
Abstract
Vascular thrombosis, both arterial and venous, is a condition associated with significant morbidity and mortality. There are multiple risk factors for thrombosis, both congenital and acquired, and in the majority of cases, these risk factors are not modifiable. Over the past 2 decades, multiple drugs (both illegal and legal) have been associated with increased risk of thrombosis. However, due to limited scientific literature regarding the prothrombotic tendencies of these drugs, there is a concomitant limited understanding of the pathophysiology of drug-induced thrombosis. As drugs are one of the few modifiable risk factors for thrombosis, further study and dissemination of knowledge regarding drug-associated and drug-induced thrombosis are essential and have the potential to lead to decreased future incidence of thrombosis. The mechanisms at the basis of the thrombophilic activity of these drugs are variable and sometimes still ill recognized. Increased levels of clotting factors, reduction in coagulation natural inhibitors, decreased fibrinolysis, activated clotting factors, increased blood viscosity, endothelial damage, and increased platelet number and activation are the most frequent causes. Arterial steal or coronary arteries no flow has also been implicated. In some cases due to the intake of several drugs, more than one mechanism is present in a given patient. The purpose of the present review is to analyze all the drugs demonstrated to be potentially thrombotic. It is hoped that a prudent use or nonuse of these drugs might result in a reduction of thrombosis-associated diseases.
Introduction
Clinical practice and society at large endorse nowadays the use and, sometimes, the misuse or abuse of pharmacological therapeutic measures. In addition, several illegal drugs are now widely used.
Oral, intramuscular, intravenous, nasal, rectal, and dermal routes are involved. Often little attention is given to the potential side effects of these compounds, especially when several drugs are taken by the same patient, at the same time.
Some of these drugs are often and widely used as antihemorrhagic preparations. Among the antihemorrhagic drugs, concentrates of clotting factors are known to be associated with thrombotic complications, particularly those which contain activated factors.
These concentrates will be dealt with only briefly in the present review since they have been extensively studied and the thrombotic complication of their use is widely known.
The purpose of this study was to evaluate the state of the art of a series of drugs or compounds that have been repeatedly associated with thrombotic events, both arterial and venous, despite the fact that their association with the clotting system appeared sometimes only indirect or minor, if any.
It is surprising to see that very few studies have ever dealt with this subject. There is 1 German study by Klöcking in 1987 1 and 2 studies in Israel in 2007 and 2013 by Ramot and Nyska. 2,3 In the latter case, the 2013 paper is an update of the 2007 paper. The first demonstration of a drug-induced (ellagic acid) hypercoagulable state in humans occurred in 1967. 4 Furthermore, it is astonishing that even good review papers on thrombophilic, prothrombotic, or hypercoagulable states have seldom discussed the problem, if any. 5 –8 This represents a clear pitfall in view of the widespread use of drugs in every country.
When dealing with the effect of drugs that may cause thrombosis, one should use the term thrombophilic or prothrombotic state, which appears more suited. The term hypercoagulable state cannot be used since it refers usually to an in vitro shortening of global tests or increase in the level of some clotting factors. Such hypercoagulable states do not necessarily evolve into a thrombotic event (Figure 1). Furthermore, thrombosis may occur without changes in blood clotting due to endothelial damage or due to increased blood viscosity. The term prothrombotic or thrombophilic is therefore more appropriate.
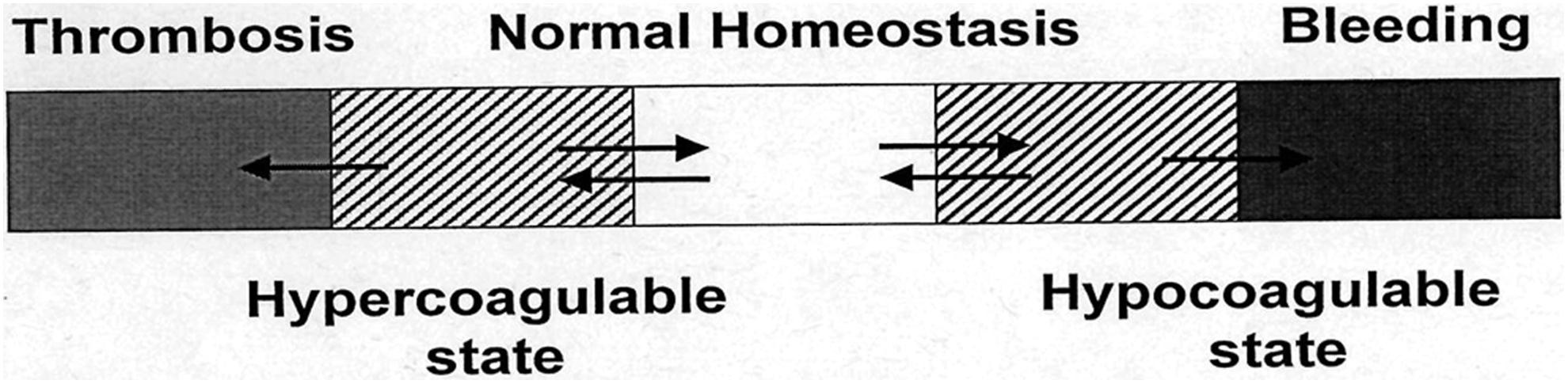
Schematic representation of blood coagulation homeostasis: there is a 2-way dynamic exchange between the normal state of blood coagulation and either hypocoagulability or hypercoagulability (double arrows). Bleeding on one side and thrombosis on the other represent instead irreversible changes (single arrow).
The term “prethrombotic” state is to be avoided since the preposition “pre” refers to a state that necessarily precedes the event, namely, thrombosis, and this is not the case in blood coagulation homeostasis. Fortunately, most thrombophilic or prothrombotic states are not always followed by the occurrence of actual thrombosis. On the contrary, the prepositions “pro” or “philic” indicate only a predisposition toward thrombosis and therefore are suited to represent the real state of conditions.
Classification of Drugs or Compounds
Since the causes of drug-induced thrombophilic states remain often ill-defined, no pathogenetic classification is feasible. Furthermore, no control studies are available for the majority of these drugs or compounds. Therefore, no structured analysis based on strict selection criteria is possible, and this represents a limitation of the study. However, the survey may still have important clinical implications. Given these circumstances, the best practical approach is to deal separately with the different drugs or groups of drugs and refer for them the available data that underline their thrombophilic or prothrombotic effect. These drugs or groups of drugs may be gathered as follows:
List of drugs that may be responsible for the occurrence of a thrombophilic state or a thrombotic event: Clotting factors concentrates. Cortisone and ACTH Oral contraceptives (OCs) and hormonal replacement therapy (HRT). Gonadotropins and related drugs for assisted pregnancy. Antifibrinolytic medications. Nonsteroidal anti-inflammatory drugs. Antipsychotic medications. Testosterone derivate (anabolic compounds). Energy drinks, cocaine, and ephedra. Tamoxifen and derivatives. Erythropoietin- and erythropoiesis-stimulating agents. Immunoglobulins (IGs). Desmopressin. Chemotherapeutic agents ( Herbal preparations. Heparins. Anti-vascular endothelial growth factor (VEGF). Immunomodulators and immunodepressant (interferon, cyclosporine). Sildenafil and similar products. Marijuana—hashish. Sirolimus and similar compounds.
We should review the state of the art for all these medications.
Clotting Factor Concentrates
Clotting factor concentrates–related thrombotic events have been known for many years and involved mainly patients with hemophilia or von Willebrand disease. 9,10
In recent years, even rare coagulation disorders have been involved, namely, fibrinogen defect, FVII deficiency, and FXI defects. 11
Fibrinogen concentrates, prothrombin complex preparation, activated FVII (a-FVII) and FXI concentrates are most frequently involved. Factor VIII concentrates may also be involved. The mechanism of action is based on the occurrence of high levels of the clotting factor and also based on the presence in the concentrates of traces of activated forms of clotting factors (a-FVII, traces of thrombin). Other still unknown causes cannot be excluded. The result is the formation of a hypercoagulable state that can be documented in vitro by shortening of global tests and by elevated levels of the clotting factors. Factor XI concentrates have been known to be occasionally thrombogenic. For this reason, antithrombin was first added to the products. In 1993, either heparin or c1 esterase inhibitor was added to the 2 concentrates available, BPL factor or Hemoleven, respectively. 12 Despite these modifications, the concentrate is still considered potentially dangerous, particularly in old age, and should be used sparingly and only for severe bleeding. 13
Needless to say that the relation between the clotting tests and the presence of thrombosis is not always present due to potential compensatory mechanisms acting in vivo (antithrombin, tissue factor pathway inhibitor [TFPI], fibrinolysis, etc). Furthermore, it has to be kept in mind that these concentrates are used prophylactically in patients with a bleeding tendency, often congenital, or in patients with actual bleeding. The type and the variable severity of the basic hemorrhagic disorder may influence the effect of the concentrates being administered.
Both arterial and venous thromboses have been described. Associated risk conditions for thrombosis are often present in these patients. Because of the danger of severe thrombotic complications, the caring physician should adequately evaluate the timing and dosage of the replacement therapy. The aFVII preparations or the so-called bypassing concentrates do not act, as originally thought, at the site of injury or bleeding, but they also cause a systemic hypercoagulable state with the potential occurrence of thrombosis in sites distal from the site of injury or from the site of bleeding. 14
Cortisone and ACTH
The first observation about the potential role of cortisone in the pathogenesis of thrombosis has come from the occasional occurrence of venous thrombosis in patients with Cushing syndrome. 15 –17 Sporadic cases of cortisone therapy–induced venous thrombosis were also reported.
This concerned usually patients on long-term cortisone therapy, for example, patients with rheumatoid arthritis or ulcerative colitis.
The mechanism at the basis of this condition has been shown to be an increased level of FVIII and von Willebrand factor (vWF). Furthermore, the dynamic composition of vWF is also altered with an increase in the high-molecular-weight dimers. 17 A decrease in fibrinolysis due to increased PAI levels has also been demonstrated. 16 Patients with Cushing syndrome or patients under long-term cortisone therapy show a hypercoagulable state which, in certain circumstance, could become actual thrombosis. 17 This interpretation has been confirmed by the observation that anticoagulant therapy has considerably benefited the patients with Cushing syndrome undergoing surgery. 18
It is worth noting that only venous thrombosis has been described. This is in agreement with the observation that the high levels of FVIII seen in certain families may be associated with an increased risk of venous thrombosis. 19 The potentially thrombotic effect of ACTH administration, particularly for the long-acting preparations, has the same underlying mechanism.
Oral Contraceptives and HRT
A worldwide literature has repeatedly demonstrated that women on OC have about a 3-fold increase in the occurrence of venous thrombosis. 20,21 Such incidence becomes higher in patients with antithrombin or protein C or protein S deficiency. 20 The effect of thrombophilic polymorphisms, such as FV Leiden and Prothrombin G to A 20210, appears to be less evident but still present, especially in older fertile women. 20,22,23 Arterial thromboses have been also described, but they are less frequent. The level of estradiol and the type of progestogens included in the OC preparation may play a role, particularly the former. 23 A long debate about the role of different first-, second-, or third-generation progestins has generated hard discussions. 21,24
The real fact is that all progestins are potentially thrombophilic. The preparations containing small doses of estradiol, regardless of the associated progestins, seem less thrombogenic. 21
The effect of HRT is also associated with an about 3-fold increase in the incidence of thrombotic events. However, in this case, the patients of older age have to be taken into consideration since age by itself may be a cause of an increased rate of thrombosis. 25 Patients with congenital thrombophilia have again further increased risk of thrombosis.
The causative mechanisms underlying this thrombophilic state are increased level of clotting factors, decreased antithrombin, and decreased fibrinolysis. 3
The best practical approach is to consider a woman on OC or on HRT, regardless of the type of medication, a potential case of thrombosis, particularly in patients with a family history or personal history of venous thrombosis.
Gonadotropins for Assisted Pregnancy
Gonadotropins or allied drugs are used widely to stimulate oocyte formation in cases of sterile women undergoing in vivo or in vitro fertilization techniques.
Several thrombotic events, mainly arterial, but also venous, have been described. Several protocols are used, but none has resulted completely safe. 26 –29 Contrary to what seen for OC or HRT-treated patients in whom venous versus arterial thrombosis is about 10 to 1, in the case of ovarian hyperstimulation, such ratio is only 2 or 3 to 1. 26,27
Improvement in techniques and adjusted dosages have recently decreased the number of these side effects. The causes are multiple and may be summarized as follows: increased estradiol, decreased fibrinolysis, decreased TFPI, and antithrombin. Hemoconcentration has also been implicated. 30
Women with a family or personal history of thrombotic events should be carefully evaluated before undergoing assisted pregnancy procedures.
Antifibrinolytic Drugs
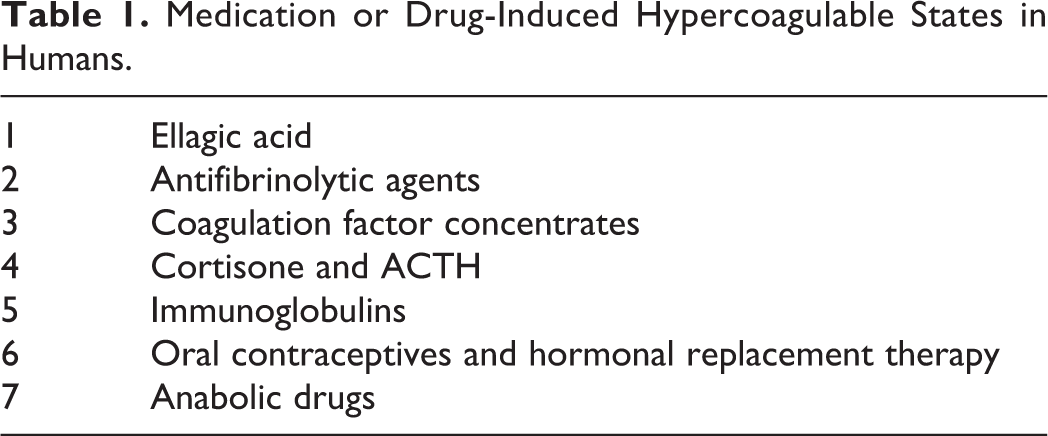
There are 2 main types of antifibrinolytic drug, namely (1) those with antiplasmin activity and (2) those with an antiactivator activity. Most of the studies involve the second group of drugs since these may be taken orally and therefore have a widespread use. E-aminocaproic acid and tranexamic acid are the 2 most common. They are used for the treatment of menorrhagia and as a general hemostatic agent. Often tranexamic acid is associated with other antihemorrhagic medications, for example, clotting factor concentrates. The increased incidence of thrombotic events, mainly venous, is demonstrated by several case reports and systemic studies. 31 –35 The thrombosis are mainly venous and may occur even in patients with congenital bleeding disorders. Antifibrinolytic drugs should not be given in the presence of hematuria since they may cause acute obstructive nephropathy and acute renal failure due to the formation of clots in the urinary tracts. This may lead to acute renal failure as occurred in a patient with hemophilia A. 36 There are other cases of misuse, for example, the association of the antifibrinolytics with activated concentrates of clotting factors. Such combination is not justified on practical considerations since the antifibrinolytic drugs would prevent the dissolution of clots that may form during the administration of such activated concentrates (Table 1).
Medication or Drug-Induced Hypercoagulable States in Humans.
Nonsteroidal Anti-Inflammatory Drugs
Nonsteroidal anti-inflammatory drugs are widely used in clinical practice. They can be subdivided into those that inhibit cyclooxygenase 1 and 2 in an equal way and those that inhibit mainly cyclooxygenase 2. The latter, known as Cox-2 inhibitors, were developed in order to eliminate the gastric effects exercised by the original Cox-1 and Cox-2 inhibitors.
Unfortunately, the Cox-2 inhibitors turned out to cause an increased incidence of arterial thrombosis, mainly myocardial infarction (MI) and strokes. 37 –41 They had to be withdrawn from the market in 2004, but some of them are still available. The thrombophilic state underlying this severe toxic effect is an imbalance in the prostacyclin to thromboxane ratio in favor of the latter with consequent occurrence of decreased prostacyclin activity and decreased fibrinolysis. The thrombotic events are mainly arterial, being the platelets the main source of thromboxane production. 37 –41
Antipsychotic Drugs
There are reports of an increased prevalence of venous thromboembolism (VTE) with the use of antipsychotic drugs. 42 –44 The complication seems to involve mainly men and refers to several medications. Clozapine seems particularly responsible. No sure increase in arterial thrombosis has been reported but for stroke. When dealing with patients who need antipsychotic drugs, it is often difficult to gather suitable information and assurance of compliance. This may explain the existence of negative reports that indicated also the need for further studies. Often these antipsychotic drugs are used in the general population for the treatment of nausea, vomiting, and vertigo. Patients should be informed of the potential risks. The mechanisms of action are not clear, but platelet activation and stasis due to vasodilation have been implicated. It has to be remembered that these patients are often bedridden with a consequent general stasis.
Testosterone and Other Anabolic Hormones
Androgenic drugs have a double effect on blood coagulation. On one side, they increase PAI production and therefore inhibit fibrinolysis. On the other hand, they may be prothrombotic because of platelet activation and increase in clotting factors levels. 3 This effect of testosterone and similar compounds is well demonstrated by what occurs in patients with hemophilia B Leiden. 45
The patients with this variant of hemophilia B show an increase in FIX at puberty so that this bleeding tendency becomes less severe. This is due to the effect of androgenic hormones on liver enzymes. This activity may be considered problematic in participants who take continuous high doses of androgens for bodybuilding or to enhance sport performances. Several cases of androgen-related thrombotic events have been published. 46 –49
Danazol is frequently implicated in these cases. This androgenic compound seems to possess, contrary to testosterone and other androgens, a fibrinolytic activity. Both arterial and venous thrombosis have been described. In these cases, it seems that the fibrinolytic effect of the drug is neutralized or overwhelmed by the increase in clotting factor levels. It is probably a question of dosages. In fact, the fibrinolytic activity of danazol has been used to treat erythropoietin-induced thrombotic events. 50
The administration of testosterone may trigger the occurrence of thrombotic events in previously asymptomatic patients with congenital thrombophilia. 51,52
Energy Drinks, Cocaine, Guarana, and Ephedra Alkaloids
These compounds can be dealt with together since they have several features in common. They all have a strong sympathetic activity.
The most frequent energy drinks are Red Bull, Rockstar, Monster, and Full Throttle. The composition varies slightly in content from one product to the other, but they are similar. They contain caffeine, sodium, taurine, vitamins B complex,
None of these substances have individually been associated with thrombotic events. The mixture preparations, on the contrary, have been associated with acute coronary thrombosis and other cardiac pathologies (arrhythmias, cardiac arrest). 54
Ephedra (Xenadrine) was banned in the United States in 2004. Subsequently, a similar compound (synephrine) was used in those “energy beverages.” However, cases of MI have been reported even with this compound. 55,56
Strictly associated with the energy drinks is the use of cocaine. The use of cocaine, however, is accompanied by a worse vascular picture. Besides the known toxic effect on cardiac rhythm, several acute thromboses have been reported. Large vessels like the aorta or iliac or renal arteries are usually involved. 57 –61
The mechanisms underlying the events for all these compounds are endothelial damage, angiitis, and platelet activation. 1,3,62
Vasoconstriction and hypertension also play a role as in the case of ephedra. 55 It has to be remembered that participants who resort to these beverages are often involved in bodybuilding activities that may include androgenic substances intake.
Tamoxifen and Similar Compounds
Tamoxifen is a widely prescribed drug for the prevention and treatment of breast cancer. The cure usually lasts 5 years. Thrombotic complications, mainly venous but occasionally also arterial, represent the main complication. 63 –67 The compound has been also demonstrated to trigger the appearance of VTE in asymptomatic participants with congenital thrombophilia, even though there is no sure evidence for a summation of effects. 63
The mechanism of action is unclear. Decrease in antithrombin and protein C together with co-mediated platelet activation has been implicated. 3,67 Reduction in TFPI has also been proposed. 64
Raloxifene, a compound similar to tamoxifen, and the new aromatase inhibitor seem to have less prothrombotic effect, especially the latter. 3
Erythropoietin and Related Drugs
The availability of recombinant erythropoietin and of other erythropoietic-stimulating agents has enabled the treatment of severe anemias due to renal failure, malignancies, and hematological disorders. Several thrombotic complications, both arterial (stroke, MI) and venous (hepatic veins), have been reported. 68 –70 The main cause for thrombosis has been maintained to be the increased blood viscosity due to the increased red blood cell mass. This is based on the results of several studies in patients with chronic renal failure. There is an increase in mortality, MI, and strokes when the therapeutic hemoglobin target is 13 versus 11 g%. 68 An increased platelet number with the appearance of young active platelets and an effect on endothelium causing increased FVIII and vWF production have also been postulated. 3,68
Strictly associated with the erythropoietin-related thrombosis are recent studies on thrombopoietin secretion stimulants. The thrombopoietin receptor agonists (romiplostim and eltrombopag) recently introduced in the treatment of chronic immune thrombocytopenia have been shown to be occasionally associated with thrombotic events. 71,72 No definite study is yet available, but it is conceivable that an increase in platelet count in patients who are also receiving or have received cortisone may cause thrombosis.
Immunoglobulins
The intravenous administration of IG, especially if prolonged, has been associated with the appearance of both arterial and venous thrombosis. 73,74 This has occurred mainly in patients with immune thrombocytopenic purpura but also in other conditions. The underlying causes have been maintained to be increased blood viscosity, contamination of the IG preparation with FXI, and increased platelet number due to the IG therapy. The concomitant or recent past use of cortisone has also been implicated.
A careful evaluation of patients, reduced doses, avoidance of association with cortisone therapy, short cycles of therapy, and continuous monitoring of platelets level are indicated during IG therapy.
Desmopressin
1-Deamino-8d-arginine vasopressin or desmopressin has been widely used for the treatment of bleeding. The compound has been proposed for the treatment of congenital or acquired bleeding disorders on the basis of its capability to release vWF and FVIII from the endothelium. However, intravenous administration of desmopressin has been reported to have caused arterial occlusions (strokes and MIs) in a few normal (nonbleeding) participants and also in patients with hemophilia A or von Willebrand disease. 75,76
Therefore, its use should be very careful and avoided if preexisting prothrombotic conditions exist. The thrombotic complications are mainly arterial. Venous thrombosis has been described only rarely. 77 The underlying mechanism is the liberation from the endothelial wall of massive doses of FVIII and vWF, mainly which composed of high-molecular-weight dimers. These dimers are known by their turn to activate platelets.
Chemotherapeutic Agents
Several chemotherapeutic agents (mitomycin, bleomycin, cis-platinum,
Thalidomide is an immunomodulatory drug that was withdrawn in 1961 from the market because of its teratogenicity. It is now used in the therapy of multiple myeloma and in other inflammatory and autoimmune disorders. It has been associated with thrombosis, especially when used together with other chemotherapeutic agents and cortisone. Venous thromboembolism is more frequent, but occasional arterial thrombosis has also been described. 78 –82
The mechanisms underlying this tendency for thrombosis seem related to platelet activation and reduced levels of thrombomodulin. When dealing with thrombosis occurring in patients with cancer, one must always keep in mind that the condition is by itself often a thrombophilic condition.
Herbal (Preparation) Drinks
Several herbal preparations, sometimes called “bush teas,” have been associated with Budd-Chiari syndrome. Plants contain pyrrolizidine alkaloid in different preparations, and this substance has been repeatedly incriminated since it causes endothelial damage and consequent triggering of coagulation. 83
In the natural form, pyrrolizidine alkaloids have little toxicity but become toxic pyrroles once metabolized by the liver. This effect is particularly evident in the hepatic veins and justifies the selectivity of the thrombotic manifestation. Cases of veno-occlusive disease have also been reported.
Heparin
It would seem astonishing that a compound known for its anticoagulant activity should be included among the thrombophilic or prothrombotic drugs. The reality has shown that this is the case. 84 –88 The clinical expression of the thrombophilic effect of heparin is represented by the “heparin-induced thrombocytopenia (HIT).” Such thrombocytopenia is due to an immunological mechanism (formation of antibodies against the PF4-heparin complex), and it is associated in fact with systemic thrombotic events. Thromboses are usually arterial, but they may be also venous. Patients undergoing hemodialysis seem particularly exposed. It was originally thought that unfractionated heparins, particularly those obtained from rabbit lungs, were more frequently associated with the complication. This assumption remains true, but HIT has been described also with low-molecular-weight heparin and even with synthetic pentasaccharide (fondaparinux) that mimics the structure of the area of heparin that bins to antithrombin. However, the prevalence and perhaps the gravity of the complication are reduced with these latter compound as compared to the UH. 86,88,89 In this regard, it is worth recording that, in at least 1 patient, a progressive reduction in the antibody title has been demonstrated to occur during long-term fondaparinux administration. 90
Anti-VEGF Compounds
Anti-VEGFs have been widely used during the past few years for the treatment of age-related macular degeneration. The treatment consists of repeated intravitreal injections of the compound. Mainly arterial thromboses (stroke, MI) have been described. 91 No sure data are available as to the pathogenetic mechanism underlying this form of thrombophilic state. It is likely that the long-term, repeated intravitreal injections of these compounds may cause some leakage into the circulation, and this could cause a decrease in circulating VEGF. Decreased levels of VEGF are associated with endothelial damage and disruption with consequent platelet adhesion, clotting activation, and thrombus formation. Ranibizumab seems associated with higher incidence of arterial thrombosis as compared to bevacizumab. 92
Immunomodulators and Immunodepressant (Interferon, Cyclosporine, and so on)
Interferon, in its variable preparations, is widely used in the treatment of hepatitis C in combination with ribavirin. Several case reports of retinal venous thrombosis have been described. This seems to be a specific side effect, since no thrombotic events in other districts have been reported. The underlying mechanism seems related to altered VEGF levels since the administration of anti-VEGF has been shown to be beneficial. Another potential explanation refers to the deposition of immunocomplexes in the retinal vessels. 93 –95
Cyclosporine
The compound is widely used as an immunodepressant after organ transplantations. Occasional venous thrombosis has been reported. The mechanism of action involves platelet activation and endothelial cells damage. 3
Sildenafil and Similar Compounds
Several observations of thrombotic events, mainly arterial (MI and stroke), have been reported in patients taking sildenafil for erectile dysfunction. 96 –99 In some cases, the concomitant use of cocaine or marijuana has been reported. 99,100 Venous thrombosis seems rare. 101,102 As our knowledge improved and with more precise limitations (no association with nitrates) in the selection of the patients suited to undergo this therapy, these reports became less frequent. However, an occasional thrombotic event (pulmonary embolism) has been described even recently with a similar compound (tadalafil) in a patient who had also high FVIII levels. 103 The problem of associated cardiovascular risk factors (hypertension, hypercholesterolemia, smoking, etc) has not been always duly emphasized in these case reports. No systematic study is available. Several mechanisms, besides clotting, have been considered at the basis of these vascular occlusions, namely sudden hypotension with consequent coronary steal or no flow, endothelial damage, and spasm. In the case of venous thrombosis, stasis due to vasodilatation has been implicated. 3
Marijuana—Hashish
Marijuana or marihuana is the most widely used illicit drug in the world. It is usually smoked, and it is supposed to induce a euphoric state. It has been purported to have several therapeutic effects, mainly for pain and fever. However, such effects often lack scientific proof. The drug, known also as hashish, contains several cannabinoids, the most important of which is tetrahydrocannabinol. Cannabis smoking has been associated with side effects involving the central nervous, pulmonary, and the cardiovascular systems. Only the latter will be discussed here.
Several cases of acute coronary syndromes have been reported. 104 –108 The patients affected are usually young and male. Thrombus formation in coronary arteries has been demonstrated on magnetic resonance imaging or at autopsy. Therefore, there is no doubt about the existence of a link between cannabis use and coronary occlusions. Arteritis and occasional ischemic stroke have been also reported. 109 Venous thrombosis, on the contrary, seems exceptional. 110 The causative mechanisms are still ill-defined. Platelet activation, endothelial damage, and increased oxygen demand due to tachycardia are probably involved, since venous thromboses are rare and no clotting change has ever been demonstrated. Coronary steal or coronaries no flow has also been proposed. Because of the huge economic interest, the toxicity of cannabis has been often minimized. The recent liberalization of the drug in some states of the United States with consequent taxations in order to improve the financial condition of these states is in line with the media underestimation of the problem.
The number of case reports is so large that every caring physician should include, in taking the history of the patient, information on cannabis use or abuse.
It is interesting to note that the only other illicit drug associated with arterial thrombotic events is cocaine and derivatives. No significant rate of MI has been associated with opiates.
Sirolimus and Similar Compounds
Sirolimus and paclitaxel have received great attention in the past decade for their use in drug-eluting stents (DESs) for coronary interventions.
The former is an antibiotic used as an immunosuppressor. The latter is a chemotherapeutic agent. This ability to inhibit inflammatory and proliferative actions has allowed their incorporation in stents (DES) in order to limit the inflammatory reaction seen with bare metal stents (BMSs). There have been several studies, not always univocal, which altogether have demonstrated the superiority of these DES over BMS stents. However, the DES have been implicated in the late stent thrombosis and occlusion. 111 The mechanism of action of these drugs seems to be a local hypersensitivity reaction and chronic inflammation, which may result in coagulation activation with consequent thrombosis.
Conclusion
The large number of drugs and medications involved, both legal and illegal, clearly indicate the potential clinical importance of the problem. In a medication-prone society, it is quite possible that a great number of patients may show thrombotic events because of these compounds. It is more likely that these drugs may act as a triggering and/or contributing factor in patients with congenital thrombophilia or otherwise predisposed to thrombosis (trauma, immobilization, diabetes, hypercholesterolemia, dehydration, surgery, OCs, obesity, etc), the so-called acquired thrombophilia.
There is no doubt that most of these compounds may cause the onset of a thrombophilic or prothrombotic state. This does not necessarily mean that this state should always evolve into an actual thrombosis. Similarly, patients with congenital deficiency of AT, protein C, protein S, or hyperhomocysteinemia do not always develop thrombosis in spite of the presence of a chronic hypercoagulable state. A triggering or concomitant factor is often needed.
The age of the patients at the time of the administration of the drug should also be taken in due consideration, since advanced age by itself may be considered a thrombophilic state.
This study underlines the complexity of the mechanisms that may cause the occurrence of a thrombotic event. Congenital thrombophilia is surely important, but only about 30% of these patients manifest actual thrombosis, and altogether, they represent only a part of all thromboses. It is likely that other congenital conditions predisposing to thrombosis might be discovered in the future, but this is not sure. No new polymorphism, besides those involving FV and FII, has surely been associated with a thrombophilic state. Acquired factors are equally important. Among the latter, legal and illegal drugs play a role that has been so far probably underestimated. Since patients may be treated with more than one of these drugs at the same time, a possible potentiation of effect may occur such as it has been demonstrated between tranexamic acid and cortisone. This represents a new field of investigation. The emphasis placed during the last 2 decades on congenital causes of thrombosis has probably underestimated the importance of acquired conditions. Acquired mechanisms are often multiple, variable in time and in intensity, and therefore of difficult interpretation. This is particularly true when drugs are involved (Table 2). On the contrary, congenital deficiency of AT or protein C is clear, stable conditions that can be easily detected. These studies indicate also that a distinction between a thrombophilic and a hypercoagulable state has to be always kept in mind. For some of the drugs (eg, erythropoietin), no hypercoagulable state can be demonstrated, even though they predispose to thrombotic events, namely, they are thrombophilic or prothrombotic.
Proven or Plausible Mechanisms at the Basis of Some Drug-Related Thrombophilic States.
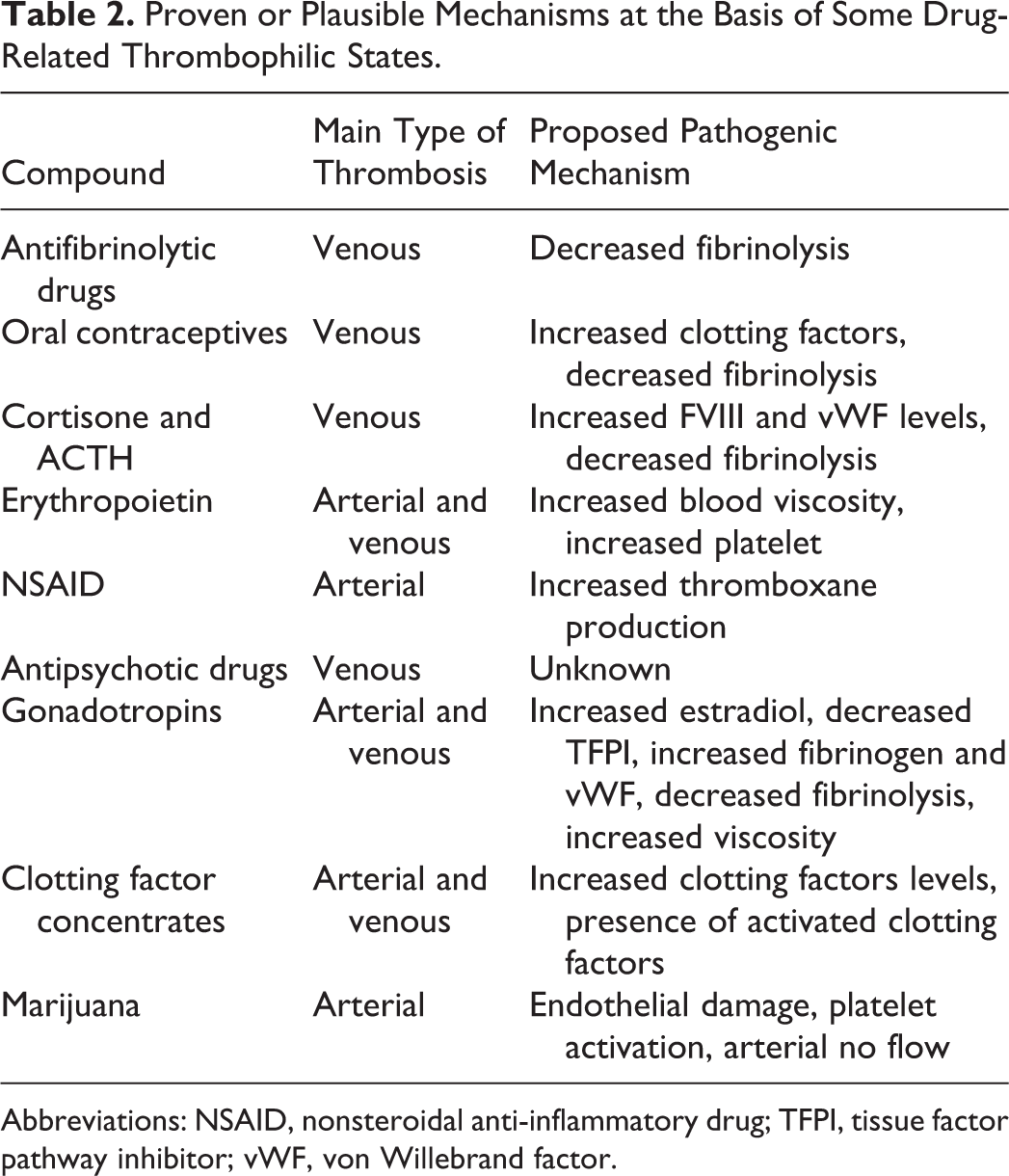
Abbreviations: NSAID, nonsteroidal anti-inflammatory drug; TFPI, tissue factor pathway inhibitor; vWF, von Willebrand factor.
It is likely that future studies may allow a classification of the mechanisms underlying the thrombotic capacity of all these medications. In the meantime, careful individual evaluation of the single patient or series of patients is essential. For example, the exclusion of congenital thrombophilia in patients, especially elderly ones, who are supposed to enter prolonged or therapeutic cycles with cortisone, gonadotropins, anabolic agents, IGs, and so on, is indicated both on clinical grounds (family and personal history) and should the family or the personal history justify it on the basis of laboratory test (antithrombin, protein C, protein S assays, etc).
Many other drugs have been exceptionally or occasionally associated with thrombotic events in a given patient (metformin, ticlopidine, clopidogrel, etc). However, the overall evaluation of these sporadic observations does not seem, at least at the present time, to warrant their inclusion among the thrombophilic drugs. 3
It is expected that the use of these drugs and similar compounds will increase due to their medical and nonmedical use, but also to the present day, immediate gratification-obsessed society we live in. Taking into account the possible concomitant presence in a user of these drugs of a congenital hypercoagulable state and, more frequently, of an acquired thrombophilic state, it is plausible that the future of Western society will show a trend toward thrombosis. The last demonstration of this is supplied by the recent surge in marijuana consumption due to legalization or excessive tolerance. 106 –109 It is likely that after the lung cancer and arterial disease epidemic related to tobacco consumption we have witnessed in the 1950s and 1960s, we will be about to face another epidemic of vascular, pulmonary, and nervous systems diseases due to marijuana use and abuse. The potential contributory effect of drugs to this trend represents a new interesting field of research. A careful selection of patients, drugs, and dosages of same could reduce the human suffering and the sanitary burden represented by thrombotic events.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported in part by the Associazione Emofilia ed altre Coagulopatie delle Tre Venezie.