
Abstract
Background:
Biomarkers of endothelial dysfunction are not recommended for routine laboratory investigation of the outcome prognosis and prediction of the course of sepsis.
Methods:
A total of 60 patients who fulfilled the criteria for diagnosis of sepsis were included in our study. Development of multiorgan dysfunction syndrome (MODS) in the first 48 hours was assessed. Differences between groups of patients with sepsis were assessed by Mann-Whitney U test and by Kruskal-Wallis test. Logistic regression analysis was performed to test the joint effect of different predictors.
Results:
Level of thrombomodulin was significantly higher in group of patients with MODS than without MODS (P = .015). Levels of antithrombin (P = .026) and protein C (P = .035) were significantly lower in patients with MODS. Level of thrombomodulin was the strongest predictor in MODS development in first 48 hours (P = .028).
Conclusion:
The level of thrombomodulin not only was able to distinguish the severity of sepsis but also was a significant predictor of MODS development.
Introduction
Sepsis is one of the most complex challenges in the treatment of critically ill patients, despite implementation of new resuscitating protocols. 1,2 Epidemiological studies bring evidence that coagulation abnormalities in patients with sepsis are in 50% to 70% clinically relevant, and that 35% of the patients with sepsis has disseminated intravascular coagulation (DIC). 3 Changes in the integrity of endothelium are the basis of these severe and mostly fatal complications of sepsis. 4 However, it is not only that inflammation leads to activation of coagulation in sepsis but coagulation also highly affects inflammatory activity, leading to the development of complications such as multiorgan dysfunction syndrome (MODS). 5,6 This extensive cross talk between inflammatory and coagulation systems may be an important factor for organ dysfunction and consequent death. 6
Because of activation of procoagulant pathways during sepsis, natural inhibitory systems, including tissue factor pathway inhibitor, antithrombin, the protein C system, and the fibrinolytic pathway, are balancing this state. Activated protein C acts with its cofactor protein S to prevent coagulation. Thrombomodulin integrates these pathways by binding thrombin to activate protein C and enhance fibrinolysis. 6,7
Thrombomodulin is a membrane glycoprotein expressed on endothelial cells and present in the body in 2 forms, bound to the membrane of endothelial cells and as a soluble or plasmatic form. 8 According to the evidence from literature, it can be used as a marker of endothelial injury. 9 However, only few studies investigated thrombomodulin as a marker of endothelial injury in sepsis. 10
Understanding the significance of the cross talk that occurs between inflammation and coagulation, recent studies have been focusing on development of novel, effective treatments for sepsis. 11,12 However, the significance of biomarkers of coagulation abnormalities and endothelial damage and their implementation in everyday practice is still not accurately defined. 10,13,14 Biomarkers of coagulation and dysfunction of endothelial cells, although noted as important in pathophysiology of sepsis, are not recommended for routine laboratory investigation in the outcome prognosis and prediction of the course of this disease. 15
To date, only few studies have been focusing on markers of coagulation and endothelial injury as a useful tool in prediction and prognosis of outcome and severity of sepsis. Measurement of these markers could contribute to early recognition of MODS development, and more appropriate therapeutic approach could be started earlier.
Our primary objective was to determine whether levels of factors of anticoagulant pathways (protein C, protein S, antithrombin, and thrombomodulin) measured within 24 hours of intensive care unit (ICU) admission are associated with 48 hours MODS development in patients with sepsis.
Materials and Methods
Patients
Data were collected prospectively (and analyzed retrospectively) over 1-year study period. Any patient treated in the Department of Anesthesia and Reanimation of Emergency Center as well as in the Clinic of Infectious Disease of Clinical Center of Vojvodina since June 1, 2012, to June 1, 2013, with a clinical diagnose of sepsis defined by The ACCP/SCCM Consensus Conference Committee American College of Chest Physicians/Society of Critical Care Medicine 1992, revised on SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference 2001, 16,17 was eligible for inclusion.
Patients who were excluded from our study were polytraumatized patients, patients that were in hemorrhagic shock, patients with malignancy, patients with liver failure, pregnant women, patients with cardiac failure, patients with antiphospholipid syndrome, patients who receive anticoagulant therapy, or per oral therapy with vitamin K antagonists (except of patients who receive minimal prophylactic dose of low-molecular-weight heparin like nadroparine 0.3 mL/24 h, from whom blood samples were obtained 12 hours after the application of medicine). Also, patients who have not signed informed consent for the participation in the study or patients with systemic inflammation caused by some other condition except sepsis (burns and pancreatitis) were excluded from the study.
The study was approved by the relevant ethical committee of our institutes, and all participants signed informed consent before enrollment in the study.
Basic laboratory test was performed within the first hour of ICU admission (complete blood count, urea and creatinine level, bilirubin level, and concentration of C reactive protein and procalcitonin). During the first 24 hours of diagnosing sepsis, predictive Acute Physiology and Chronic Health Evaluation II (APACHE II) and Sequential Organ Failure Assessment (SOFA) scores were calculated.
Patients were classified into 4 groups representing different forms of sepsis severity, and development of MODS in the first 48 hours was assessed, with MODS being defined as more than 2 organ dysfunctions since sepsis development according to the already defined criteria. 16,17
To assess the development of complication and also the outcome of the disease, we monitored patients for 28 days from the day of the sepsis diagnosis.
Biomarkers of Endothelial and Coagulation Integrity
After inclusion in the study, in the first 24 hours from onset of sepsis, 5 mL of venous blood was obtained from each patient. Blood samples were anticoagulated with citrate and immediately centrifuged, and plasma samples were then refrigerated at −20°C for 2 weeks.
Laboratory tests were performed in a blind manner, without any knowledge of health condition and development of MODS.
The level of thrombomodulin was measured using R&D enzyme-linked immunosorbent assay thrombomodulin commercial kits (ProMedia doo, Beograd, Serbia). The manufacturer-revised protocol was followed, and values are expressed in ng/mL. Since higher concentrations of plasma thrombomodulin were expected in patients with sepsis than in the healthy population, undiluted stock solution with concentration of 40 000 pg/mL served as the high standard. Minimum detectable dose of the assay ranged from 2.91 to 27 pg/mL.
The levels of protein C activity, antithrombin activity, and free protein S antigen were determined with IL reagents (Instrumentation Laboratory, Milan, Italy) using ACL 9000 coagulometer (Instrumentation Laboratory), and results were given as percentage of normal values.
Statistical Analysis
Data were analyzed using SPSS 20.0 software. Data are expressed as mean ± standard deviation or numbers (%). Since most continuous variables were skewed, nonparametric approaches were used. Differences between variables were assessed by the Mann-Whitney U test and by Kruskal-Wallis test. Categorical variables were compared using chi-square (χ 2 ) test.
To establish the potential for combinations of markers to improve prediction of MODS development in sepsis, we first used correlation (Kendall τ). Logistic regression analysis was performed to test the joint effect of different predictors added to the model. All P values were 2-sided, and statistical significance was set at a value of .05.
Results
Between June 1, 2012, and June 1, 2013, of the total number of patients with sepsis treated in our institutes, only 60 patients fulfilled defined inclusion criteria and were not excluded by exclusion criteria. Among those 60 patients diagnosed with sepsis, 33 were males and 27 were females, 19 to 87 years old. Patients were classified into 4 groups, simple sepsis, severe sepsis, septic shock, and MODS on the admission in ICU. Development and persistence of MODS if patients already had MODS on admission were noted during the first 48 hours of the diagnosis of sepsis according to the already defined criteria. 16,17
Table 1 shows the clinical characteristics of studied patients. There was no significant difference between the groups of patients with sepsis according to the clinical course of sepsis on the admission in age and gender. Of the patients, 28.33% developed MODS in the first 48 hours, and the significant difference was obtained between the 4 groups representing different forms of sepsis severity in MODS development or persistence (P < .05). The overall mortality was 30%, while patients with more severe form of sepsis had higher mortality (P < .05). Statistically significant differences were obtained between groups of patients with sepsis for SOFA score (P < .05), while there was no significant difference between groups for APACHE II score. However, both of these scores were higher in group of patients with severe sepsis than in patients with septic shock on the admission (14.33 ± 8.73 vs 11.54 ± 4.76 for APACHE II and 9.33 ± 6.98 vs 9.09 ± 7.88 for SOFA score). Development or persistence of MODS in the first 48 hours was also significantly different between 4 groups of patients with sepsis (P < .05). Mortality was higher in the group of patients with septic shock than in other groups, and as expected significant difference between the groups was obtained (P < .05). Patients with MODS development in the first 48 hours had significantly higher mortality (P < .05).
Clinical Characteristics of Patients.a
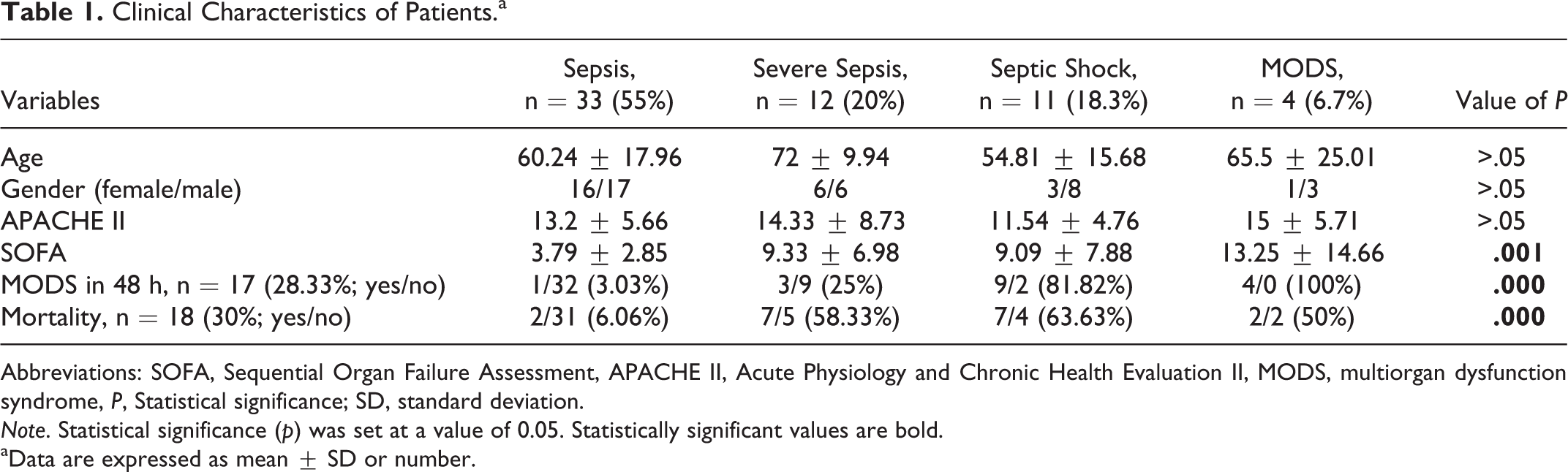
Abbreviations: SOFA, Sequential Organ Failure Assessment, APACHE II, Acute Physiology and Chronic Health Evaluation II, MODS, multiorgan dysfunction syndrome, P, Statistical significance; SD, standard deviation.
Note. Statistical significance (p) was set at a value of 0.05. Statistically significant values are bold.
aData are expressed as mean ± SD or number.
Table 2 shows the levels of natural anticoagulants on day 1 of ICU admission with APACHE II and SOFA scores between studied groups according to MODS development and persistence in the first 48 hours. Concentration of thrombomodulin was significantly higher in group of patients with MODS than without MODS (10.40 ± 4.58 vs 7.6 ± 3.10 ng/ml, P < .05). Concentration of antithrombin and protein C was significantly lower in group of patients with MODS than without MODS (39.13% ± 16.11% vs 52.44% ± 23.20%, P < .05 for antithrombin and 39.85% ± 16.47% vs 62.14% ± 20.33%, P < .05 for protein C). Although the level of protein S was also decreased in the group of patients with MODS in contrast to patients without MODS, statistical significance was not obtained. Our results do not show statistically significant difference between patients with and without the development of MODS in the first 48 hours for APACHE II score, while SOFA score was significantly higher in the group of patients with MODS (10.58 ± 9.75 vs 4.63 ± 3.75, P < .05).
Differences Between Predictive Scores and Anticoagulant Factors Between Groups According to MODS Development and Persistence in the First 48 Hours.a
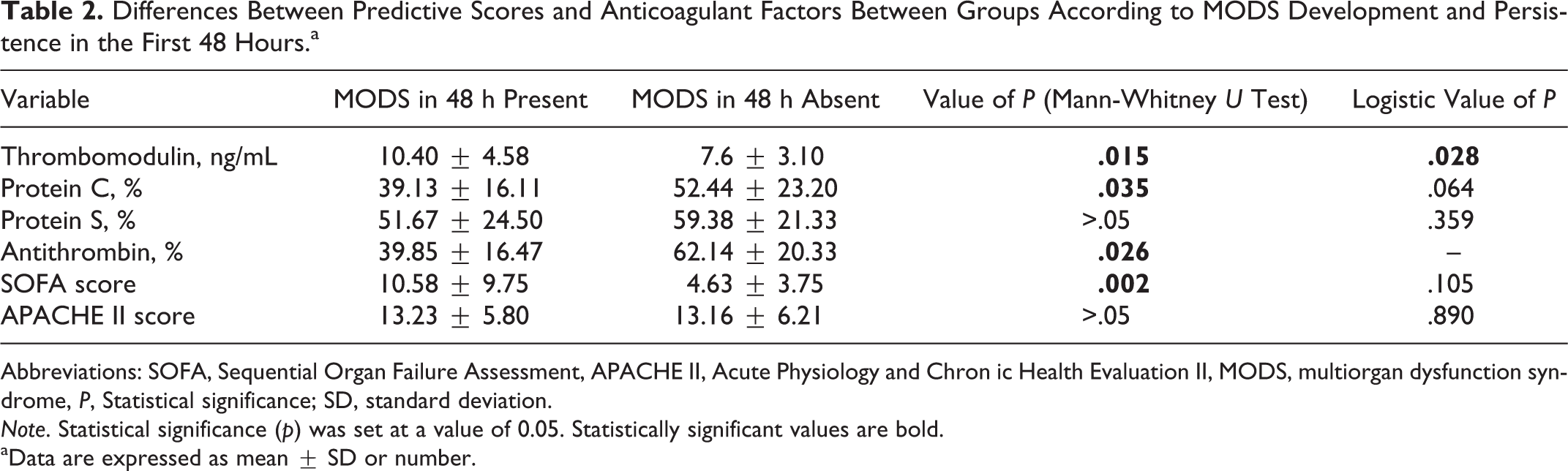
Abbreviations: SOFA, Sequential Organ Failure Assessment, APACHE II, Acute Physiology and Chron ic Health Evaluation II, MODS, multiorgan dysfunction syndrome, P, Statistical significance; SD, standard deviation.
Note. Statistical significance (p) was set at a value of 0.05. Statistically significant values are bold.
aData are expressed as mean ± SD or number.
In order to establish the potential for combinations of anticoagulant markers and predictive ICU scores to improve prediction of MODS development, we first used correlation (Kendall τ). Our results do not show significant correlation between levels of thrombomodulin and other anticoagulant factors, while positive correlation was found between levels of antithrombin and protein C (P < .05) and antithrombin and protein S (P < .05). Level of antithrombin was not included in the model of logistic regression because of these positive correlations. Significant correlation was not obtained between SOFA and APACHE II scores or between these scores and levels of investigated markers.
Direct logistic regression was performed in order to assess the impact of levels of natural anticoagulants and predictive scores on ICU admission on the likelihood that development of MODS would occur within 48 hours from onset of sepsis. The model contained 5 different variables (levels of thrombomodulin, protein C and protein S, as well as SOFA and APACHE II score) as predictors. The full model with all the predictors was statistically significant χ 2 (5, N = 60) = 17.96, P = .003. Model explains between 29.2% and 41.2% of the variance and could classify 78.8% of the cases correctly. Only 1 independent variable gave significant contribution to the model (level of thrombomodulin), and results are shown in Table 2. Thus, level of thrombomodulin on ICU admission has proven to be the strongest predictor in MODS development in the first 48 hours in our model. Although level of protein C was statistically insignificant in our model, its value as a predictor of MODS development was higher than values of APACHE II and SOFA scores (Table 2).
Discussion
Sepsis remains an extreme challenge for treatment despite new therapeutic guidelines. 1,2 The initial manifestation of sepsis can often be misleading due to many nonspecific clinical signs of systemic inflammation. 15 –17 Since time for early resuscitation andgoal-directed therapy are essential in this disease, 18,19 it is very important to diagnose promptly. The deterioration from sepsis to septic shock and sequential MODS develops most often in the first 24 hours. 20 Early recognition of high-risk patients is therefore an imperative because of the need for more aggressive therapeutic approach.
Since endothelial disruption and consequential coagulation disorders are essential in pathogenesis of sepsis, many studies were performed in order to test new therapies that could prevent sepsis-induced coagulopathies. 12 –22 However, only few studies have been focusing on markers of coagulation and endothelial injury as predictors of sepsis severity and indicators of high-risk patients. 14,23
Our results bring evidence that plasma concentrations of thrombomodulin were significantly higher in group of patients with MODS than without MODS, while levels of antithrombin and protein C were significantly lower in patients with MODS development in the first 48 hours than without MODS. Once again, these results highlight the fact from recent studies that protein C anticoagulant pathway plays a major role in controlling microvascular coagulation and inflammation. 6,7 Level of protein S was also decreased in the group of patients with MODS in contrast to patients without MODS, but this difference was insignificant.
Thrombomodulin not only plays an important role in the protein C system, by binding to thrombin and converting it from a procoagulant protease to an anticoagulant enzyme that activates protein C, 24 but also prevents dissemination of procoagulant and proinflammatory molecules, such as complement factors, lipopolysaccharide, high-mobility group protein B1, and probably histones, and by doing that allows these molecules to act locally at the site of injury. 25
The SOFA and APACHE II scores are accepted as valuable method for risk stratification and prognosis of patients with sepsis. 26,27 However, in our study both of these scores were higher in group of patients with severe sepsis than in patients with septic shock on the admission. Our results didn’t show statistically significant difference between patients with and patients without development of MODS in the first 48 hours for APACHE II score, while SOFA score was significantly higher in the group of patients with MODS, but in logistic regression model the SOFA score was also not statistically significant in predicting MODS. Results from our study may imply that these scores were not sufficient enough to predict development of MODS, because none of these scores includes any marker of endothelial functioning. The SOFA score includes the number of platelets, but the integrity of endothelium which is a base of proper organ functioning remains unanalyzed. The level of thrombomodulin, however, not only was able to distinguish more severe form of sepsis course but was also a significant predictor of MODS development in the first 48 hours of sepsis onset. Similar results were obtained in the study by Lin et al, 28 in which levels of serum thrombomodulin were higher in patients with DIC and MODS.
Since soluble thrombomodulin fragments circulate in the plasma and are found at increased levels in conditions other than sepsis that cause ischemic and/or inflammatory endothelial injuries, 24,29,30 we have limited our group of studied patients to exclude any possible significant endothelial damage or systemic inflammation of other etiology but sepsis (excluding criteria).
Therefore, our results suggest that increased level of thrombomodulin found in group of patients with MODS is due to endothelial injury caused by proinflammatory cytokines and endotoxins in the course of sepsis.
Since thrombomodulin expression is downregulated in patients with sepsis, 25,31 which may result in dissemination of procoagulant and proinflammatory molecules and subsequent MODS, new studies are aimed toward appropriate therapeutic approach for this condition. 32 We highly support these studies, but we also want to remind that the molecules that are strongly involved in sepsis and MODS pathogenesis should also serve as biomarkers for identification of high-risk patients, so “the golden hour” would not be missed.
We are aware that this study has some limitations. The first limitation is relatively small number of patients due to 1-year incidence of patients with sepsis treated in Clinical Center of Vojvodina and strict exclusion criteria that had significant impact on sample size. The second limitation of our study is that concentration of natural anticoagulants was measured only initially, although their dynamic during the sepsis evolution would be interesting to evaluate the potential therapeutic strategies.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Noninvasive markers in diagnosing and prognosis of critical illness, Provincial secretariat for science and technological development, Republic of Serbia, Autonomous province of Vojvodina.