
Abstract
The increased risk of cardiovascular and cerebrovascular events in patients with migraine remains unexplained. Prothrombotic states are thought to contribute to this increased risk. The present study aimed to compare the prevalence of prothrombotic states in patients with migraine and headache-free controls. We conducted a case–control study to screen for prothrombotic states protein C, protein S (PS), antithrombin III, factor V Leiden, lupus anticoagulant, anticardiolipin, and anti-β2-glycoprotein 1 antibodies in 101 consecutive patients with migraine and 148 controls. An underlying prothrombotic state was encountered in 11.8% of the patients with migraine, PS deficiency being the most common (4.0%). There was no significant difference in the prevalence of prothrombotic states in patients with migraine compared to controls. Traditional prothrombotic states do not seem to have a higher prevalence in patients with migraine compared to controls.
Introduction
Migraine is a syndrome of recurrent headache often associated with varying combinations of visual or sensorimotor aura and autonomic symptoms. It is usually a benign illness in most individuals. 1 However, several studies have noted an increased risk of cardiovascular and cerebrovascular ischemic events in patients with migraine. 2 –9 Recent data indicate that this risk is highest among women who experience migraine with aura. 10 –12 Several putative mechanisms have been considered to explain the increased risk of ischemic events in these patients. These include an increased prevalence of vascular risk factors among patients with migraine causing earlier atherosclerosis, 13 selective cerebral vasospasm, 14 endothelial dysfunction, 15 coexisting patent foramen ovale, 16 autoimmune phenomena, or presence of a prothrombotic state due to genetically transmitted coagulation abnormalities. Studies relating to prothrombotic states have so far revealed conflicting and inconclusive data. 17 –22 Being genetically transmitted, significant geographical variation is likely to exist in the representation of prothrombotic states in various populations. The present study aimed to evaluate the prevalence of prothrombotic states among patients with migraine in North India and compare it to headache-free controls.
Materials and Methods
A total of 101 patients with migraine attending the Neurology clinic of Post Graduate Institute of Medical Education and Research (PGIMER), a tertiary care hospital in North West India, were recruited (Figure 1). A total of 148 age- and sex-matched controls were included from healthy volunteers recruited at the Department of Hematology. The tests were performed at the Department of Hematology, PGIMER. Migraine was diagnosed as per the International Headache Society International Classification of Headache Disorders 2 criteria. 23 Patients with liver disease, diabetes, hypertension, connective tissue disorders, on oral or parenteral anticoagulation, those taking oral contraceptive pills, those with history of cerebrovascular accident, myocardial infarction or venous thrombosis in the recent past (3 months), current smokers, and pregnant women were excluded.
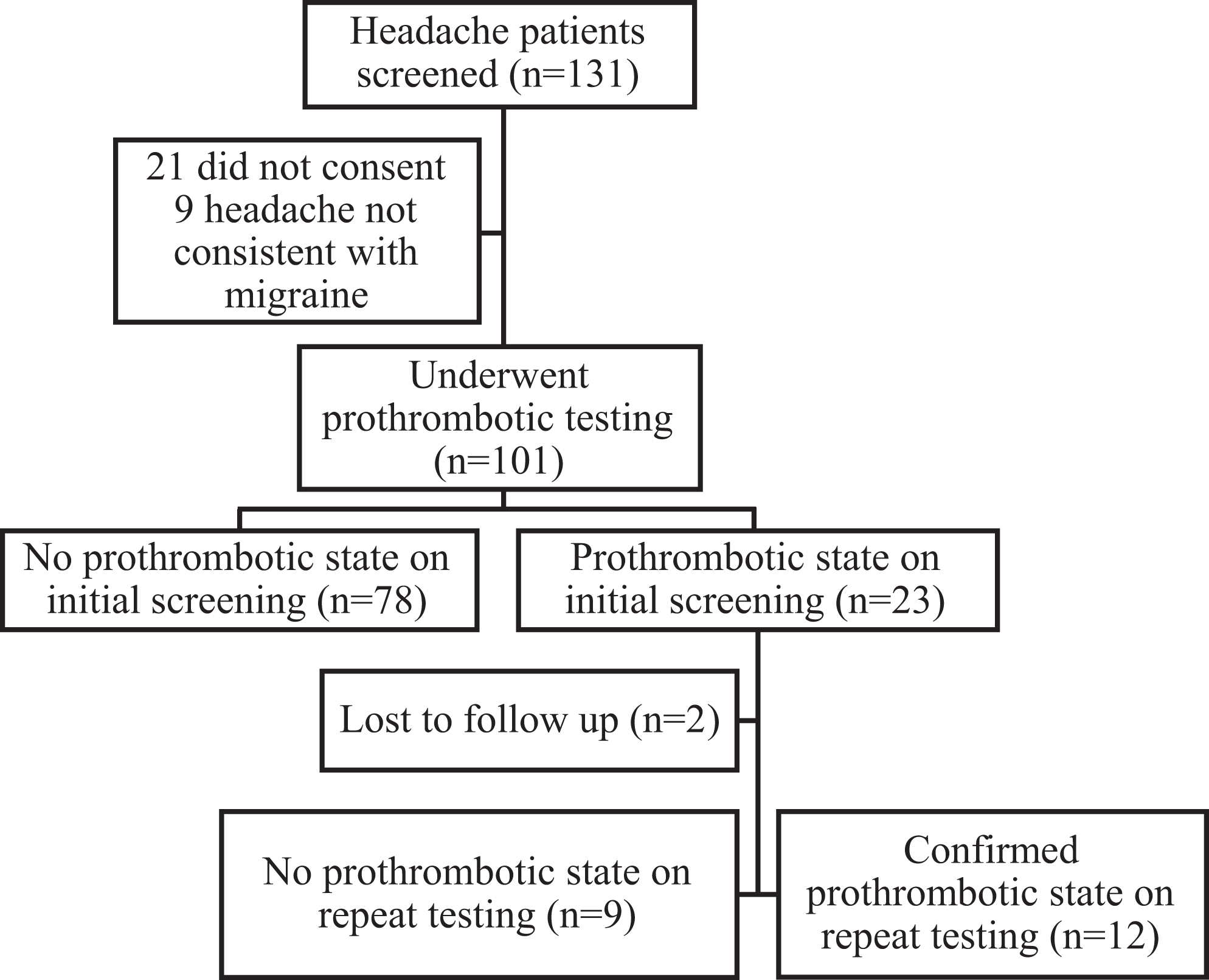
Patient flow diagram.
Institutional ethical clearance was obtained, and informed consent was taken from all patients. Clinical history, physical examination, and relevant investigations were done to rule out secondary causes of headache and establish the diagnosis of migraine as required. Atraumatic blood sample was drawn by venipuncture from the antecubital vein and aliquoted as follows: 5 mL in liquid EDTA for DNA study of factor V Leiden (FVL), 2 aliquots of 2.7 mL in 3.2% trisodium citrate for coagulation assays, and 1 mL in plain vial for serum for the anticardiolipin (ACL) antibody and anti-β2-glycoprotein 1 (anti-β2-GPI) assay.
After performing a clotting screen with prothrombin time, activated partial thromboplastin time, and fibrinogen assay, aliquots of the citrated samples were used for functional protein C (PC) level and protein S (PS) levels using clot-based Staclot PC and Staclot PS kits (Diagnostica Stago, France), respectively, on the STA COMPACT coagulation analyzer with the manufacturer’s instructions. Quantitative determination of antithrombin III (ATIII) level in plasma was done by synthetic chromogenic substrate method using the STA-Stachrom ATIII kit on the same analyzer. All abnormal tests were repeated on a fresh sample. Lupus anticoagulant (LA) was detected by 2 tests: Dilute Russell’s Viper Venom Time (using Dade Behring/Siemens LA Screen [LA1]/and Confirm [LA2] kits) and in house Kaolin clotting time. The IgG and IgM isotypes of ACL antibodies and anti-β2-GPI antibodies were assayed using commercial kits (Orgentec GmBh, Germany). ACL IgG >10 GPLU/mL and IgM>7 MPLU/mL were taken as positive, and for anti-β2-GPI antibodies values of IgG or IgM isotypes >5 units/mL were considered positive. Positive results for LA, ACL, and antibody tests were repeated after 12 weeks, and only those with stable positivity were considered to have a prothrombotic state. Polymerase chain reaction-restriction fragment length polymorphism for FVL was carried out as per the protocol of Bertina. 24 The tests for PC, PS, ATIII, LA, ACL antibody, and anti-β2-GPI antibody are all registered in an international quality assessment scheme (United Kingdom National External Quality Assessment Scheme) with frequent assessments. The reference ranges for deficiencies of PC, PS, and ATIII have already been established for the North Indian population in our laboratory using samples from 130 healthy volunteers (PC: 63%-123%, PS: 67%-143% [males], 55%-123% [females], ATIII: 80%-120%).
Statistical analysis was carried out using SPSS (version 15.0 for Windows; SPSS Inc, Chicago, Illinois). Considering the prevalence of various prothrombotic states in our population (1.0%-8.7%) and assuming the prevalence in patients with migraine to be similar to the previously published data, 21 we calculated that a sample size of 80 patients and 120 controls would be required to determine a significant difference in proportions with power of 80% and α = .05. Comparisons were made using Mann Whitney and chi-square tests. All statistical tests were 2-sided and performed at a significance level of α = .05.
Results
Mean age of the study population was 35.5 (15-60) years. Mean duration of migraine was 7.8 (0.25-30) years, and the mean frequency of attacks was 10.06 (5-24) per month. In all, 29 (28.7%) patients satisfied the criteria for migraine with aura, and the rest had migraine without aura. There were no significant differences in the baseline characteristics of age, sex, duration of illness, and frequency of attacks among the groups having migraine with or without aura and controls (Table 1). Among patients with migraine having aura, a significant proportion (93.1%) reported visual aura (P < .001), while the rest had sensorimotor premonitory symptoms.
Baseline Characteristics of Patients with migraine and Controls.

Abbreviations: MOA, migraine without aura; MA, migraine with aura.
In this study, 4 patients had clinical and radiological evidence of prior cerebrovascular accidents (3 ischemic events and 1 intracranial bleed). There was no statistically significant correlation between cerebrovascular accidents and presence of an aura (P = .576; Table 2). None among them had any of the prothrombotic states tested for. No other thrombotic events or cardiovascular disease were encountered. In all, 6.9% reported a family history of thrombotic events.
Cerebrovascular Accidents in Patients With Migraine.
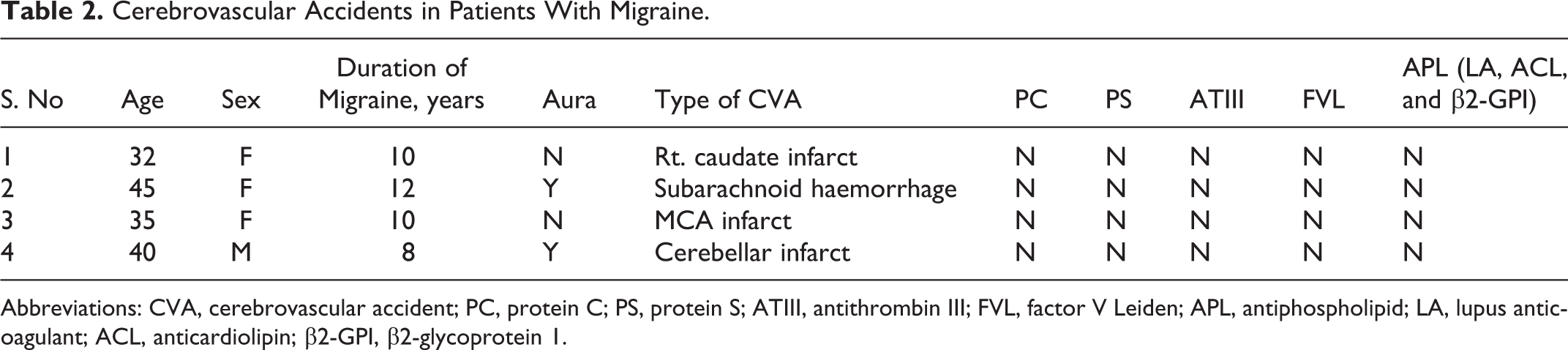
Abbreviations: CVA, cerebrovascular accident; PC, protein C; PS, protein S; ATIII, antithrombin III; FVL, factor V Leiden; APL, antiphospholipid; LA, lupus anticoagulant; ACL, anticardiolipin; β2-GPI, β2-glycoprotein 1.
Four (3.96%) individuals were found to be PS deficient; all had migraine without aura. One (0.99%) individual was deficient in ATIII. None among the study patients were deficient in PC. Two (1.98%) individuals were heterozygous for the FVL mutation . Three (2.97%) individuals were positive for ACL IgM antibodies on initial screening, but on repeat testing after 12 weeks, all of them had ACL IgM levels within normal limits. Three (2.97%) individuals had elevated ACL IgG antibodies, and on repeat testing at 12 weeks, 2 of them had persistently elevated ACL IgG, whereas the third individual was lost to follow-up. There was no statistically significant difference among the groups with or without migraine in the distribution of ACL IgM (P = .554) or ACL IgG (P = .553). Nine individuals had anti-β2-GPI IgM antibodies above the cutoff on initial screening; however in 7 of them, the values returned to normal on repeat testing at 12 weeks. Three individuals had anti-β2-GPI IgG antibodies above the cutoff value, and on repeat testing, 2 (1.98%) of them had persistently elevated anti-β2-GPI IgG. Two individuals with stable positivity for ACL antibodies were the same as those with positivity for β2-GPI antibodies, thus conforming to the biochemical criteria for highly probable antiphospholipid syndrome (APS). 25 However, the clinical criteria of recurrent pregnancy losses/thrombosis for APS were not met in either of these individuals. Test for LA was negative among all. Other than combined ACL and anti-β2-GPI antibody positivity, none of the patients had more than 1 prothrombotic state simultaneously. The overall prevalence of any procoagulant abnormality in our study population was 11.8%. Thrombocytopenia (platelet count < 1.5 × 109/L) was detected during screening in 7.7% of the individuals, and none of them had any of the other prothrombotic states tested for.
There was no statistically significant difference in the prevalence of PC, PS, and ATIII deficiency, FVL mutation, LA, ACL antibodies, and anti-β2-GPI antibodies between patients with migraine and controls (Table 3). Only ACL antibody (ACL IgG) had a higher prevalence among patients with migraine; however, this was not statistically significant (P = .651).
Prothrombotic States in Migraine and the General Population.
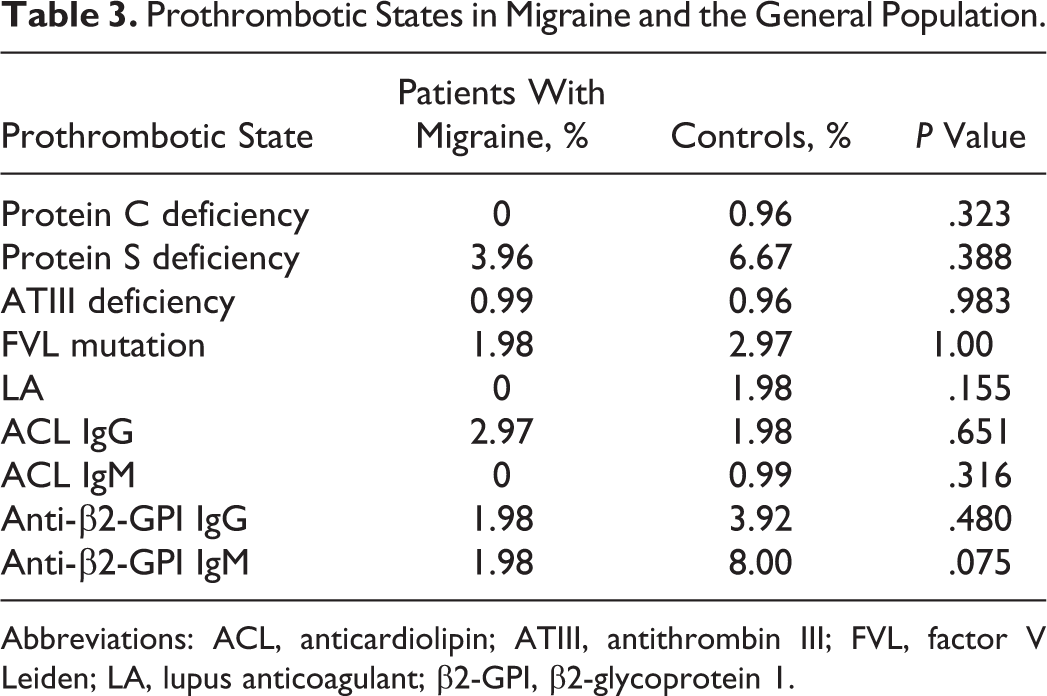
Abbreviations: ACL, anticardiolipin; ATIII, antithrombin III; FVL, factor V Leiden; LA, lupus anticoagulant; β2-GPI, β2-glycoprotein 1.
Discussion
The prothrombotic state is a propensity for blood to coagulate more easily than normal. A number of factors may contribute to this condition. Deficiency of natural inhibitors of coagulation—PC, PS, and ATIII; persistence of certain antibodies, that is, LA, ACL, and anti-β2-GPI antibodies, genetic mutations rendering activated coagulation factors resistant to inactivation (FVL mutation), and increase in coagulant factors (prothrombin gene mutation G20210A) are some of the well-characterized prothrombotic risk factors. Individuals with migraine having these factors may be placed at added risk of adverse cerebrovascular events. To the best of our knowledge, there has been no previous literature on procoagulant states in migraine from the Indian subcontinent, and we screened 101 patients with migraine to establish the prevalence.
In this study, 12 (11.8%) individuals had evidence of a prothrombotic state, the commonest being PS deficiency and positivity for ACL antibodies. None among the study population had PC deficiency or LA. Our results are comparable to other published data that showed no significant difference in the prevalence of FVL, PS, PC, and antiphospholipid (APL) antibodies in patients with migraine 17,18,20,22 (Table 4).
Studies on Prothrombotic States in Migraine.
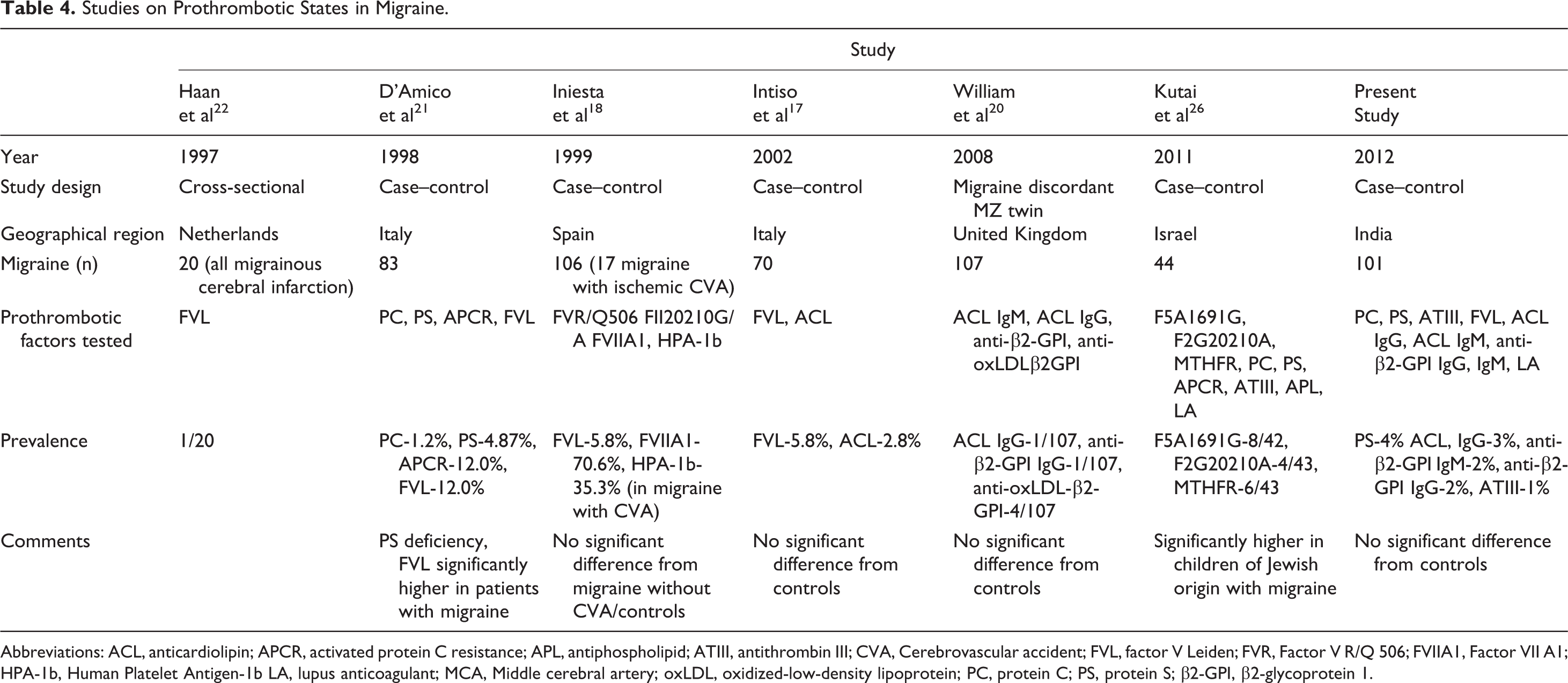
Abbreviations: ACL, anticardiolipin; APCR, activated protein C resistance; APL, antiphospholipid; ATIII, antithrombin III; CVA, Cerebrovascular accident; FVL, factor V Leiden; FVR, Factor V R/Q 506; FVIIA1, Factor VII A1; HPA-1b, Human Platelet Antigen-1b LA, lupus anticoagulant; MCA, Middle cerebral artery; oxLDL, oxidized-low-density lipoprotein; PC, protein C; PS, protein S; β2-GPI, β2-glycoprotein 1.
Although studies have reported a link between the migraine and the prothrombin gene mutation FII G20210A, 26 we did not include this factor in our test panel. The prothrombotic risk factors, especially FVL, have a geographic/ethnic distribution, being relatively uncommon in the Oriental races. The absence of the prothrombin gene G20210A mutation has been reported previously from our center, 27 and presently most centers in this region do not include this test in the thrombophilia screen.
The prevalence of FVL mutation in our study was 1.9% without any significant difference in comparison with controls. This in sharp contrast to an earlier study that reported a high prevalence of FVL up to 12% in patients with migraine compared to controls. 21 Various other studies have shown a prevalence of 5.7% to 6.1% for FVL in patients with migraine; however, these were similar to the prevalence rates in their general population or controls. 22,28 These findings may be attributed to genetic heterogenity in the distribution of procoagulant states in various ethnic groups. Recent data from Israel showing a significant variation in the distribution of FVL among children belonging to 2 ethnic groups in the same cohort lend support to this hypothesis. 26
Persistently elevated IgM antibodies to neither ACL nor β2-GPI were found among the study group. Although the prevalence of ACL IgG was higher than that of the controls, this finding was not statistically significant. Higher incidence of APL antibodies has been reported among patients with connective tissue disease and migraine compared to those with other headache types. 19 A twin study involving migraine discordant monozygotic twins that utilized self-assessment questionnaires failed to detect any increase in the incidence of APL among individuals with migraine. 20 Our data also support these findings that APL antibodies do not seem to be significantly elevated in patients with migraine compared to controls.
Two individuals in the study population had stable positivity for both ACL and anti-β2-GPI IgG, but no clinical features to suggest the APS. According to the recent consensus, these individuals fit into the biochemical criteria for highly probable APS, but neither met clinical criteria for the same. 25 The current recommendation is that asymptomatic APL-positive patients such as these do not need anticoagulation. However, they should be counseled regarding thrombosis and traditional risk factors such as smoking, oral contraception, and pregnancy. 29 Patients with isolated single-test positivity (among LA, ACL, and β2-GPI) are at very low risk of developing clinically significant APS. We had 3 individuals with ACL IgM positivity and 7 with anti-β2-GPI IgM positivity who later reverted to negative on repeated testing at 12 weeks. Such unstable positivity is well known for all the APL antibodies and is not considered to be of clinical significance. According to the current recommendations, such individuals with isolated single-test positivity are at very low risk of developing clinically significant APS and hence unlikely to benefit from repeated follow-up testing.
We encountered 4 patients with clinicoradiological evidence of prior cerebrovascular accident, none of whom had any of the prothrombotic states tested for. Recent data have shown that migraine with aura is independently associated with hypercoagulable states in young patients with ischemic stroke. 30 Our data do not reflect this, probably due to the small number of patients with ischemic events. The relatively small sample size also limited further analysis of each prothrombotic state according to migraine subtype.
Conclusion
The present study reveals that the prevalence of prothrombotic states in migraine is not significantly different from the controls. None of the patients with migraine having ischemic events included in this study had an underlying prothrombotic state to account for their ischemic event. Although limited by the rarity of prothrombotic states and small sample size, these results indicate that prothrombotic states are unlikely to contribute significantly to the vascular morbidity in patients with migraine. Screening patients with migraine who have no prior history of an ischemic event for prothrombotic states thus seem to be a cost ineffective and unproductive approach in our population. Mechanisms such as endothelial dysfunction and cerebral vasospasm need to be analyzed with greater vigour before we can successfully answer the question of why thrombotic events occur with greater frequency in an otherwise benign illness of young individuals like migraine.
Footnotes
Acknowledgments
The technical assistance by Mr Joseph, Mr S Bose, and Mr Harikishen is gratefully acknowledged.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.