
Abstract
Background:
Total joint arthroplasty (TJA) patients are mostly of advanced age and with comorbidities such as increased body mass index (BMI) and impaired glucose tolerance. These factors and type of surgery may affect the fibrinolytic system.
Aim:
To investigate the effect of age, sex, BMI, type of surgery, and tranexamic acid (TXA) treatment on the fibrinolytic system in TJA patients.
Methods:
Ninety-nine patients undergoing TJA (32 total hip arthroplasty [THA] and 67 total knee arthroplasty [TKA]) were included in this study. Blood samples were drawn at preoperative clinic appointments and on postoperative day 1. Antigenic levels of
Results:
Preoperative
Conclusion:
These results confirm that advanced age and elevated BMI positively contribute to fibrinolytic dysregulation in TJA patients, whereas TXA seems to decrease the fibrinolytic activity.
Introduction
The average patient population undergoing major lower extremity total joint arthroplasty (TJA) is of increased age and body mass index (BMI) with multiple medical comorbidities, requiring the use of multiple medications, all of which, including type of surgery, have the potential to alter the perioperative fibrinolytic status in these patients. Total hip arthroplasty (THA) is obviously performed without a tourniquet, whereas a total knee arthroplasty (TKA) can be formed with or without tourniquet application. A tourniquet provides reduced quantity of blood in the operative field for the surgeon 1,2 and decreases intraoperative blood loss. 3 However, tourniquet application has been shown to cause severe pressure and tissue ischemia, which can result in metabolic and cellular changes to the underlying tissues in addition to vascular injury. These changes may contribute to the increased thrombotic and fibrinolytic activity in peripheral blood that has been found when a tourniquet is used. 2,4,5 Increased fibrinolytic activity in TKA and THA patients has also been associated with increased bleeding amount. 6,7
One of the main components of the fibrinolytic system is plasminogen activator inhibitor 1 (PAI-1), which is synthesized from endothelium, liver, and adipose tissue. 8 The PAI-1 inhibits tissue plasminogen activator (tPA), thereby inhibiting its activator effect on inactive plasminogen to active plasmin, which degrades fibrin. Activated plasmin is also inactivated by α2-antiplasmin. Low level of antiplasmin or high level of plasmin–antiplasmin (PAP) complex indicates recent fibrinolytic activity. 9 High PAI-1 levels have been found to be correlated with high BMI 10 and high glucose levels. 11
The tranexamic acid (TXA) is an antifibrinolytic agent, which is a synthetic derivative of the amino acid lysine. The TXA shows antifibrinolytic effect by the reversible blockade of lysine-binding sites on plasminogen molecules and thereby inhibiting the interaction of plasminogen with fibrin. The plasminogen molecule is activated by plasminogen activators after binding to fibrin. The TXA interferes with this binding and results in inhibition of plasminogen activation. 12 Antifibrinolytic treatments prevent the breakdown of a developed thrombus and decrease the bleeding amount. The TXA treatment is used for this purpose in orthopedic surgeries and has been shown to reduce blood loss and the need for blood transfusions in TKA. 13
The aim of this study is to monitor the effect of age, gender, BMI, type of arthroplasty surgery, and TXA treatment on the fibrinolytic system parameters in TJA patients.
Methods
Upon approval of the institutional review board, 99 consecutive patients undergoing TJA (hip or knee) were recruited at the Loyola University Medical Center. Patients with a history of atrial fibrillation with stroke, thromboembolic event, cardiac or other vascular stents, or color blindness were excluded, as they were unable to receive TXA preoperatively. Patients of only 1 of the surgeons were eligible for TXA because, at the time of the study, the other 2 surgeons did not administer TXA as part of their protocol. One gram of intravenous TXA was given in the preoperative holding area to 25 patients. Seventy-four patients did not receive TXA.
Preoperative day 1 and postoperative day 1 blood samples of the 99 arthroplasty patients who underwent TKA (67) or THA (32) were obtained.
Blood samples were drawn in tubes containing 3.2% (0.109 mol/L) sodium citrate. Samples were centrifuged for preparation of platelet-poor plasma at 3000 rpm, at room temperature, for 20 minutes. Plasma samples were aliquoted and stored at −80°C until analysis.
All of the TKA surgeries were performed with the use of a tourniquet for at least a portion of the procedure, with 5 of the surgeries using the tourniquet only for cementing and the remainder of the surgeries using the tourniquet from incision until the final components was in place. Postoperatively, patients who had undergone a TKA were placed into a knee immobilizer in full extension but were allowed to range the knee as much as possible while in bed. They were allowed to ambulate immediately with the knee immobilizer on. Patients who underwent THA were not immobilized in any way and were allowed to ambulate immediately following surgery. All patients received warfarin on preoperative day 1, which was continued until postoperative day 30, with a goal international normalized ratio (INR) of 2.0 to 2.5 for anticoagulation.
The antigen levels of PAI-1,
Parameters such as age, sex, BMI, glucose, hemoglobin A1c (HbA1c), and hemoglobin (Hb) g/dL values were collected from the electronic medical record.
Statistical Considerations
The data were analyzed using Stata version 12.0 (Statacorp, College Station, Texas). Percentage changes (PCs) in fibrinolytic marker levels were calculated as (postoperative value − preoperative value) × 100/preoperative value. Associations between age and BMI with
Results
Baseline Characteristics
The study comprised 69 females and 30 males with a mean age of 65.5 ± 10.1 years. Sixty-seven patients underwent TKA, and 32 patients underwent THA. Patient characteristics of the TKA, THA, and combined TJA groups are shown in Table 1.
Characteristics of Patients Undergoing TJA.a
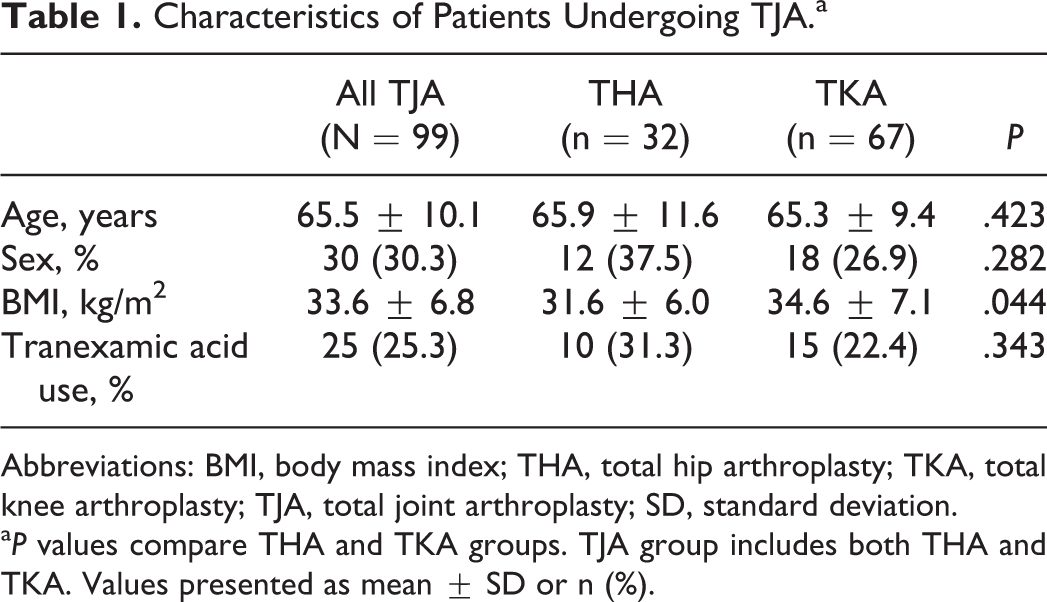
Abbreviations: BMI, body mass index; THA, total hip arthroplasty; TKA, total knee arthroplasty; TJA, total joint arthroplasty; SD, standard deviation.
a P values compare THA and TKA groups. TJA group includes both THA and TKA. Values presented as mean ± SD or n (%).
Effect of Age
Preoperative
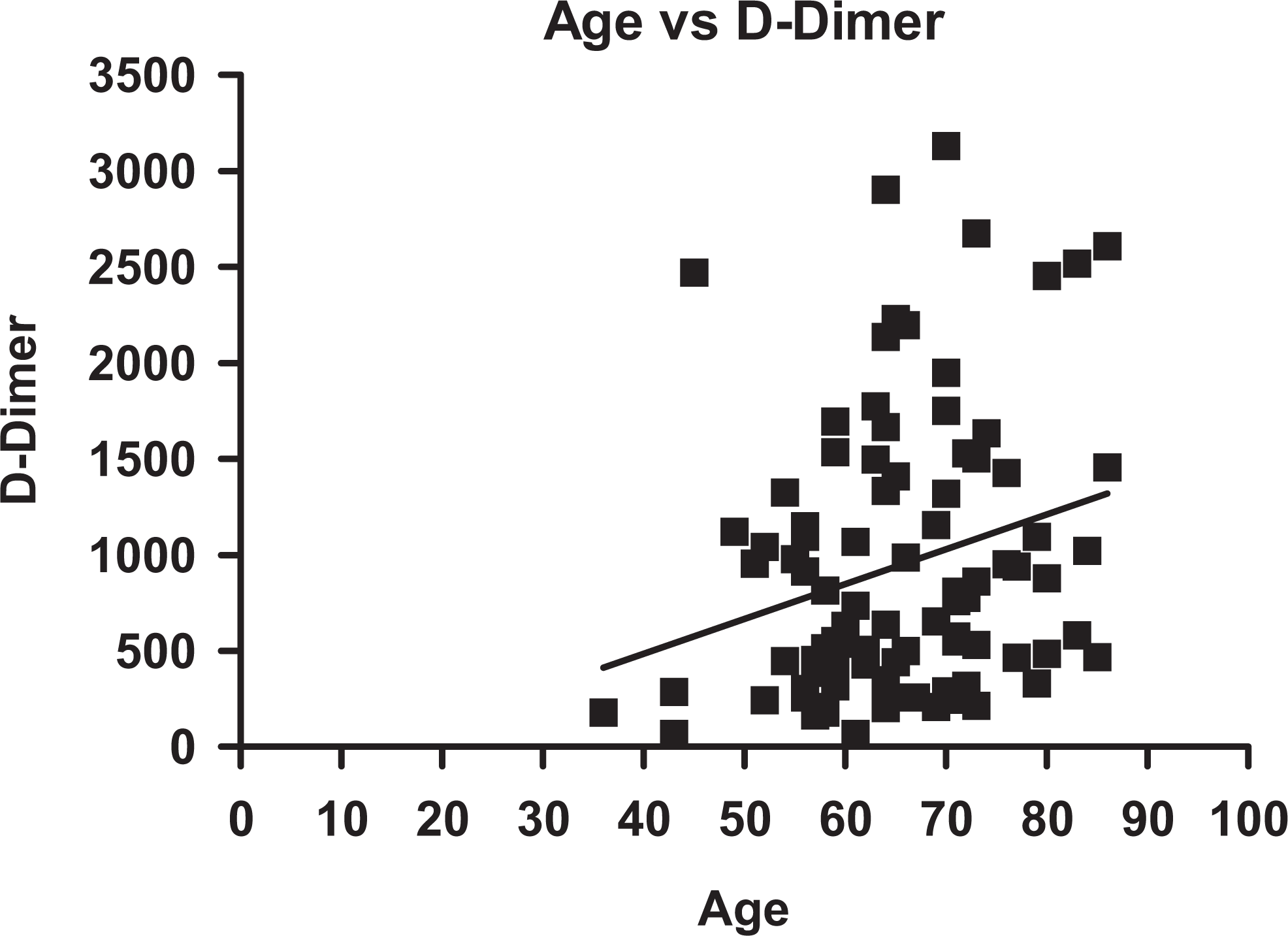
Correlation plot between
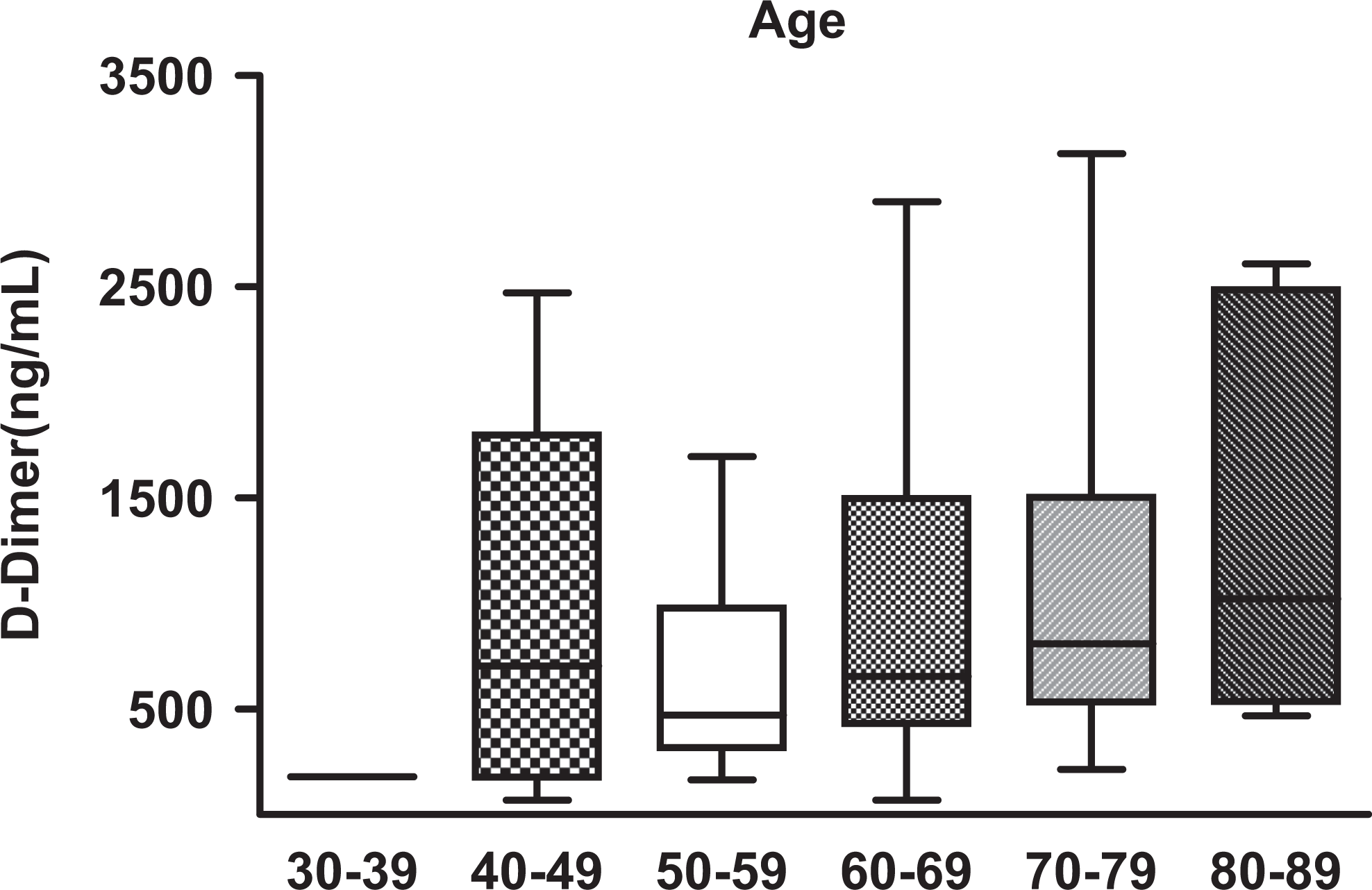
Box plots depicting the
Effect of Sex
No significant differences were observed between female and male sex in relation to
Effect of BMI
A positive correlation was observed between BMI and preoperative tPA levels (r = 0.26, P = .015; Figure 3), but no association was noted between BMI and
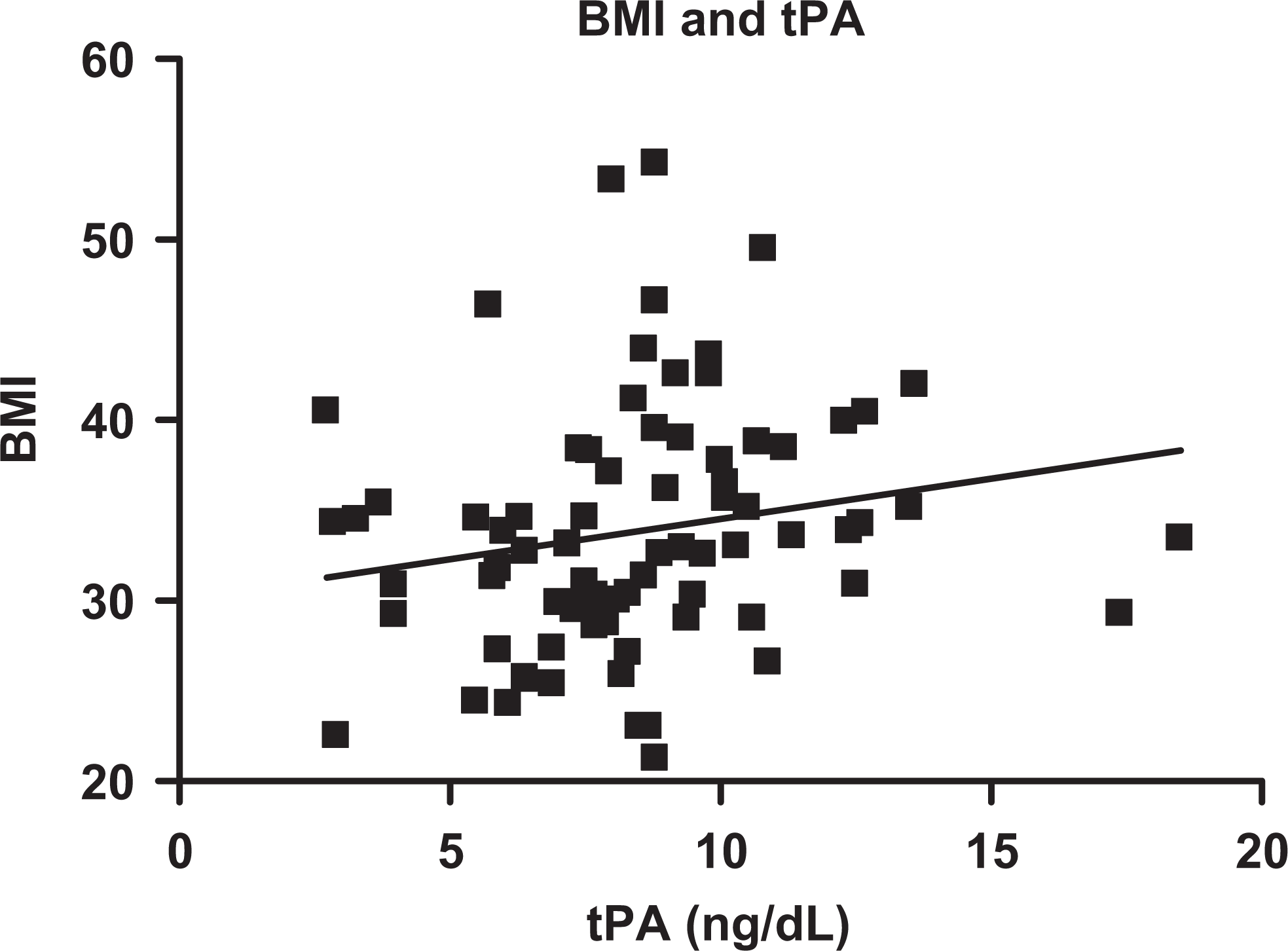
Correlation plot between BMI and tPA. The BMI is positively correlated with the circulating tPA antigen levels (r = 0.26, P = .015). BMI indicates body mass index; tPA, tissue plasminogen activator.
Effect of TXA
There were no significant differences in the postoperative levels of
Fibrinolytic Parameters in Patients Day 1 Postsurgery Treated With and Without TXA.a
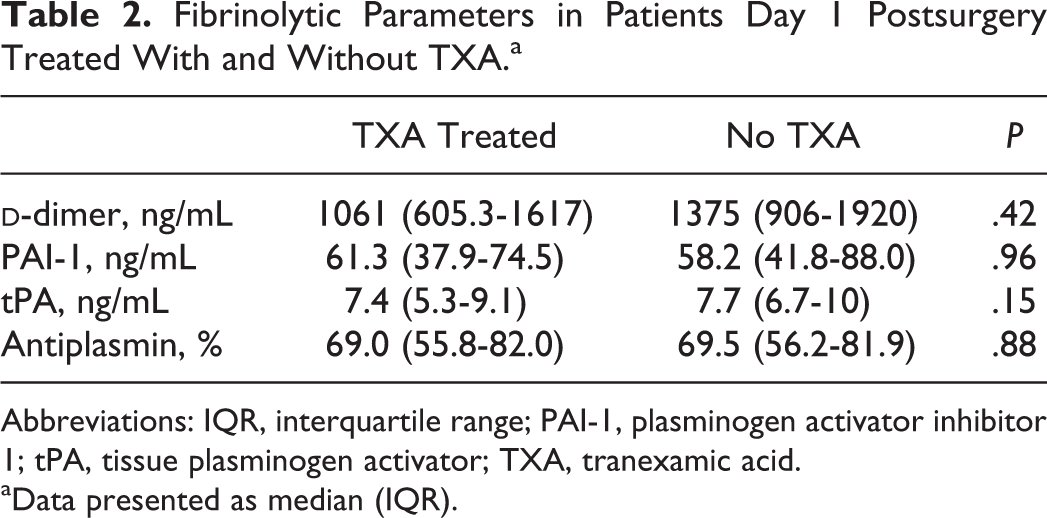
Abbreviations: IQR, interquartile range; PAI-1, plasminogen activator inhibitor 1; tPA, tissue plasminogen activator; TXA, tranexamic acid.
aData presented as median (IQR).
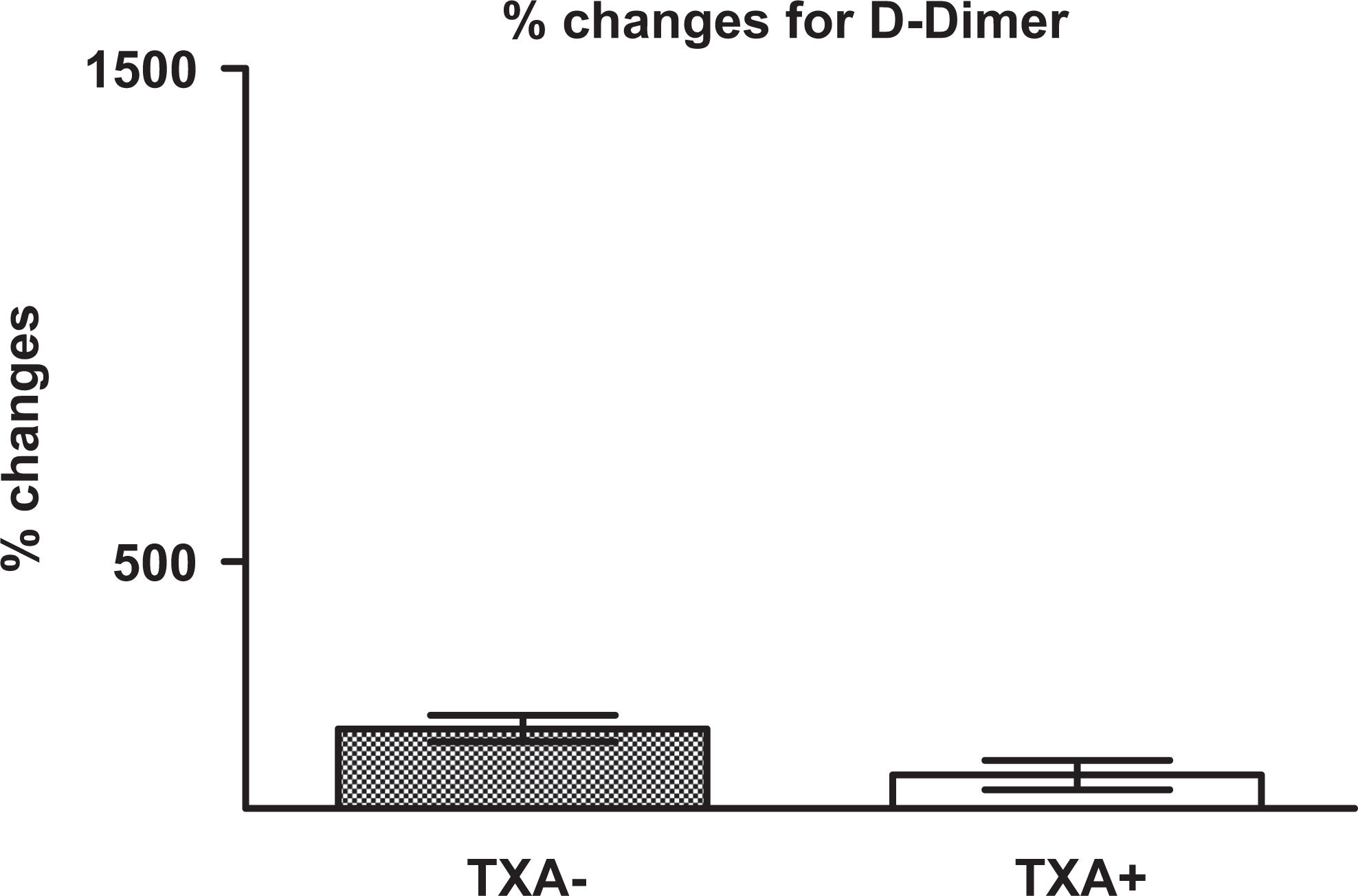
Box plots demonstrating the percentage changes in
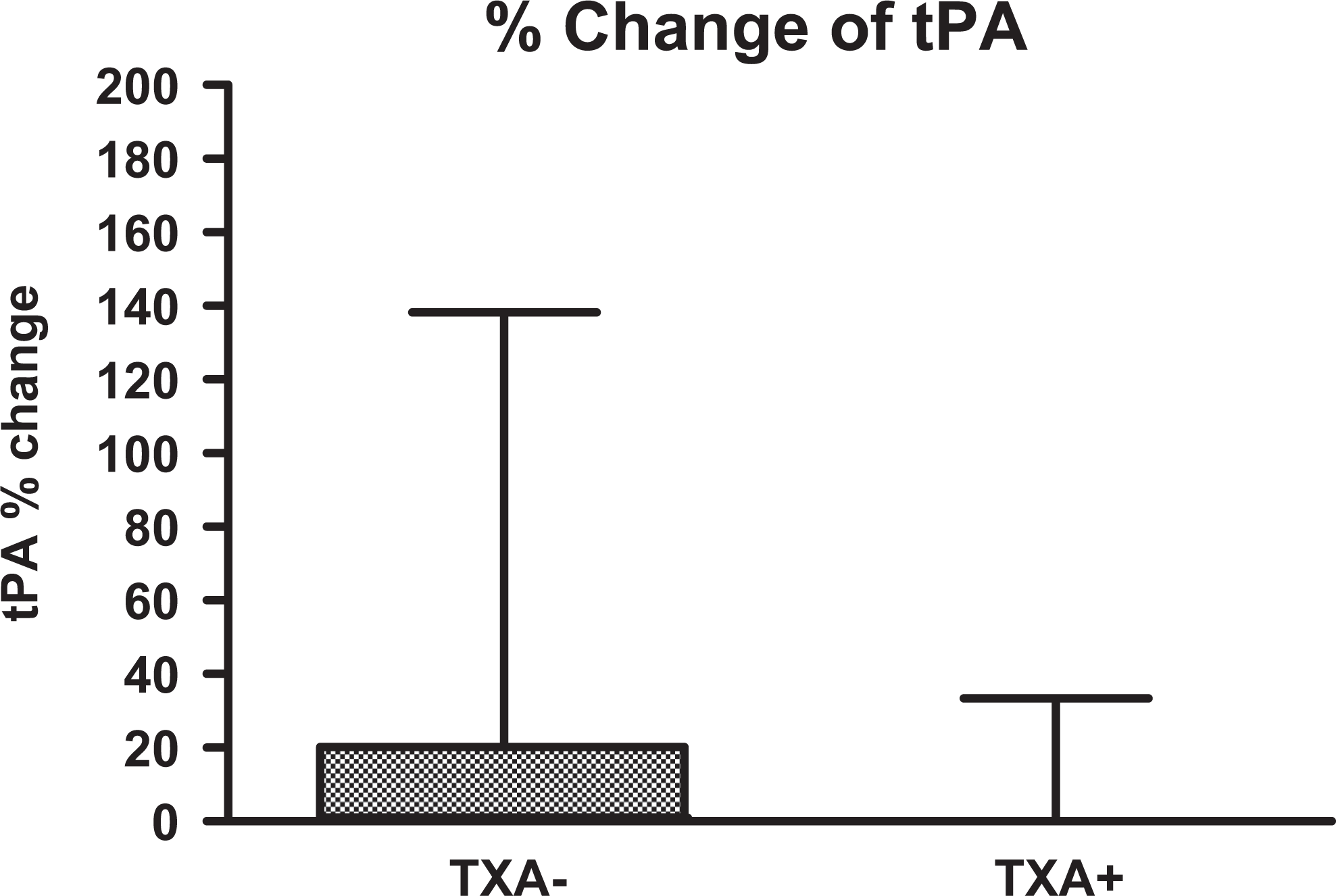
Box plots demonstrating the percentage changes in tPA levels in patients treated (TXA+) and untreated (TXA−) with TXA. tPA indicates tissue plasminogen activator; TXA, tranexamic acid.
Percentage Change in Fibrinolytic Parameters in Patients Treated With and Without TXA.a
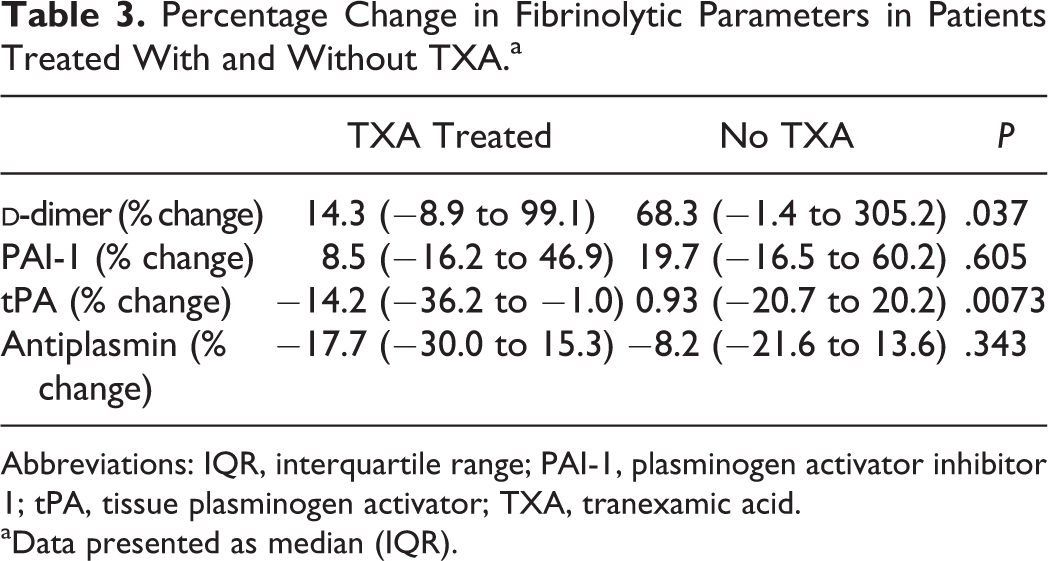
Abbreviations: IQR, interquartile range; PAI-1, plasminogen activator inhibitor 1; tPA, tissue plasminogen activator; TXA, tranexamic acid.
aData presented as median (IQR).
Type of Arthroplasty
Postoperative levels and PC of
Effect of Blood Glucose Levels and HbA1c
As it has already been reported that there is a correlation between PAI-1 and glucose,
11
a potential correlation with preoperative glucose level and PAI-1 (r = 0.194; P = .184) and
Preoperative PAI-1 levels were not shown to be significantly different between patients with normal and high HbA1c level (median [IQR]: 47.04 ng/mL [34.76-72.06 ng/mL] vs 53.79 ng/mL [39.71-66.64 ng/mL], respectively, P = .375).
There was also no difference observed between patients taking Celebrex, a selective COX-2 inhibitor, or not in regard to PAI-1, tPA,
Discussion
The population for this study was mostly comprised of patients of advanced age having high BMI with multiple medical comorbidities. Advanced age was found to correlate with elevated levels of
In the current study, there is no gender-related difference in regard to fibrinolytic markers, which argues against the literature in which antiplasmin and
The main sources of plasma PAI-1 are primarily liver and adipose tissue.
8,10
In this study, PAI-1 levels were not correlated with increased BMI. There was also no correlation between
Previous studies have shown that glucose is one of the biologic substrates that increase PAI-1 values. 11 Results of the current study do not support the triggering effect of glucose on the levels of PAI-1. As there has been an emphasis on better perioperative glucose control and optimization, these random glucose measurements may not be a reliable marker of overall blood glucose regulation. Because of this, HbA1c levels were also used to monitor the effect of glucose on PAI-1 levels. In contrast to the current literature, 11 no correlation was found between blood glucose and PAI-1.
Total joint arthroplasty can lead to large amounts of blood loss. It has been shown that a TKA can lead to a decrease in preoperative hemoglobin values of 3.88 g/dL by postoperative day 3. 12 According to a meta-analysis by Zhang et al, 13 TXA significantly reduces total blood loss by a mean of 486.7 mL in TKA and decreased the proportion of the patients needing a blood transfusion by 37%. The TXA also decreased the number of the packed red blood cell transfusion per patient. Routes of administration of TXA are different in the literature such as intra-articular, 17 intravenous, and oral, 18 with no literature showing one route to be superior to another.
As there is no reliable method to detect exact blood loss during surgery, we preferred to analyze the postoperative hemoglobin values in comparison to preoperative values to analyze blood loss. Blood loss during surgery was not measured directly. Patients’ postoperative hemoglobin changes were not found to be different between the TXA-treated and the nontreated group. Percentage change in hemoglobin values were also not different between the TXA-treated and the nontreated group.
The PCs in tPA and
Blanié et al
19
found increased
Both TKA and THA have been shown to cause an increase in the fibrinolytic markers PAP and
Many arthroplasty patients take nonsteroidal anti-inflammatory drugs (NSAID) for their analgesic and anti-inflammatory effects. The most commonly prescribed NSAID in our patient population was celecoxib. An attempt was made to monitor the effect of celecoxib on the fibrinolytic profile. There were no significant effects of celecoxib noted on the fibrinolytic markers.
Limitations of this Study
A major limitation to this study is that the only patients who received TXA were treated by 1 surgeon and that the administration of TXA was not randomized. It can be assumed that there are no significant differences between surgeons who could alter the fibrinolytic markers, but without randomization of the groups, one cannot be sure. Another limitation is that the levels of PAI-1 and tPA were evaluated with an antigenic method. This can cause insufficient evaluation of these markers during fibrinolysis. Measurement of activity of these 2 markers could give more information and allow for better evaluation of the data.
Conclusion
Our results confirm that age and BMI are essential components for imbalanced/increased fibrinolytic activity in TJA patients preoperatively. Surgeons must be aware of this, and care must be tailored for patients with older age and high BMI in order to decrease perioperative bleeding.
The TXA appears to decrease the fibrinolytic activity in arthroplasty patients and can be considered in order to diminish blood loss during TJA surgeries and potentially help decrease bleeding-related complications and blood transfusion rates. However, if this increased fibrinolytic activity is due to increased thrombin generation as a result of increased age in this patient population, the use of TXA could potentially be counterproductive. Despite the proven safety of TXA in the literature during major lower extremity orthopedic surgery, thrombotic risk with TXA usage should be evaluated in well-designed studies.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.