
Abstract
Background:
Distal deep venous thrombosis (DVT) accounts for approximately half of all the cases of lower limb thrombosis. The impact and management of this condition is still controversial. This study aims to evaluate the incidence of pulmonary embolism (PE) in patients with distal DVT in comparison to proximal DVT and evaluate the correlation between DVT and PE extension.
Methods:
100 patients with acute lower limb DVT diagnosed with whole leg Doppler ultrasound from January 2006 to December 2014 were retrospectively analyzed. Active investigation for PE was carried out in all patients using multislice computed tomography angiography. Classification of DVT and PE was based on the proximal extension of the thrombus.
Results:
The overall incidence of PE in our sample patients was 72%. In the subgroup analysis, incidence of PE was equal in both the proximal and distal DVT groups (77%, p > 0.99). PE was detected in 43% of the patients with isolated calf vein thrombosis (ICVT). No statistical difference was observed between the distribution of lobar, segmental and subsegmental PE in the 3 DVT subgroups (p = 0.665); however, truncular PE was only observed in the proximal DVT group.
Conclusion:
Distal DVT is associated with a high incidence of PE compared to proximal DVT. Distal DVT and ICVT can provoke PE with involvement of proximal vessels in the pulmonary arterial tree, even in asymptomatic patients. Our study arises discussion in the controversial debate regarding the need for routine anticoagulation in distal DVT.
Introduction
Venous thromboembolism (VTE) is a prevalent and potentially fatal condition that affects over 900 000 in the United States and over 1 million people in Europe annually. 1,2 Pulmonary embolism (PE) is the most feared complication of deep venous thrombosis (DVT) with a case fatality rate of approximately 15%, exceeding the rate reported for myocardial infarction. 3 Distal DVT accounts for approximately half of all the cases of lower limb DVT diagnosed on whole leg compression ultrasonography. 4
Studies have demonstrated that the incidence of silent PE in patients with DVT varies between 32% and 50%. 5 –7 These outcomes are apparently underestimated, since they are based on imaging studies with lower accuracy, such as pulmonary scintigraphy or computed tomography angiography (CTA) scans with thicker slices. Furthermore, the literature discloses a common knowledge that the prevalence of PE in patients with proximal DVT is significantly higher when compared to distal DVT, inferring a lower severity of the latter condition. 8
The management of distal DVT is still controversial. Recent studies and guidelines have suggested that this condition can be treated conservatively without routine need for anticoagulation, however, with weak levels of recommendation. The American College of Chest Physicians (CHEST) guidelines for the first time in 2012 attempted to differentiate treatment strategies for patients with distal and proximal DVT, nonetheless, the decision to administer anticoagulation is based upon the presence of clinical symptoms and physician’s experience without any clear consensus. 9,10 There are currently ongoing trials comparing treatment versus placebo for distal DVT. 11
The aim of this study was to evaluate the incidence of PE in patients with distal DVT in comparison to proximal DVT, based on the use of modern gold-standard CTA scans, and to evaluate the correlation between DVT and PE extension. As a secondary outcome, we aim to analyze how the laboratorial biomarkers C-reactive protein (CRP),
Methods
This retrospective transverse study was carried out in accordance with the Ethics Committee of our institution. Due to the observational and retrospective nature of the study, informed consent terms were dismissed. Medical records of 120 consecutive patients followed by our vascular surgery team, with the diagnosis of acute DVT of the lower limb between January 2006 and December 2014 were retrospectively analyzed.
We included patients who reported to the emergency department of our institution with an acute onset of inferior limb DVT and were submitted to chest CTA for active investigation of PE upon admission. All included patients reported leg pain and/or edema and had no initial complain of respiratory symptoms. Twenty patients who were not submitted to CTA due to renal impairment (creatinine levels over 1.5 mg/dL), pregnancy, and/or hypersensitivity to iodinated contrast media were excluded from our analysis. All the patients were immediately treated with full-dose enoxaparin (1 mg/kg twice daily) for at least 48 hours prior to the introduction of an oral anticoagulant therapy.
Relevant epidemiologic characteristics including age, sex, body mass index (BMI), and comorbidities were registered. We considered as risk factors patients older than 75 years, BMI ≥ 25, positive thrombophilia testing, recent trauma or surgical intervention (within the last 4 weeks), use of oral contraceptives, recent travel (over 8 hours in the last 4 weeks), and active malignancy.
Certified radiologists in our institution performed the color Doppler ultrasound examinations. The CTA scans were performed in 16- or 64-row multislice scanners (Toshiba Medical Systems, Tokyo, Japan) with reconstructed axial images of 1 mm thickness. Intravenous iodinated contrast (iobitridol 350 mg/mL, Henetix®, France) was used in all cases with doses ranging from 90 to 120 mL, administered by a power injector with an approximate rate of 4.0 mL/s.
Information regarding the site of affected vein, laterality of thrombus, and extent of DVT and PE was recorded. We reviewed blood samples collected from the study patients upon admission and analyzed red and white cell tests (including RDW), basic biochemistry, CRP using chemiluminescence assay (reference range 0-3.0 mg/L), and
Deep Venous Thrombosis and PE Classification
Patients with DVT were classified into 3 subgroups: proximal, distal, or isolated calf thrombosis (ICVT) according to the proximal location of the thrombus. Clots affecting popliteal, femoral, or iliac veins were classified as proximal, clots affecting axial leg veins (tibial or fibular veins) were classified as distal, whereas isolated clots in soleus or gastrocnemius veins were defined as ICVT. To evaluate clot burden, we counted the number of individual venous segments involved (ie, the sum of the number of veins with clots as reported in the Doppler ultrasound).
Pulmonary embolism was classified into 4 categories based on the anatomical site of the pulmonary arterial tree affected by the clot. 12 Clots involving the main pulmonary artery or its bifurcation were classified as truncular, and clots affecting the second, third, and fourth bifurcations of the pulmonary artery were classified as lobar, segmental, or subsegmental, respectively.
Control Group
A control group including patients admitted in the emergency department of the same institution, in the same time period, followed by other vascular surgery teams was studied. We used the hospital’s official database and surveyed the cases of DVT using the International Classification of Diseases, Tenth Revision (ICD-10) coding system. The codes analyzed were I82.8 (embolism and thrombosis of other specified veins) and I82.9 (embolism and thrombosis of unspecified vein). Cases of thrombosis in sites other than inferior limbs, cases of isolated superficial thrombophlebitis, and cases of PE with no detected DVT were excluded from the control group analysis. Comparisons between baseline epidemiological characteristics of the patients included in our internal validation sample and our study group were performed.
Statistical Analysis
Qualitative variables were described using absolute frequencies and percentages. Quantitative variables were described using medians and interquartile intervals, since normal distribution could not be verified using the Shapiro-Wilk test.
Variables of interest were tested for the presence of PE using χ2 or Fisher test in the case of categorical variables. In the case of continuous variables, Mann-Whitney U test or Kruskal-Wallis test was used.
The association between RDW, CRP, and
The association between RDW, CRP, and
Results
General Characteristics of the Study Population and Comparison With the Control Group
The clinical baseline characteristics of the study patients in the 3 DVT subgroups are outlined in Table 1. Gender, age, BMI, and laterality of DVT were similar in the 3 groups. We observed bilateral DVT involvement in 3 cases of the proximal group.
Baseline Characteristics of Patients With DVT.
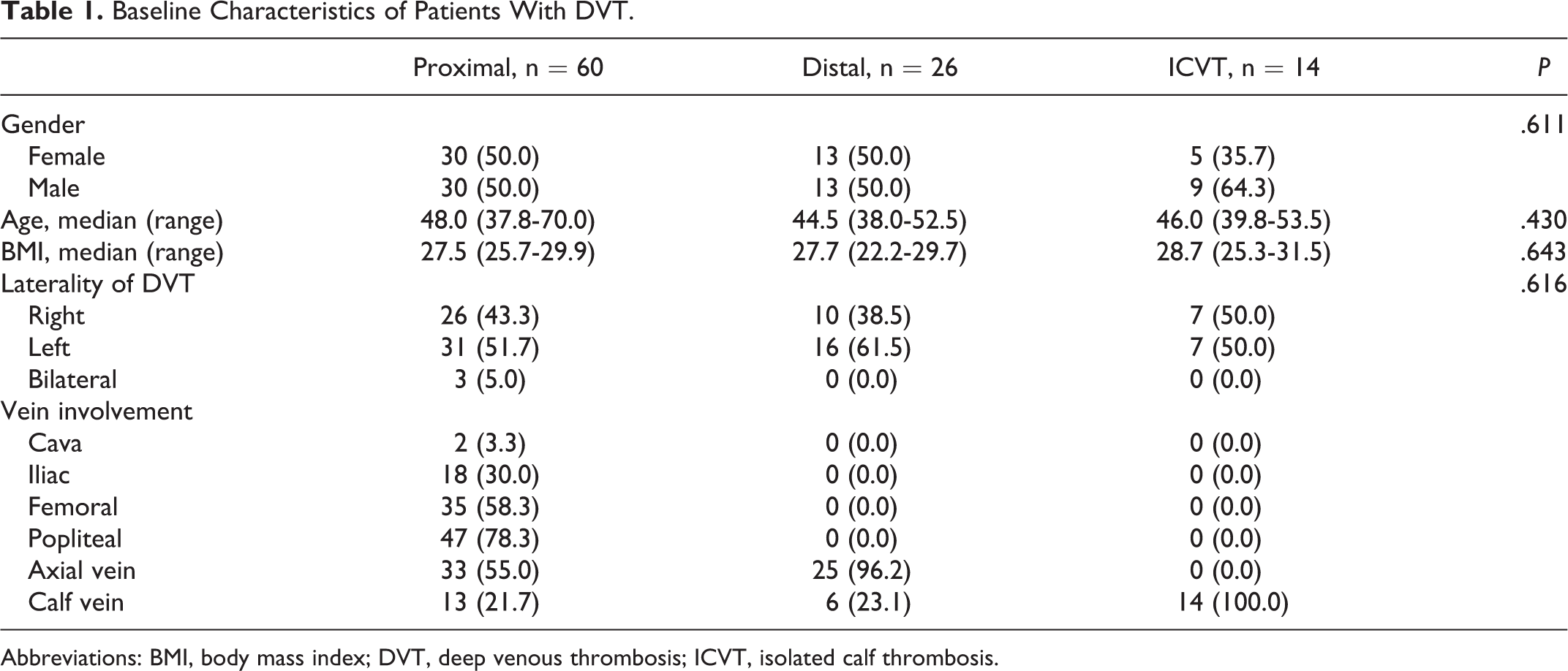
Abbreviations: BMI, body mass index; DVT, deep venous thrombosis; ICVT, isolated calf thrombosis.
Table 2 outlines the comparison between demographic and clinical characteristics of the study and control groups. Age was significantly higher in the control group. Among the studied risk factors, recent surgery was significantly more prevalent in the protocol group (P = .011).
Comparative Analysis Between Baseline Characteristics of Protocol and Control Group.
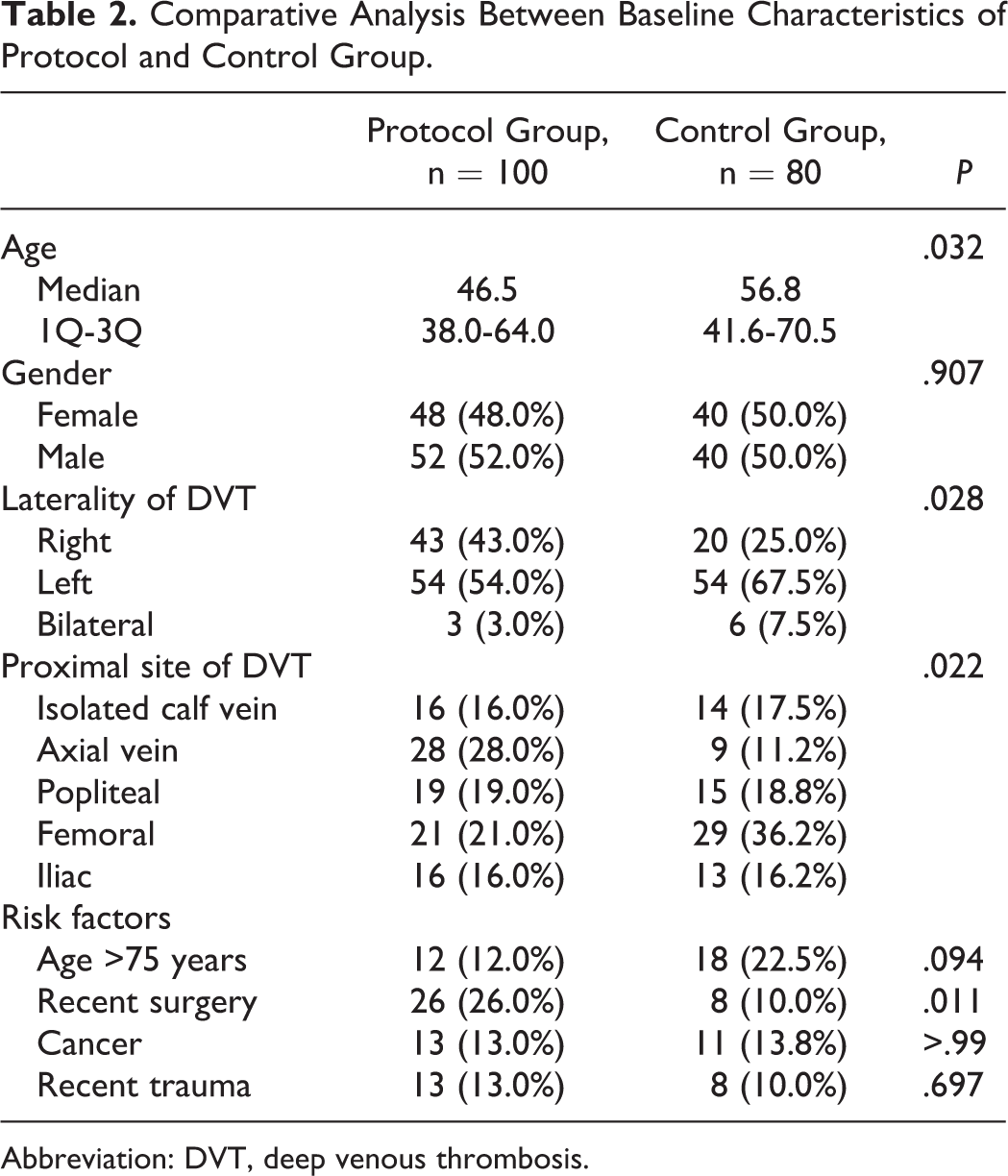
Abbreviation: DVT, deep venous thrombosis.
Risk Factor Analysis According to the Severity of the Thromboembolic Event
The association between risk factors and the severity of the thromboembolic event, defined by occurrence of PE and extension of DVT, is presented in Table 3. Recent travel and recent surgical intervention were the only variables significantly associated with the occurrence of distal DVT. None of the other studied risk factors were predictive of the severity of the thromboembolic event.
Risk Factor Analysis According to the Presence of PE and Classification of DVT (Proximal or Distal).
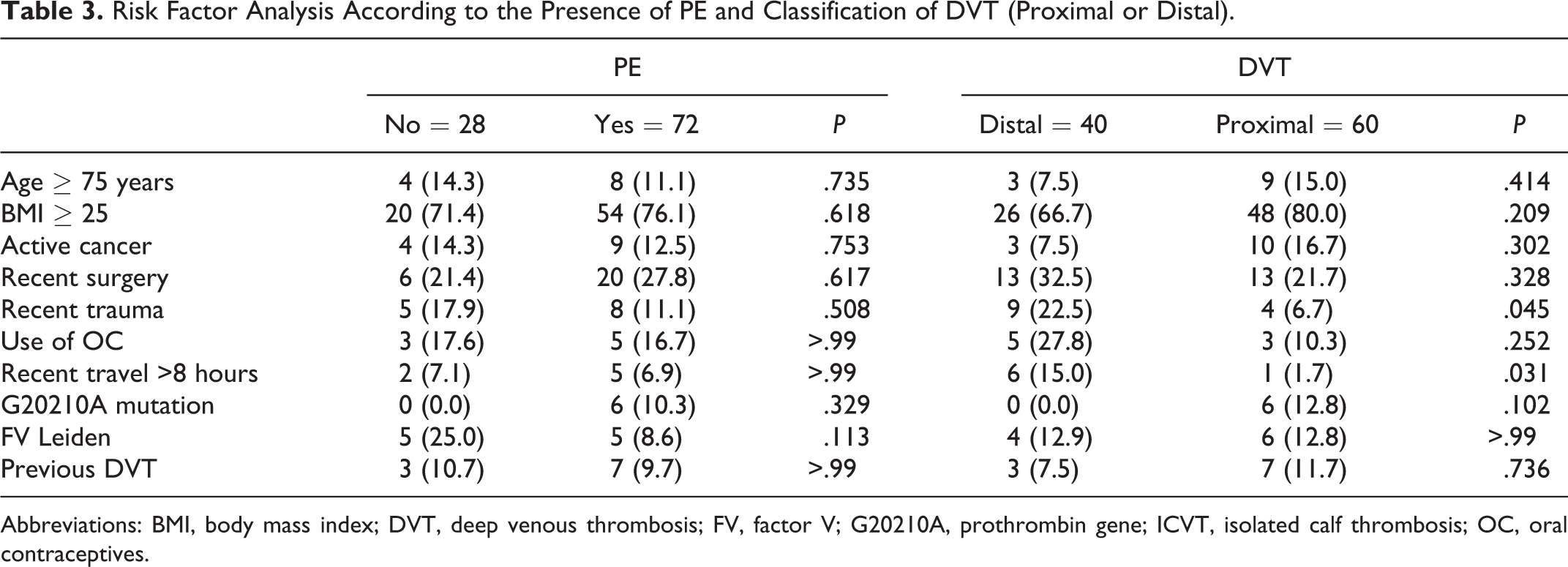
Abbreviations: BMI, body mass index; DVT, deep venous thrombosis; FV, factor V; G20210A, prothrombin gene; ICVT, isolated calf thrombosis; OC, oral contraceptives.
Incidence and Severity of Asymptomatic PE in the DVT Groups
The overall incidence of PE in our sample patients was 72%. In the subgroup analysis, incidence of PE was equal in both the proximal and the distal DVT groups (77%, P > .99), as shown in Figure 1. Pulmonary embolism was detected in 43% of the patients with ICVT. No statistical difference was observed between the distribution of lobar, segmental, and subsegmental PE in the 3 DVT subgroups (P = .665), however, truncular PE was only observed in the proximal DVT group (Figure 2).
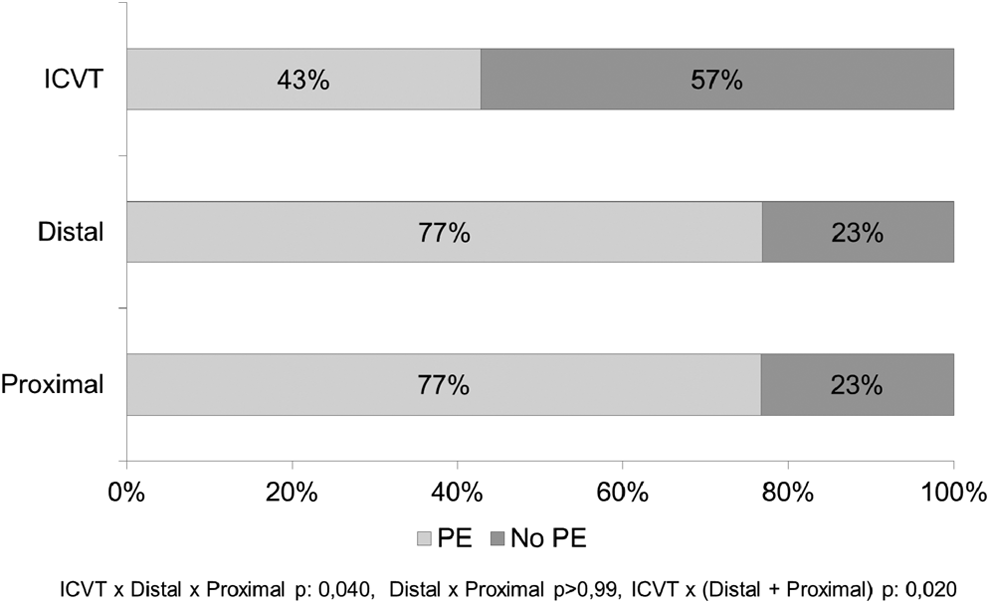
Incidence of pulmonary embolism (PE) in the deep venous thrombosis (DVT) groups.
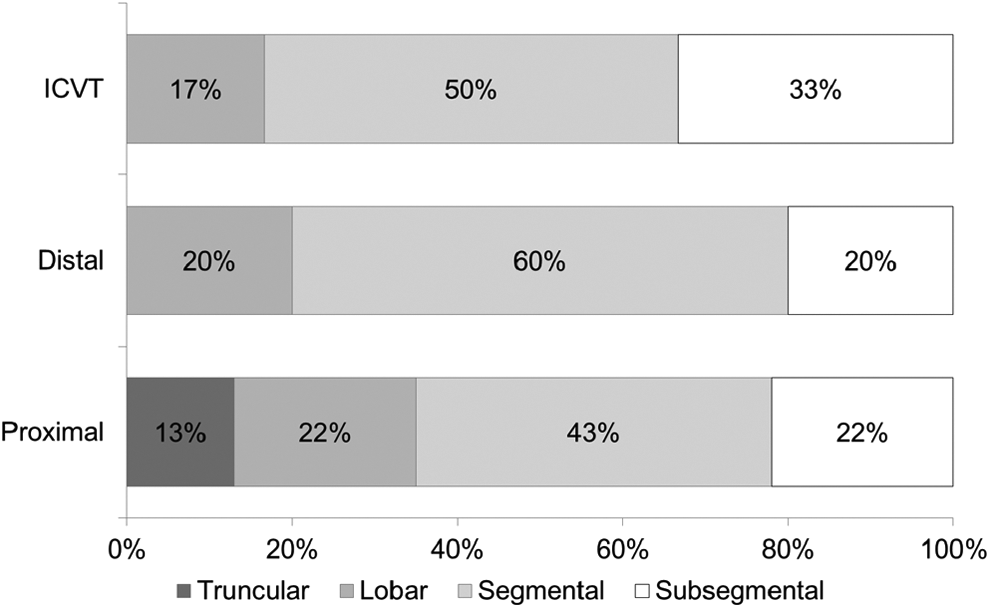
Proximal site of pulmonary embolism (PE) thrombus location in the deep venous thrombosis (DVT) groups.
Association Between Laboratorial Biomarkers (CRP, RDW, and d -Dimer) and Clot Burden
Only
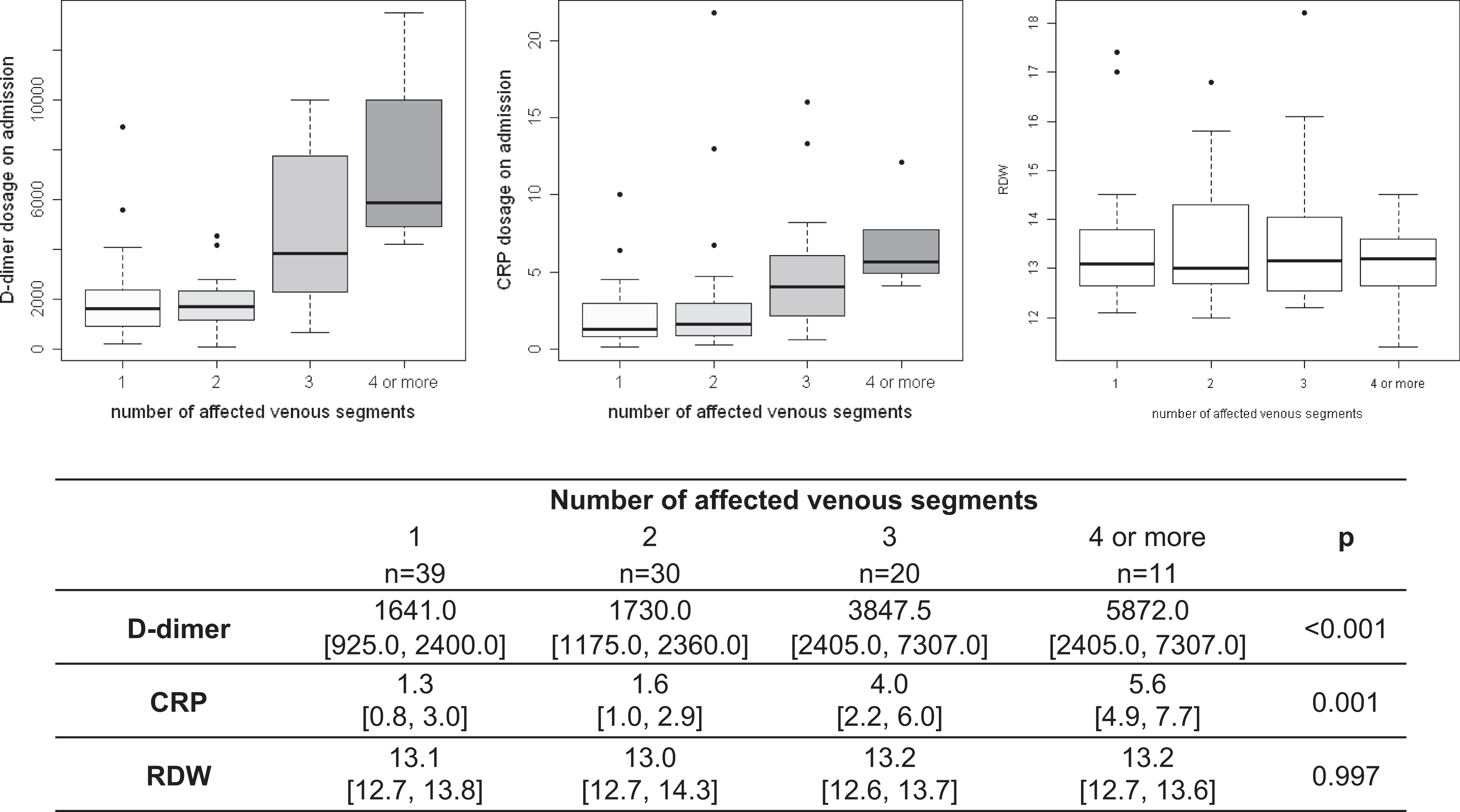
Association between number of affected venous segments laboratorial biomarkers.
Predictive Value of d -Dimer for PE
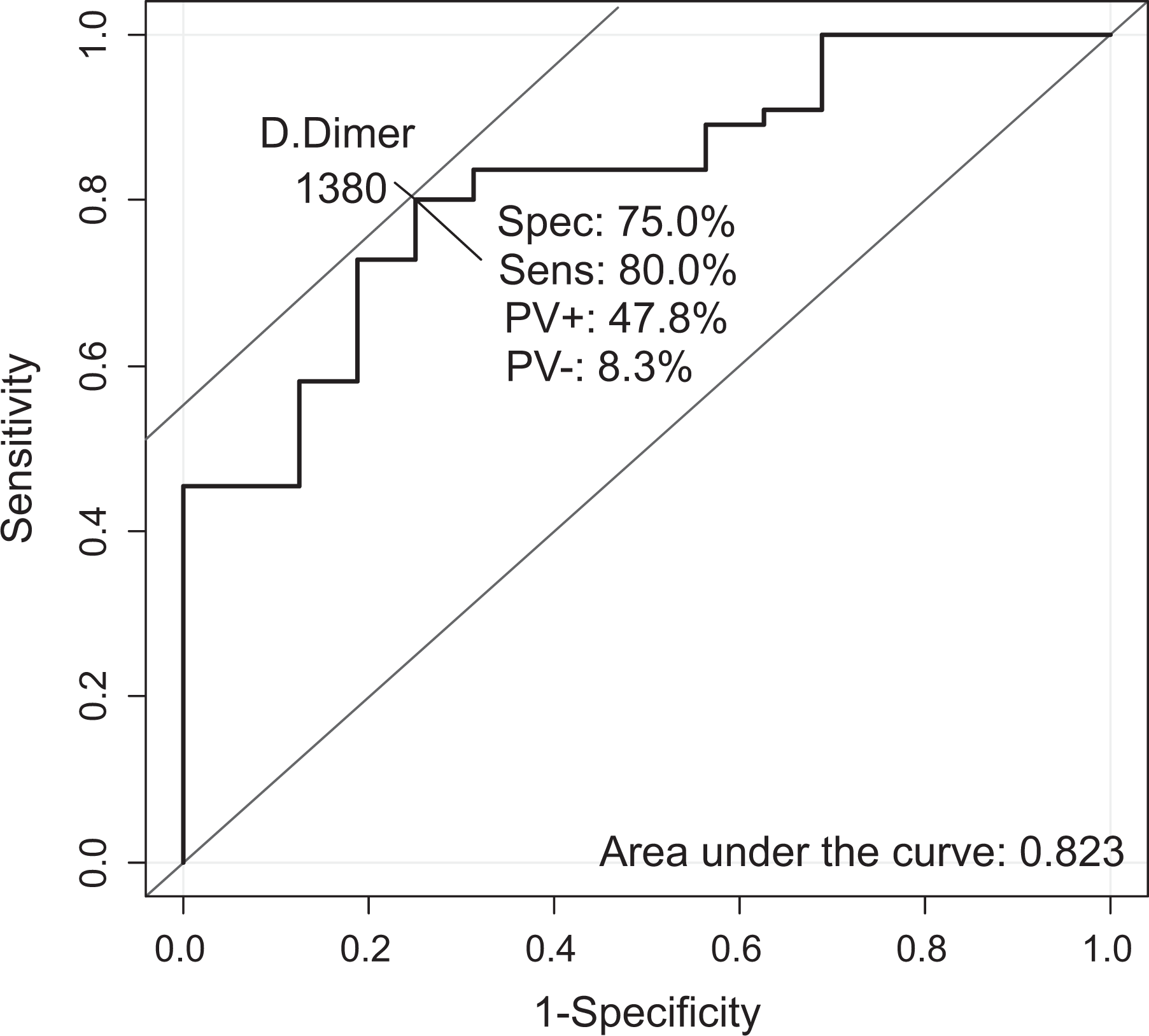
Receiver–operating characteristic (ROC) curve for
Discussion
The observed overall incidence of 72% of asymptomatic PE in patients with acute DVT is higher than any data shown in the current literature. The equal incidence of PE in patients with proximal and distal DVT with a similar distribution of lobar and segmental clots is yet unpublished information. Our incidence of PE in patients with ICVT is similar to what is expected for proximal DVT according to recent papers.
The general concept that distal DVT is less likely to lead to PE has been well accepted in clinical practice and supported by recent publications. 14 Recent thrombosis guidelines do not recommend routine anticoagulation for distal DVT. 9 Our findings demonstrating an equal risk of PE among patients with proximal and distal DVT (77%, P > .99) may influence change in the clinical management of these patients. These results strongly encourage a need for standardizing mandatory use of anticoagulation in all cases of distal DVT.
The high incidence of PE in patients with ICVT (43%) shows that findings from a systematic review published in September 2014 describing a 13.1% prevalence of asymptomatic PE in patients with this condition are underestimated. 15 Despite the asymptomatic nature of incidental PE, treatment is mandatory due to the increased risk of symptomatic and fatal recurrence. 16 Watchful waiting can no longer be an option for patients with distal DVT, considering an almost 80% risk of associated PE. Furthermore, these undiagnosed and untreated patients are in risk of developing chronic thromboembolic pulmonary hypertension (CTPH), a condition that is frequently recognized in a late phase when prognosis is poor. 17
Although truncular PE was only observed in the proximal DVT group, lobar and segmental PE similarly affected the 3 DVT subgroups. This alerts to the higher potential severity of PE in patients with proximal DVT but does not minimize the concern with PE in distal or ICVT. Despite the lower clot burden in distal DVT, proximal sites of the pulmonary arterial tree (ie, lobar arteries) are affected in around 20% of the cases.
The lower median age observed in our sample patients together with the similarity of relevant baseline characteristics between our sample and control groups was important to further validate our outcomes. These findings ensure that the high incidence of PE is not likely to be attributed to a selection bias of critically ill patients. The higher incidence of recent surgery observed in our protocol group emphasizes the need for adequate prophylactic measures in surgical patients. Special attention should be given to orthopedic interventions that were highly prevalent in our sample.
None of the studied risk factors were predictive of PE occurrence. Recent surgery consisted of 77% of orthopedic interventions and was significantly associated with distal DVT. This association corroborates with the results of a recent observational study including 50 000 patients, which demonstrated a higher prevalence of distal DVT (60% distal vs 33% proximal) in orthopedic surgical patients. 18 Recent travel was also significantly associated with distal DVT as also demonstrated in a 2006 literature review of the quantitative risk of VTE following air travel. 19
Despite the enthusiasm of previous studies in demonstrating a significant association between RDW and PE and severity of DVT, 20,21 this outcome was not reproduced in our research. Red cell distribution width did not show association with incidence of PE, location of proximal DVT thrombus, or DVT clot load. The observation that RDW does not show predictive value for the diagnosis of DVT has also been demonstrated in a study that analyzed patients undergoing total joint arthroplasty. 20
Our results showed that both CRP and
Limitations
Our study was based on a retrospective analysis of electronic medical records, therefore, information loss is inevitable, despite the strict documentation protocol used by our group. Information regarding risk factors such as tobacco use was lacking in most of the analyzed medical records and was therefore excluded from our analysis.
Overexposure to radiation and contrast is a point of concern in our study. Despite the lack of conclusive data, this exposure may have implications in the renal function of predisposed patients and increased risk for certain types of radiation-induced cancers. However, modern CTA scanners require increasingly lower radiation doses,
26
and a recent systematic review and meta-analysis have reported that intravenous, as opposed to intra-arterial, contrast infusion is not associated with an increase in contrast-induced nephropathy.
27
Furthermore, this concern is what motivated our
Our findings of asymptomatic PE may represent an overdiagnosis of a condition with debatable clinical relevance, since favorable outcomes with complete thrombus recanalization are expected after full anticoagulation for DVT treatment. On the other hand, assuming the current recommendations in light of our results, almost half of the patients with ICVT will not be adequately treated for PE, leaving them at risk of sudden death or future pulmonary implications such as the development of CTPH. 17
Conclusion
Distal DVT is associated with a high incidence of PE comparable to proximal DVT, around 77%. Distal DVT and ICVT can provoke PE with involvement of proximal vessels in the pulmonary arterial tree, including lobar and segmental branches even in asymptomatic patients. Our study arises discussion in the controversial debate regarding the need for routine anticoagulation in distal DVT.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.