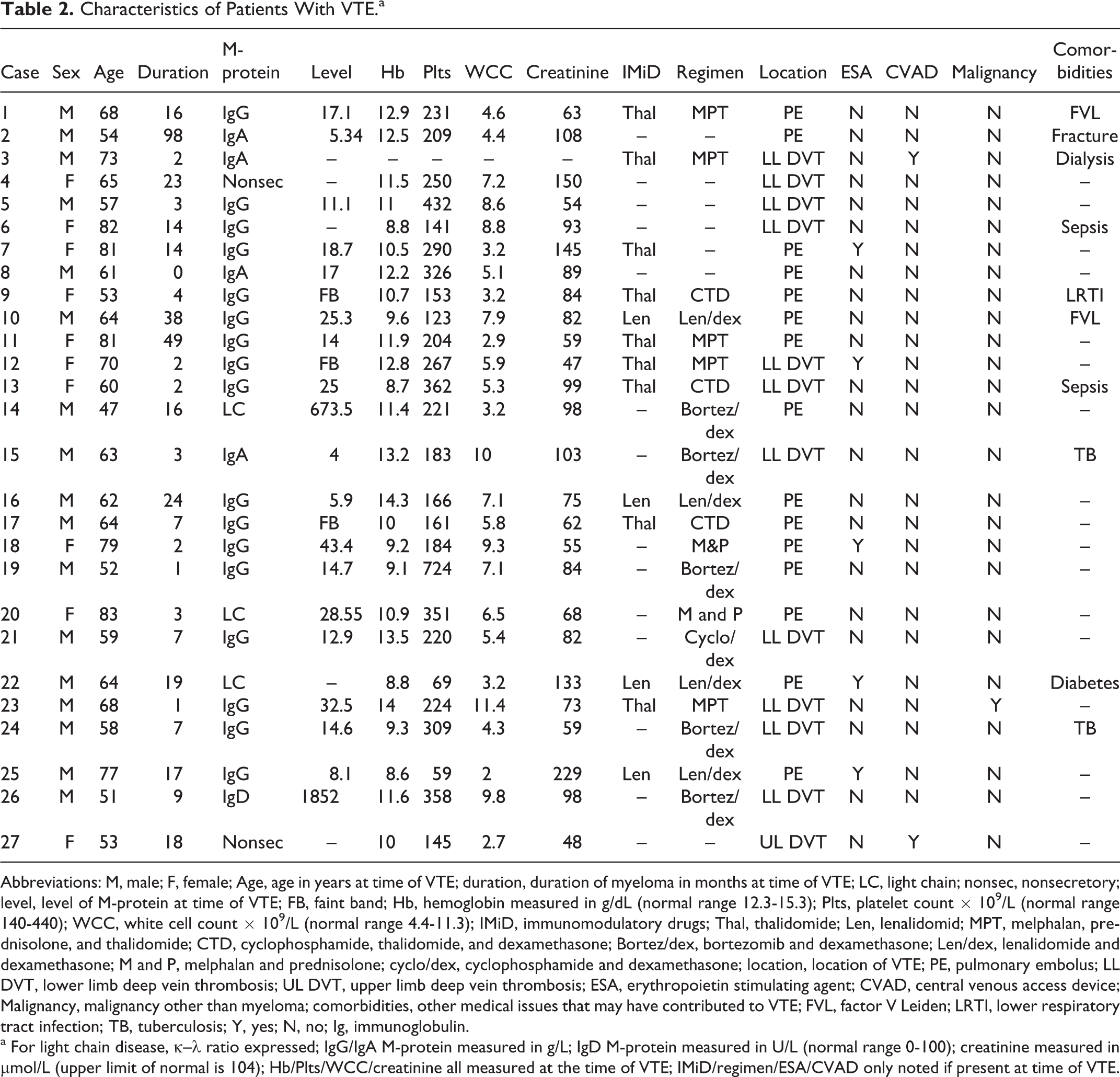
Abbreviations: M, male; F, female; Age, age in years at time of VTE; duration, duration of myeloma in months at time of VTE; LC, light chain; nonsec, nonsecretory; level, level of M-protein at time of VTE; FB, faint band; Hb, hemoglobin measured in g/dL (normal range 12.3-15.3); Plts, platelet count × 109/L (normal range 140-440); WCC, white cell count × 109/L (normal range 4.4-11.3); IMiD, immunomodulatory drugs; Thal, thalidomide; Len, lenalidomid; MPT, melphalan, prednisolone, and thalidomide; CTD, cyclophosphamide, thalidomide, and dexamethasone; Bortez/dex, bortezomib and dexamethasone; Len/dex, lenalidomide and dexamethasone; M and P, melphalan and prednisolone; cyclo/dex, cyclophosphamide and dexamethasone; location, location of VTE; PE, pulmonary embolus; LL DVT, lower limb deep vein thrombosis; UL DVT, upper limb deep vein thrombosis; ESA, erythropoietin stimulating agent; CVAD, central venous access device; Malignancy, malignancy other than myeloma; comorbidities, other medical issues that may have contributed to VTE; FVL, factor V Leiden; LRTI, lower respiratory tract infection; TB, tuberculosis; Y, yes; N, no; Ig, immunoglobulin.
a For light chain disease, κ–λ ratio expressed; IgG/IgA M-protein measured in g/L; IgD M-protein measured in U/L (normal range 0-100); creatinine measured in μmol/L (upper limit of normal is 104); Hb/Plts/WCC/creatinine all measured at the time of VTE; IMiD/regimen/ESA/CVAD only noted if present at time of VTE.
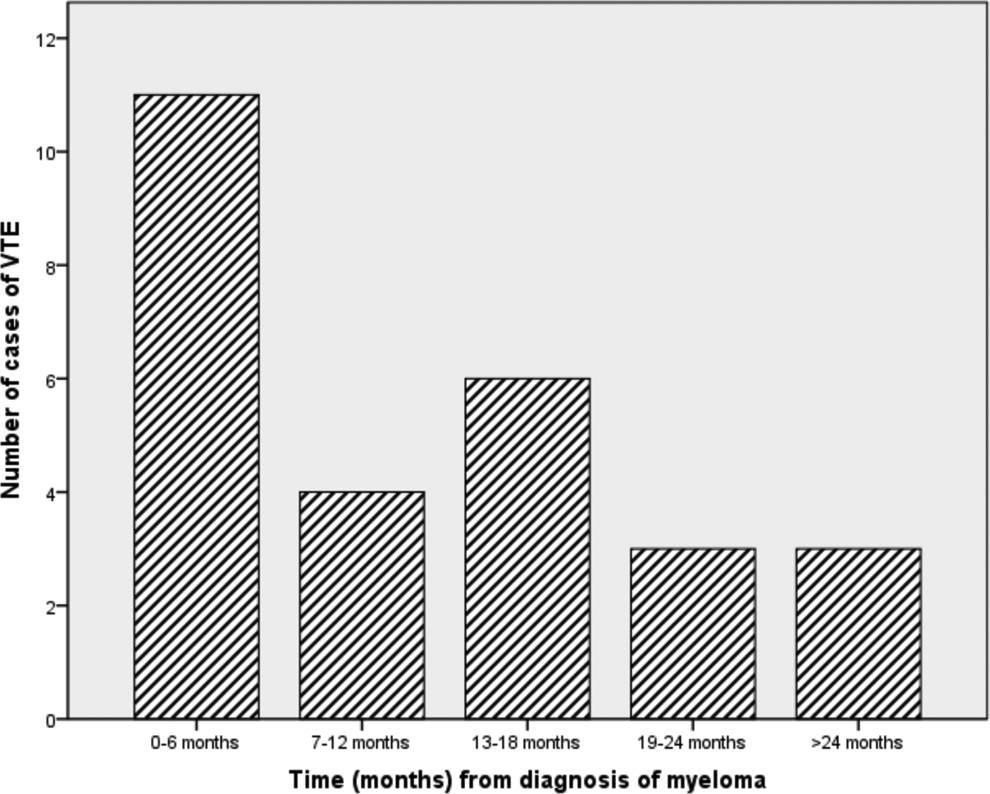
Bar chart showing the number of patients with myeloma diagnosed with VTE in 6 monthly intervals following myeloma diagnosis.
Of 27 patients, 13 were on IMiDs at the time of VTE (9 on thalidomide and 4 on lenalidomide). In all but 1 case, these were taken in combination with steroids or cytotoxic agents. In all, 5 patients were on the proteasome inhibitor bortezomib, 5 were on an erythropoietin stimulating agent, and 5 were on no treatment regimen at the time of VTE. Two patients had central venous access devices in situ.
Ten patients had at least 1 comorbidity known to increase the risk of VTE. Two had known heritable thrombophilias in the form of the Factor V Leiden mutation (1 homozygote and 1 heterozygote). The remaining 8 patients had transient risk factors—5 patients had infections serious enough to require hospitalization, 1 patient had a pathological femoral fracture requiring, 1 patient had a temporary central line inserted for dialysis, and 1 patient was hospitalized with uncontrolled diabetes; 1 patient had a secondary malignancy (basal cell carcinoma of the skin).
Patients who had a VTE had a similar median follow-up to patients who did not (33 verses 35 months). Of the 27 patients with VTE, 4 died within 6 months of the VTE. A Fisher exact test was performed to see whether patients who did not have a VTE were more likely to be alive at the end of the follow-up period but this was not found to be significant (P = .837).
When the factors used to determine the Khorana score were looked at, it was found that the mean (SD) hemoglobin was 11 (2) g/dL and the median (IQR) platelet count and white cell count were 221 × 109/L (159-313) and 5. 6 × 109/L (3.2-8.1), respectively. None of the patients in the study had a BMI >35 kg/m2. In all, 30% (8 of 27) had a hemoglobin in the normal range (12.3-15.3 g/dL) and 37% (10 of 27) had a hemoglobin of <10 g/dL or were on an erythropoietin-stimulating agent. In all, 81% (22 of 27) had a normal platelet count (140-440 × 109/L), with only 19% (5 of 27) having a platelet count >350 × 109/L. Three patients had thrombocytopenia. In all, 1 patient had a white cell count >11 × 109/L with 63% (17 of 27) having a white cell count in the normal range (4.4-11.3 × 109/L) and 30%(8 of 27) being leukopenic.
Discussion
The mean age at diagnosis, gender mix, and the distribution of myeloma subtypes in this cohort are in keeping with other published studies. ABO blood groups in this cohort are in keeping with the distribution of blood groups in Ireland. Although 36.4% of the patients in this study had only recieved 1 line of therapy, the remainder (relapsed/refractory patients) had recieved a median of 3 treatment regimens. This is less than in other studies of relapsed/refractory patients. 34,35 However, with regard to therapy, the only information available was the type of agents that patients were exposed to rather than the number of lines of therapy that a patient recieved. Therefore, if a patient recieved the same regimen on a number of occassions, it was only documented as 1 regimen so this is an apparent underrepresentation of the treatment burden of this cohort. It had initially been planned to look at the use of thromboprophylaxis, but as this was found to be poorly documented in the patient’s records, it was decided that it was not valid to include this in the analysis.
The location of VTE in this cohort was evenly split between pulmonary emboli (15 of 27) and DVT (12 of 27). Two patients had venous access device-related thrombosis—1 lower limb and 1 upper limb DVT.
Univariate analysis (see Table 3) did not show any significant association between sex, myeloma subtype, ISS, presence of a second malignancy, IMiD exposure, number of regimens, Khorana score, ABO blood group, and the occurrence of VTE. This is likely due to the small numbers in the study and the fact that in VTE risk assessment in general, the number of risk factors present rather than the occurrence of particular risk factors is what determines risk. Multivariate analysis also did not show any significant associations (supplementary data).
Univariate Analysis.
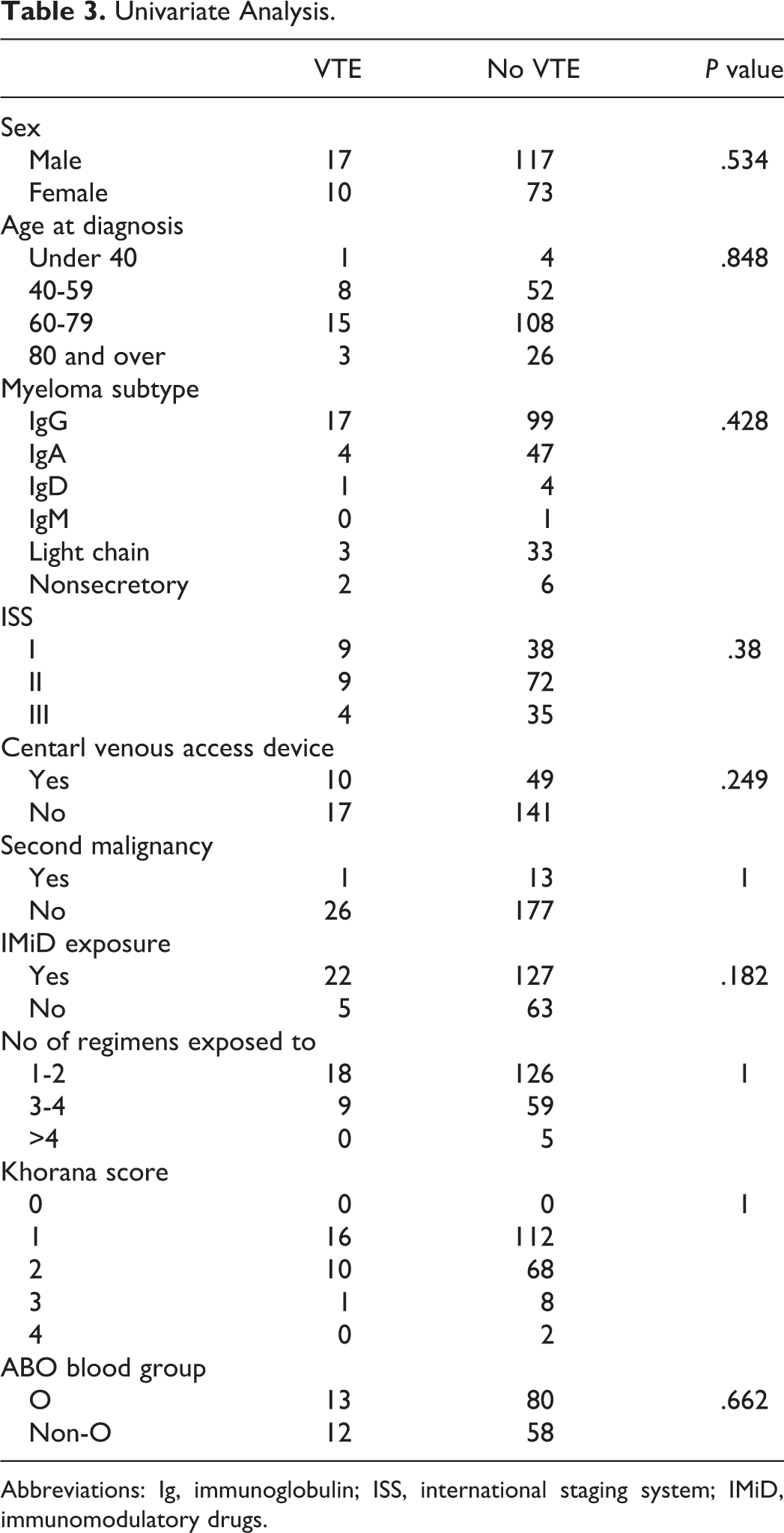
Abbreviations: Ig, immunoglobulin; ISS, international staging system; IMiD, immunomodulatory drugs.
Treatment-related thrombosis has come to the forefront of late, given the prevalence of VTE in the initial lenalidomide and thalidomide studies. However, it is important to recognize that many factors contribute to a patients VTE risk profile and it is interesting to note that 19% (5 of 27) of the cases in this study were not on treatment at the time of VTE. Myeloma-specific thromboprophylaxis guidelines such as the IMWG guideline focus on patients on thalidomide and lenalidomide but for the patients in this study, this would not have been adequate. No particular risk factor was found to be predictive of VTE. However, it is clear that the number of risk factors is important and as this is not static, it is important to risk stratify patients on an ongoing basis.
Despite being an attractive option due to the ease of use, the Khorana score was not found to be helpful in this cohort. All patients scored at least 1 as they had a diagnosis of myeloma. Although anaemia and ESA use were common, most patients had normal platelet and white cell counts. This poor correlation with VTE risk is likely due to the fact that patients with myeloma were poorly represented in the cancer-associated thrombosis study that was used to validate this score, accounting for only 2.2% of the total cohort.
This study is subject to limitations. It is a retrospective, single-center study and thereby subject to inherent biases. Given the rapidity of development and implementation of new treatment regimens, historic data may not be fully applicable to current practice. Although the agents that patients were exposed to was well documented, the number of cycles that a patient received was not. This lead to difficulty in establishing the true treatment burden of this cohort.
This study also has many strengths. It looks at all patients with myeloma that attended a tertiary referral center, the only exclusion criteria being not having symptomatic myeloma. Therefore, factors that may exclude patients from a clinical trial can also be investigated.
Cancer thrombosis has been highlighted of late with the recent publication of cancer thrombosis guidelines by both the American Society of Clinical Oncology 36 and the International Society of Thrombosis and Haemostasis. 37 Although these guidelines only minimally refer to myeloma, it is clear that the prevention of cancer-associated thrombosis is important in the treatment of all types of malignancy and is core in malignancies that have an especially high risk such as myeloma.
It appears that myeloma-related thrombosis will continue to be an issue for both physicians and patients in the future, given that a recently published phase 1 study of pomalidomide reported a 5%rate of grade 3 or 4 thromboembolic events. 34 This means that efforts need to be continued to ensure that all patients with myeloma are appropriately risk stratified and put on effective thromboprophylactic regimens.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.